In terms of current guideline principles, he emphasized that imaging can be used to identify the presence of metastatic disease both at initial recurrence and then periodically thereafter. Currently, cross-sectional imaging (CT or MRI) and technetium bone scan are recommended. However, these studies have significant limitations in terms of both their accuracy and also the burden (3-4 hours for a bone scan) and radiation exposure. Beginning first with a CT scan, he emphasized that the strength of this modality is the ability to identify nodal and visceral disease. However, it lacks sensitivity for bony disease and is somewhat limited in the detection of nodal metastasis with a sensitivity <40% and specificity of approximately 80%. The technetium bone scan is highly sensitive for osteogenic activity and imaging the entire skeleton. However, it lacks specificity and has relatively poor sensitivity, particularly when PSA levels are low.
Assuming these “conventional” imaging approaches are negative, novel next-generation imaging using PET-CT may be used and they may also be considered as an alternative to these conventional approaches. However, when conventional imaging is negative, the guidelines recommend observation or clinical trial enrollment.
In the context of non-metastatic castration resistant disease, imaging is recommended every 6 to 12 months, with the interval personalized based on PSA doubling time, symptoms, and other patient-specific factors. However, once androgen-receptor targeted therapy is initiated, imaging is only required annually. The Prostate Cancer Clinical Trials Working Group 3 provides further guidance on imaging in CRPC. CT scan and bone scan are recommended at baseline with MRI or CT of the brain for those with neuroendocrine features. Reimaging should be performed at 3-12 months intervals based on the PSA kinetics and symptoms. Any evidence of apparent worsening on bone scan after starting a new therapy should warrant consideration of flare and be confirmed on repeat imaging. The RADAR III guide provides further recommendations, including on the use of next-generation imaging, stratified by disease state.
RADAR III Guide
(Radiographic Assessments for Detection of Advanced Recurrence)
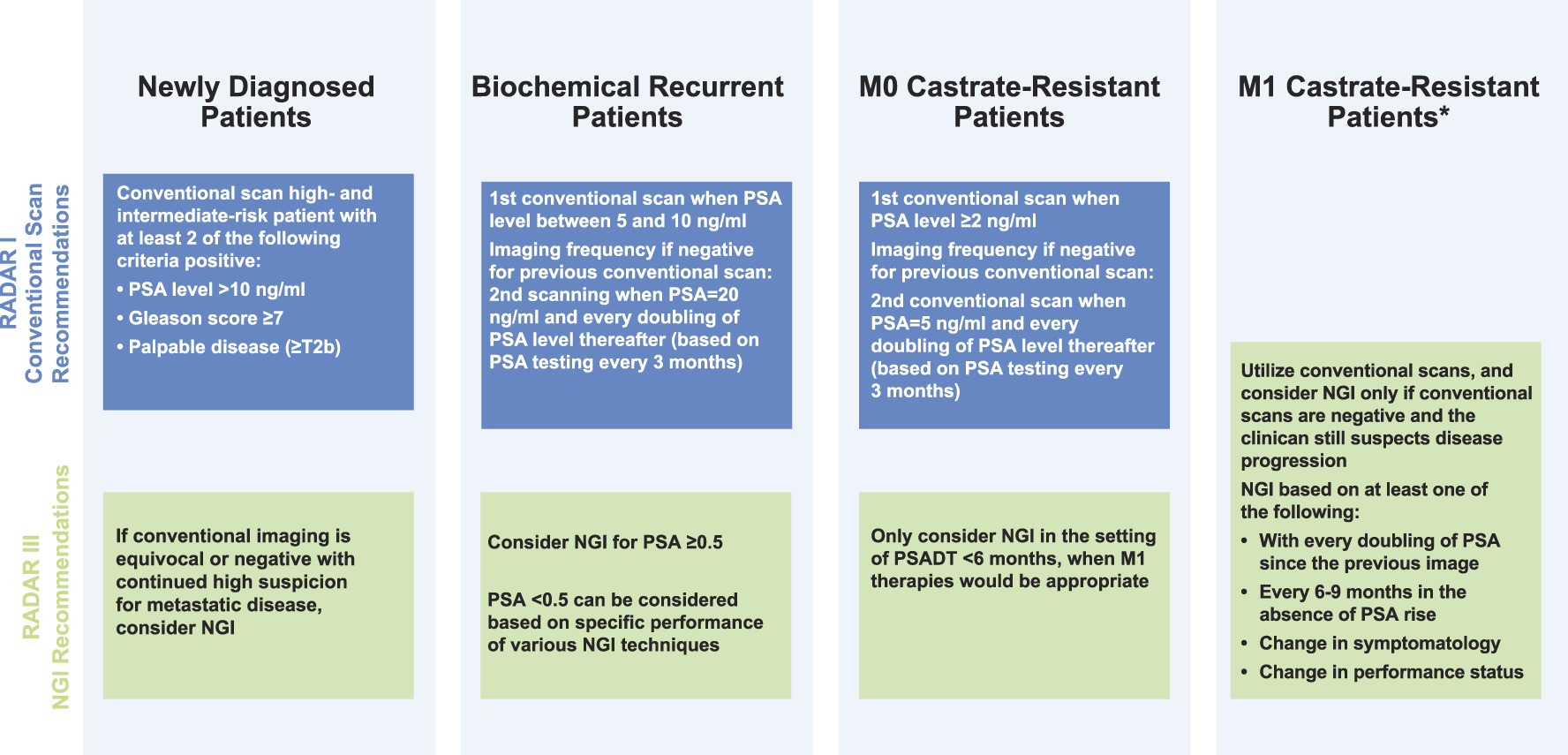
Dr. Stratton then briefly noted that a conventional FDG-PET-CT is of little use in most patients with prostate cancer given the relatively low glucose metabolism of hormone-sensitive prostate cancers. However, other advanced imaging modalities can be considered including PET-CT using F-18 NaF, C-11 choline, F-18 fluorocholine, synthetic amino acid PET radionuclides, and PSMA targeting, as well as whole-body MRI. Dr. Stratton compared the characteristics of a number of the available PET radiotracers.
