(UroToday.com) Despite active surveillance being the preferred management option for low-risk prostate cancer, formal guidelines on optimal follow-up are inconsistent and practices vary considerably across treatment centers. At the American Urological Association (AUA) 2020 virtual annual meeting, Dr. Monique Roobol and colleagues presented results of their study describing the risk of upgrading and conversion to treatment among men on active surveillance, according to the intensity of repeat biopsy during follow-up.
This study used the Movember Foundation’s Global Action Plan Prostate Cancer Active Surveillance (GAP3) database, consisting of more than 20,000 men from 27 centers across the world. Inclusion criteria were as follows:
- Diagnosis year ≥1995
- Age <80 years
- cT1-2 disease
- Gleason score ≤6
- PSA<20ng/mL
- ≥9 months of follow-up or ≥1 repeat biopsy on active surveillance
Two centers with only MRI-based re-biopsy and three without follow-up biopsy data were excluded. Men were grouped by their center’s prostate biopsy schedule: High – yearly; Intermediate – biennially; Low - PRIAS protocols (for example at year 1, 4 and 7). Risk of upgrading (Gleason ≥3+4) and transitioning to active treatment (surgery, radiotherapy or hormone therapy) were assessed according to intensity of follow-up schedules using Cox proportional hazards regression, adjusting for age, diagnosis year, PSA, clinical T-stage, number of biopsy cores, and positive cores.
The flow diagram for the study is as follows: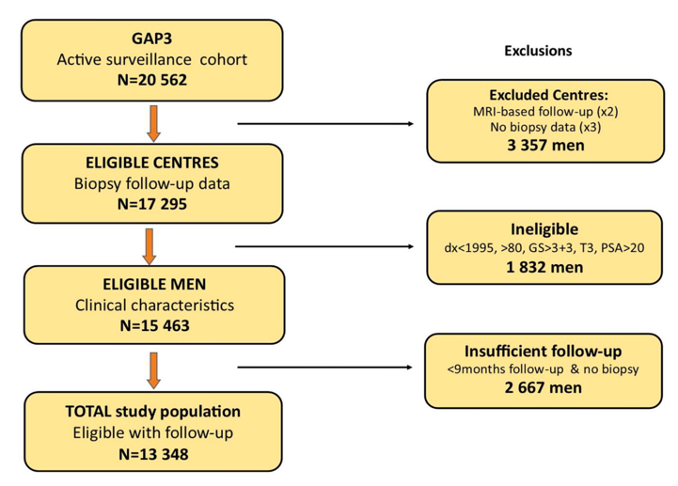
There were 13,348 men from 22 centers contributing to the GAP3 database and followed for a median 35 months. Among these men, 55% were managed at 10 centers with PRIAS biopsy protocols, 33% at 8 centers with biennial biopsy schedules and 12% at 4 centers with annual biopsy schedules. The observed biopsy rates were 34 biopsies per 100 person-years for low, 47 biopsies per 100 person-years for intermediate, and 62 biopsies per 100 person-years for high-frequency groups. The proportions still on active surveillance at 5 years was 62% for low, 62% for intermediate, and 54% for high-frequency groups. Compared with the PRIAS biopsy schedule, an annual biopsy was associated with an increased risk of transitioning to treatment (HR 1.54, 95% CI 1.40-1.70) but was not associated with risk of upgrading (HR 0.99, 95% CI 0.86-1.15).
Several limitations of this study include that (i) variation in protocols for transitioning to treatment across centers is likely to influence findings, and (ii) the authors were unable to determine whether decisions to transition to treatment are based on patient choice or clinician’s recommendations.
Dr. Roobol concludes that there was an increased risk of active treatment among men from centers with annual repeat biopsy schedules, without any similar increased risk of upgrading. Importantly, this indicates higher rates of discontinuation without evidence of upgrading. Further modeling will determine the impact of differing biopsy schedules on delays in detecting disease progression.
Presented by: Monique Roobol, Ph.D., MSc, Professor, Department of Urology, Erasmus University Medical Center Rotterdam, The Netherlands
Co-Authors: Kerri Beckmann, Chris Bangma, Jozien Hellman, Aida Santa Olalla, Daan Nieboer, Anders Bjartell, Peter Carroll, Todd Morgan, Bruce Trock, Riccardo Valdagni, for Movember Foundation's GAP3 Consortium
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2020 American Urological Association (AUA) Annual Meeting, Virtual Experience #AUA20, June 27- 28, 2020