- Patients with cN1 (at functional or conventional imaging)
- Patients with de-novo metastatic disease
- Patients with oligo-recurrent disease

The case for treatment of cN1 prostate cancer with radiotherapy and hormone therapy relies on data from the STAMPEDE trial, assessing 157 patients in the control arm. 2 Long-term hormone therapy, either alone or with radiotherapy (as per the local standard of care) was administered to cN1 patients. Failure-free survival was better among patients receiving radiotherapy with an adjusted HR of 0.35 (95% CI 0.19-0.65). Additionally, 2-year failure-free survival was 89% (95% CI 77%-94%) and 64% (95% CI 51%-75%) for radiotherapy and no radiotherapy, respectively.
Surgery for cN1 disease relies on only retrospective evidence, with a high risk of patient selection bias (no standardized indications for surgery), no standardized extent of PLND/use of multi-modal approaches, and mainly based on the use of conventional imaging. The rationale for surgery in the cN1 setting is oncologic control. Work from the NCDB suggests that men receiving some form of local therapy +/- ADT had a significant overall mortality benefit compared to men receiving ADT alone 2. However, when comparing radical prostatectomy +/- ADT vs radiotherapy +/- ADT, there was no difference in survival advantage between the two treatment modalities 3. Of the utmost importance is deciding which cN+ patients should be considered for radical prostatectomy. Gandaglia et al. 4 identified 162 patients with lymphadenopathies treated with radical prostatectomy and lymph node dissection at three referral centers. The primary outcome was clinical recurrence was defined as the onset of metastases detected by conventional imaging. The median follow-up for survivors was 64 months with an 8-yr clinical recurrence-free and cancer-specific mortality-free survival rate of 59% and 80%, respectively. The biopsy grade group and the preoperative nodal burden should identify patients more likely to experience clinical recurrence. As follows is the risk stratification tree assessing 8-year clinical recurrence for prostate cancer patients with clinical lymphadenopathies undergoing radical prostatectomy and lymph node dissection:
Dr. Briganti then discussed a case of a patient with a PSA of 6.71 ng/mL, digital rectal examination suspicious of a right lesion (cT2b), and mpMRI suggestive of a PI-RADS 4 lesion, with no extraprostatic extension and no seminal vesicle involvement. A targeted + systematic biopsy showed two cores positive of ISUP grade group 3 on the right base, as well as 3 targeted cores positive for ISUP grade group 4. A CT scan demonstrated a suspicious right internal iliac lymph node (13 mm) and a bone scan was negative. A 68Ga-PSMA PET/CT showed uptake at the level of the fourth rib. Based on the evidence, the question is how we should treat this patient? Dr. Briganti notes that the highest level of data we have currently for this patient is from STAMPEDE arm H 5. For cM1 patients, the STAMPEDE arm H data showed an 8% absolute OS benefit among low burden disease patients (HR 0.68, 95% CI 0.52-0.90). The low burden is defined as patients with only non-regional lymph nodes or 3 or fewer bone metastases with or without non-regional lymph nodes regardless of axial or extra-axial location and without any visceral/other metastases. In a recent secondary analysis published earlier this year, Ali et al 6 suggested that survival benefit decreased as the number of bone metastases increased, with benefit most pronounced up to 3 bone lesions.
Dr. Briganti notes that there are several open questions in this disease space, including:
- Are these results applicable to M1 patients diagnosed with functional imaging?
- What is the optimal treatment sequencing for these patients?
- Should these patients also receive combination systemic therapy?
- Should these patients receive concomitant imaging-guided treatments to the visible lesions at imaging? What about the lymph nodes?
- Are these results applicable to surgery?
For surgery in the oligometastatic disease space, (i) there are no prospective randomized studies available assessing surgery in oligometastatic prostate cancer, (ii) surgery has been tested in retrospective/prospective registries only (with possible patient selection bias), (iii) no standardized use of post-radical prostatectomy treatments or use of metastasis directed therapies, (iv) there are few data on long-term follow-up, and (v) it is not yet clear if the results obtained by radiotherapy can be applied to a radical prostatectomy series. However, even with the low level of evidence, radical prostatectomy is still practiced in this setting.
The EAU 2021 guidelines give a strong recommendation to offer ADT combined with prostate radiotherapy (using the doses from the STAMPEDE trial) to patients whose first presentation is M1 disease and who have a low volume of disease by CHAARTED criteria. Dr. Briganti notes that based on these statements, there is indirect support for the fact that the outcome of radiotherapy cannot be extrapolated to surgery due to the lack of evidence. In Dr. Briganti’s opinion, the following patients are the optimal candidates for surgery:
- Low volume disease according to CHAARTED criteria/1-3 bone metastases
- Men with cN0 disease
- Gleason grade group 3-4 (versus 5)
- Patients with lower PSA (< 60 ng/mL according to a population-based series)
- Patients responding to neoadjuvant ADT

