He began by highlighting the plethora of treatment options available in advanced prostate cancer, ranging for targeting of the androgen axis, to cytotoxic chemotherapy, immunotherapy, checkpoint inhibitors, and radionuclide therapy. These agents may be suitable at many instances across the natural history of prostate cancer.
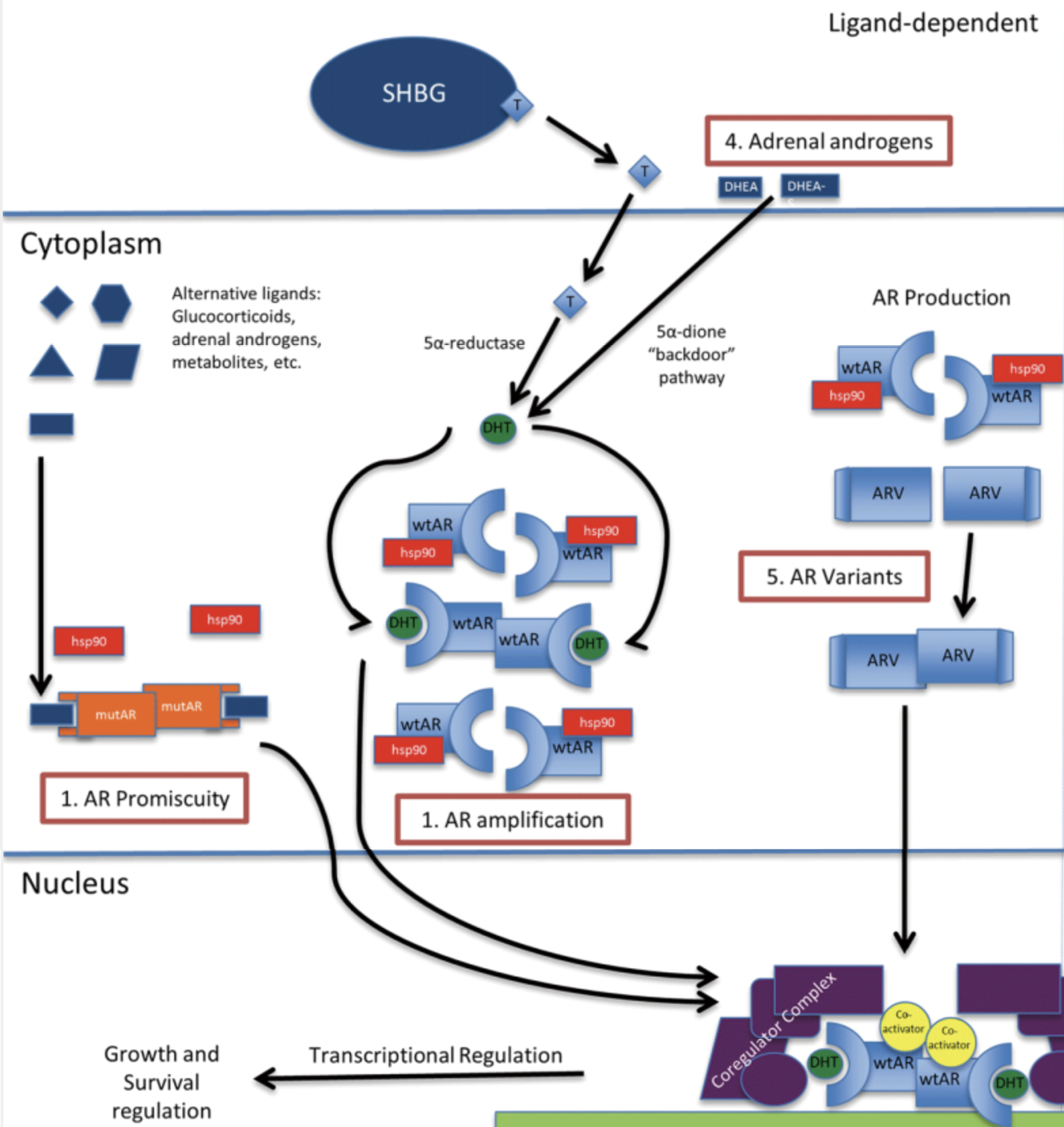
Dr. Jarrard then highlighted a case to emphasize treatment options in advanced prostate cancer. The patient in question had a history of biochemical recurrence following radiotherapy for locally advanced prostate cancer and was started on androgen deprivation therapy (ADT). Three years later, while continuing on ADT, he developed a rising PSA from 8 ng/mL to 21 ng/mL. His testosterone was 19 ng/dL. Conventional imaging was performed demonstrating new pelvic bony metastasis and enlarged pelvic and retroperitoneal lymph nodes. Despite having castration resistant prostate cancer (CRPC), Dr. Jarrard emphasized that this patient is likely to have ongoing androgen receptor activity on the basis of many studies of such patients. Thus, ongoing targeting of the androgen axis remains relevant despite castration resistance. In part, this may be explained by the ligand-dependent mechanisms of CRPC.
Abiraterone acetate, acting as an androgen biosynthesis antagonist at pregnenolone, mechanistically drives increased levels of aldosterone, with the associated toxicity of hypertension and hypokalemia.
