(UroToday.com) Advanced urothelial carcinoma has among the worst prognosis for tumors treated by genitourinary oncologists. Standard of care dictates that patients receive platinum-based induction chemotherapy. However, even with this treatment, rates of recurrence and disease progression are high and overall survival is quite short due to the development of chemotherapy resistance. In the JAVELIN Bladder 100 study which was reported at ASCO 2020 Virtual Annual Meeting and subsequently published, the addition of avelumab, a PD-L1 directed therapy, as first-line maintenance to best supportive care (BSC) demonstrated improvements in overall survival for patients who did not have disease progression during their initial cytotoxic chemotherapy induction. However, the optimal timing for starting avelumab after completing 1L chemotherapy is unknown.
In a podium presentation at the American Urologic Association Annual Meeting, Dr. Srikala Sridhar and colleagues presented results of their post hoc analysis JAVELIN Bladder 100 examining the efficacy of avelumab by duration of treatment-free interval (TFI) from end of 1L chemotherapy.
To briefly summarize, eligible patients had unresectable locally advanced or metastatic urothelial carcinoma that had not progressed with 4-6 cycles of 1L platinum-based chemotherapy. Patients were randomized to receive avelumab + BSC (n=350) or BSC alone (n=350) after a TFI of 4-10 weeks from their last dose of chemotherapy.
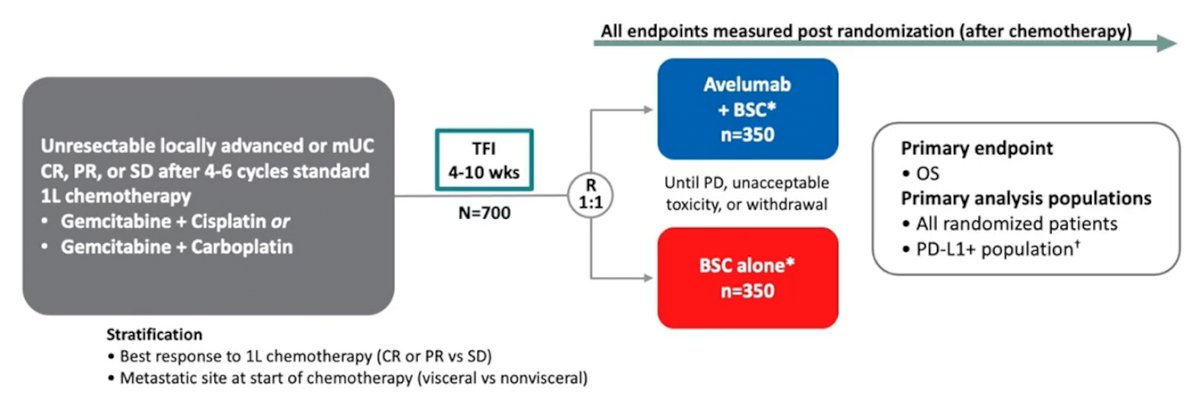
In this exploratory analysis, the authors categorized TFI into subgroups of 4 to <6 weeks (<42 d), 6 to <8 weeks (42 to <56 d), or 8 to 10 weeks (≥56 d).
In the avelumab + BSC and BSC alone arms, TFI was 4 to <6 weeks in 143 and 158 patients, 6 to <8 weeks in 109 and 80 patients, and 8 to 10 weeks in 98 and 110 patients, respectively. Baseline characteristics in subgroups were generally well balanced between arms.
For both arms combined, however, the TFI 4 to <6 weeks subgroup included more patients with visceral metastases (57.8% vs 54.0% and 50.0%), an objective response with 1L chemotherapy (76.4% vs 69.3% and 68.3%), and an ECOG performance status of 1 (44.5% vs 33.3% and 35.6%), compared with the other TFI-defined subgroups.
OS was prolonged with avelumab + BSC vs BSC alone in all subgroups. In the subgroup with TFI 4 to <6 weeks, the HR was 0.76 (95% CI: 0.546, 1.059) (median OS [95% CI], 19.9 months [16.3, 25.3] vs 13.5 months [11.7, 17.4]). Among those with TFI 6 to <8 weeks, the HR was 0.64 (95% CI: 0.404, 1.021) (median OS [95% CI], 26.1 months [19.9, not estimable (NE)] vs 21.0 months [10.7, NE]). Finally, in the TFI 8 to 10 weeks subgroup, the HR was 0.70 (95% CI: 0.468, 1.035) (median OS [95% CI], 20.1 months [13.8, NE] vs 14.1 months [11.7, 19.6]).
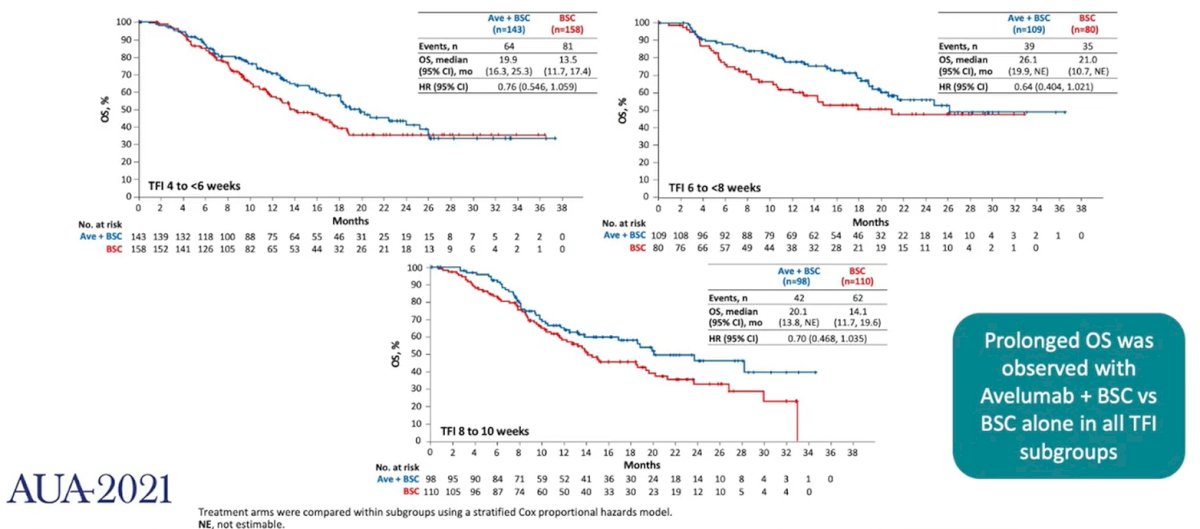
Dr. Sridhar concluded that avelumab 1L maintenance prolonged OS irrespective of the TFI interval (though this was limited to 4-10 weeks in this study context).
Written by: Christopher J.D. Wallis, University of Toronto, Twitter: @WallisCJD during the 2021 American Urological Association, (AUA) Annual Meeting, Fri, Sep 10, 2021 – Mon, Sep 13, 2021.