In the context of the RADAR III recommendations, summaries of each of these advanced imaging approaches are provided. In particular, Ga-68-PSMA and DCFPyL-PSMA appear increasingly clinically relevant.
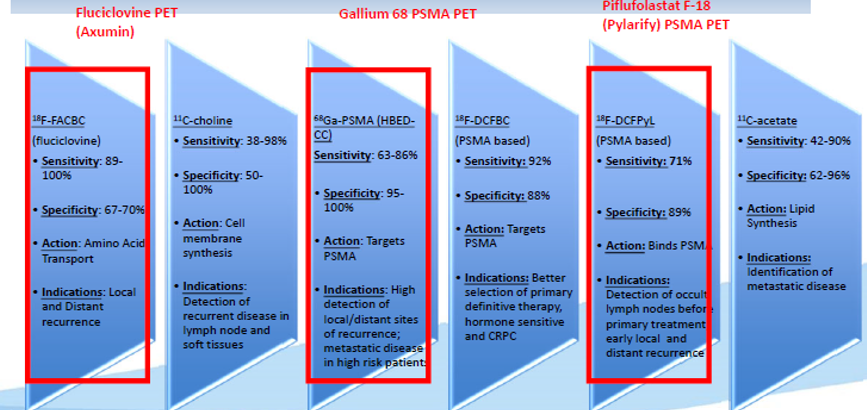
However, Dr. Stratton also reviewed a number of other modalities. Beginning with F-18 NaF PET/CT, he emphasized that this approach has higher bone affinity than technetium bone scan and earlier imaging with improved image quality. However, it has relatively low specificity. A number of imaging approaches have utilized cell membrane-based radiotracers, including C-11 choline, C-11 acetate, and F-18 fluorocholine. The C-11 based of these approaches have the advantages of low excreted urine activity while F-18 fluorocholine has longer half-life.
F-18 fluciclovine, marketed as Axumin, is a synthetic amino acid analog of leucine. It has increased uptake into prostate cancer cells due to their increased metabolism. Additionally, it has minimal urine excretion. This agent is FDA approved for men with suspected recurrence based on increased PSA levels and outperforms the ProstaScint scan. Compared with C-11 choline PET-CT, fluciclovine has similar sensitivity and negative predictive value in the BCR setting but higher specificity and positive predictive value. However, Prostate-Specific Membrane Antigen (PSMA)-based PET/CT outperformed fluciclovine based imaging. PSMA is a transmembrane glycoprotein that is over-expressed on prostate cancer cells. There are a number of different approaches which have been used with PSMA targeting although Ga-68-PSMA and Pylarify-PSMA are the two most clinically relevant currently. Compared with C-11 choline, Dr. Stratton emphasized that PSMA-based imaging is superior, with higher detection rates, particularly at low PSA levels. He highlighted that PSMA based approaches have recently been FDA approved.
Finally, he discussed whole-body MRI. This has the advantage of evaluating bone, viscera, and nodal disease in a single, non-irradiating study. However, this is a technically challenging approach that is not standardized and availability and reimbursement may provide logistic issues as well.
He closed by emphasizing that clinical trials assessing the outcomes of salvage therapy informed by these new imaging approaches are needed to understand how their use affects patient care.
Presented by: Kelly L. Stratton, MD, The University of Oklahoma School of Medicine, Oklahoma City, Oklahoma
Written by: Christopher J.D. Wallis, MD, Ph.D., Assistant Professor in the Division of Urology at the University of Toronto Contact: @WallisCJD on Twitter during the 2021 American Urological Association, (AUA) Annual Meeting, Fri, Sep 10, 2021 – Mon, Sep 13, 2021.