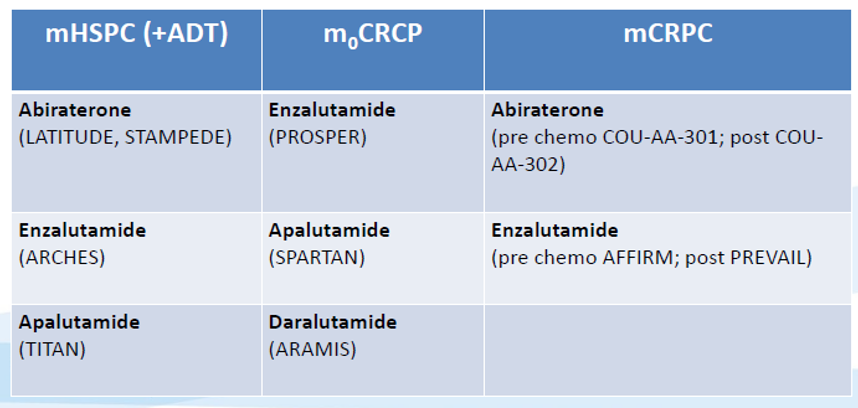
Dr. Jarrard then synthesized the data for the use of abiraterone in advanced prostate cancer. First, he noted the results of COU-AA-301 which, in the post-docetaxel mCRPC space, demonstrated significant overall survival benefits for the use of abiraterone (HR 0.65, 95% CI 0.54-0.77). Subsequently, the COU-AA-302 trial demonstrated a survival benefit (HR 0.53, 95% CI 0.45-0.62) among patients with mCRPC in the pre-chemotherapy setting. In addition to benefits in terms of overall survival, abiraterone improved secondary endpoints including PSA progression, progression-free survival, PSA response rate, and time to opiate use. In terms of toxicity, hypokalemia and hypertension were somewhat increased. However, more notably, Dr. Jarrard emphasized increases in ALT and AST. To minimize the side effects of abiraterone, he suggested it be taken on an empty stomach and co-administered with prednisone (in keeping with its drug monograph). Monitoring of liver function tests and basic metabolic panels is recommended, beginning every 2 weeks, then monthly, and finally quarterly after 3 months.
He then discussed data from LATITUDE and STAMPEDE supporting the role of abiraterone acetate in patients with metastatic castration sensitive disease (mCSPC). The LATITUDE trial enrolled a high-risk group of patients who were hormone naïve and demonstrated significant improvements in cancer progression and overall mortality. Further, patients receiving abiraterone had less pain and delayed the start of cytotoxic chemotherapy.
Thus, summarizing the data for abiraterone, he emphasized that it is indicated for patients with mCRPC whether before or after chemotherapy as well as for those with mCSPC. Additionally, he highlighted that it has been used off-label in nmCRPC. However, side effects including hypertension, hypokalemia, edema, and steroid induced hyperglycemia warrant careful monitoring. Dr. Jarrard suggested that the following patients would be poor candidates for abiraterone: those who cannot tolerate systemic steroids (due to brittle diabetes, gastric ulcer, infection, or other reasons), those with cardiac disease (including heart failure or edema), and those with hepatic dysfunction (such as active viral hepatitis or alcohol abuse).
He then moved to discussing androgen receptor signalling inhibitors, including enzalutamide, darolutamide, and apalutamide. In parallel to the COU-AA-301 trial, the AFFIRM study examined the role of enzalutamide in patients with mCRPC following docetaxel. Similar to abiraterone, use of enzalutamide was associated with improved overall survival (HR 0.63, 95% CI 0.53-0.75). Subsequently, the PREVAIL study showed a benefit to the use of enzalutamide in the pre-chemotherapy mCRPC setting (overall survival HR 0.71, 95% CI 0.60-0.84). In terms of toxicity, Dr. Jarrard emphasized that enzalutamide is associated with fatigue, falls, hot flushes, hypertension, and a small risk of seizures. To manage these, he suggested dose reductions for patients with profound fatigue or those on concurrent CYP2C8 inhibitors. Further, care would be suggested for any patients on medications that would lower the seizure threshold. Summarizing, he emphasized that enzalutamide is indicated for patients with mCRPC whether before or after chemotherapy as well as for those with mCSPC and nmCRPC. Patients with a history of seizure, strokes or falls and those with significant fatigue may be particularly poor candidates.
He then briefly discussed other androgen signalling inhibitors. Apalutamide is mechanistically similar to enzalutamide and is approved in both nmCRPC and mCSPC. While the toxicity profile is generally similar to enzalutamide, additional note of the risk of hypothyroidism and rash is warranted. Darolutamide is structurally distinct but mechanistically similar and indicated in nmCRPC. As a result of its unique structure, it has less penetration of the blood brain barrier and thus, decreased risk of fatigue, seizure, and hypertension.
Dr. Jarrard emphasized that there is little data to guide the decision of which agent to choose first. He did note that the sequence of abiraterone followed by enzalutamide had somewhat better PSA progression compared to the converse approach. However, he particularly emphasized that we should avoid sequencing agents with the similar mechanism of action.
Presented by: David F. Jarrard, MD, Vice-Chair for Clinical Affairs, John P. Livesey Chair in Urologic Oncology, Associate Director, University of Wisconsin Carbone Cancer Center, Madison, WI
Written by: Christopher J.D. Wallis, MD, Ph.D., Assistant Professor in the Division of Urology at the University of Toronto Contact: @WallisCJD on Twitter during the 2021 American Urological Association, (AUA) Annual Meeting, Fri, Sep 10, 2021 – Mon, Sep 13, 2021.