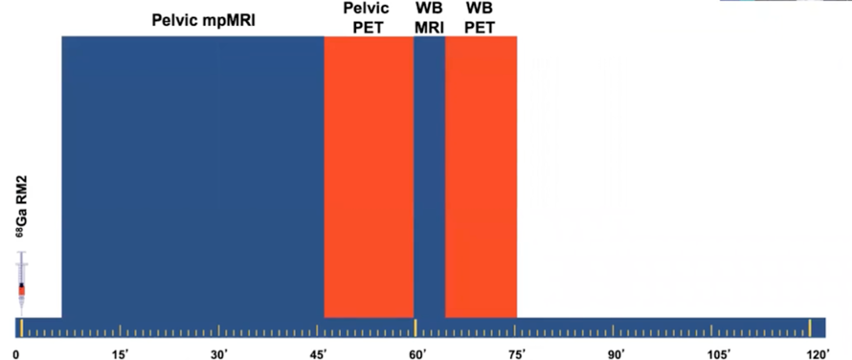
Dr. Briganti then discussed a case of a 58-year-old with intermediate-risk prostate cancer, with a PSA of 11.2 ng/mL, cT2b, Gleason score 4+3 disease. He ultimately underwent radical prostatectomy with left extracapsular extension, 30% tumor volume, 1 mm positive margin on the left, 0/20 nodes positive, Gleason score 4+4, pT3apN0R1. At 6 weeks, his first PSA was <0.001. He initially chose observation, his 9 months PSA was 0.001 ng/mL, his 12-month PSA was 0.11 ng/mL, and his 18-month PSA was 0.38 ng/dL, with a PSA doubling time of 3 months. A PSA PET/CT at this point in time was positive:

According to the 2021 EUA guidelines, this patient should only be offered metastasis-directed therapy to M1 patients within a clinical trial setting or a well-designed prospective cohort study (Strength rating: Strong). As follows is a summary table of the available phase 2 randomized trial data for metastasis-directed therapy from the STOMP, ORIOLE, and SABR-COMET trials:

In the STOMP trial 8, Ost and colleagues randomly assigned 62 patients to either surveillance or metastasis-directed therapy of all detected lesions (surgery or stereotactic body radiotherapy), with a primary endpoint of ADT-free survival. At a median follow-up time of 3 years (IQR 2.3-3.75 years), the median ADT-free survival was 13 months (80% CI 12 to 17 months) for the surveillance group and 21 months (80% CI 14 to 29 months) for the metastasis-directed therapy group (HR 0.60, 80% CI 0.40 to 0.90; log-rank p = 0.11):

The ORIOLE trial 9 randomized 54 men in a 2:1 ratio to receive stereotactic body radiotherapy or observation. The primary endpoint for this trial was progression at 6 months, defined as a PSA increase, radiographic or symptomatic progression, ADT initiation, or death. Progression at 6 months occurred in 7 of 36 patients (19%) receiving stereotactic body radiotherapy and 11 of 18 patients (61%) undergoing observation (p = 0.005). Furthermore, treatment with stereotactic body radiotherapy improved median progression-free survival (not reached vs 5.8 months; HR 0.30, 95% CI 0.11-0.81; p = 0.002):

For those patients in the stereotactic body radiotherapy arm that had a PSMA PET-CT scan, the proportion of men with disease progression at 6 months was 5% in those who did not have any untreated lesions, compared to 38% in those who did have some untreated PSMA avid lesions (p=0.03).
The SABR-COMET study was a randomized, open-label phase 2 study that randomized 99 patients (1:2) to receive either palliative standard of care treatments alone (control group) or standard of care plus stereotactic body radiotherapy to all metastatic lesions (SABR group) 10. Over a median follow-up was 25 months (IQR 19-54) in the control group versus 26 months (23-37) in the SABR group, median overall survival was 28 months (95% CI 19-33) in the control group versus 41 months (26-not reached) in the SABR group (HR 0.57, 95% CI 0.30-1.10; p=0.090). Recently published long-term outcomes of this trial showed durable findings 11. Over a median follow-up of 51 months, the 5-year OS rate was 17.7% in the control group (95% CI 6% to 34%) versus 42.3% in SABR group (95% CI 28% to 56%; stratified log-rank p = 0.006), and the 5-year PFS rate was not reached in the control group (3.2%; 95% CI 0% to 14% at 4 years with last patient censored) and 17.3% in the SABR group (95% CI 8% to 30%; p = 0.001):

In this disease space, Dr. Briganti notes that there are several open questions, including 1) Should we combine metastasis-directed therapy with systemic treatment? 2) Should we treat the local tumor anyway? 3) What is the definition of treatment response after metastasis-directed therapy? 4) How do we follow these patients?
Dr. Briganti concluded his presentation with the following take-home messages:
- Functional imaging has led to a stage migration towards locally advanced and metastatic disease
- Long-term data on treatment-based on functional imaging is lacking
- Image-guided treatments represent novel approaches that require accurate patient selection and long-term follow-up data
- Local treatment of the disease seems to play a crucial role in men with limited systemic dissemination
- What is still unknown is the best combination/sequencing of treatment
Presented by: Alberto Briganti, MD, Ph.D., Department of Urology, Vita-Salute San Raffaele, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 American Urological Association, (AUA) Annual Meeting, Fri, Sep 10, 2021 – Mon, Sep 13, 2021.
References:
- Ventimiglia E, Seisen T, Abdollah F, et al. A systematic review of the role of definitive local treatment in patients with clinically lymph node-positive prostate cancer. Eur Urol Oncol. 2019 May;2(3):294-301).
- James ND, Spears MR, Clarke NW, et al. Failure-free survival and radiotherapy in patients with newly diagnosed nonmetastatic prostate cancer: Data from patients in the control arm of the STAMPEDE trial. JAMA Oncol. 2016 Mar;2(3):348-357.
- Seisen T, Vetterlein MW, Karabon P, et al. Efficacy of local treatment in prostate cancer patients with clinically pelvic lymph node-positive disease at initial diagnosis. Eur Urol 2018 Mar;73(3):452-461.
- Gandaglia G, Soligo M, Battaglia A, et al. Which patients with clinically node-positive prostate cancer should be considered for radical prostatectomy as part of multimodal treatment? The impact of a nodal burden on long-term outcomes. Eur Urol. 2019 May;75(5):817-825.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumor for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.
- Ali A, Hoyle A, Haran AM, et al. Association of bone metastatic burden with survival benefit from prostate radiotherapy in patients with newly diagnosed metastatic prostate cancer: A secondary analysis of a randomized clinical trial. JAMA Oncol. 2021 Apr 1;7(4):555-563.
- Mazzonee, Priesser F, Nazzani S, et al. The effect of lymph node dissection in metastatic prostate cancer patients treated with radical prostatectomy: A contemporary analysis of survival and early postoperative outcomes. Eur Urol Oncol. 2019 Sep;2(5):541-548.
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol 2018 Feb 10;36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomized, phase 2, open-label trial. Lancet. 2019 May 18;393(10185):2051-2058.
- Palma DA, Olson R, Harrow S, et al. Stereotactic Ablative Radiotherapy for Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J Clin Oncol. 2020 Sep 1;38(25):2830-2838.