He began his talk showing the Coronavirus phylogenetic tree (Figure 1).
Figure 1- Coronavirus phylogenetic tree with human Coronaviruses shown in red:
Before the COVID-19 pandemic, two other coronaviruses have caused limited outbreaks in the recent past. These include the:
- Severe Acute Respiratory Syndrome (SARS) between 2002-2003
- Middle East Respiratory Syndrome (MERS) between 2012 and the present
SARS began spreading from the Metropole hotel in Hong-Kong, with a total of 8096 reported cases and 774 reported deaths worldwide (Figure 2).
The containment strategies that were used during the SARS spread included two main actions:
Local spread:
- Isolation of cases
- infection control measures
- quarantine Contacts
- hospital and school closures
- Travel advisories
- screening departing airline passengers
- information to passengers arriving from affected areas
Figure 2 – SARS spread: November 1st, 2002-July 31st, 2003: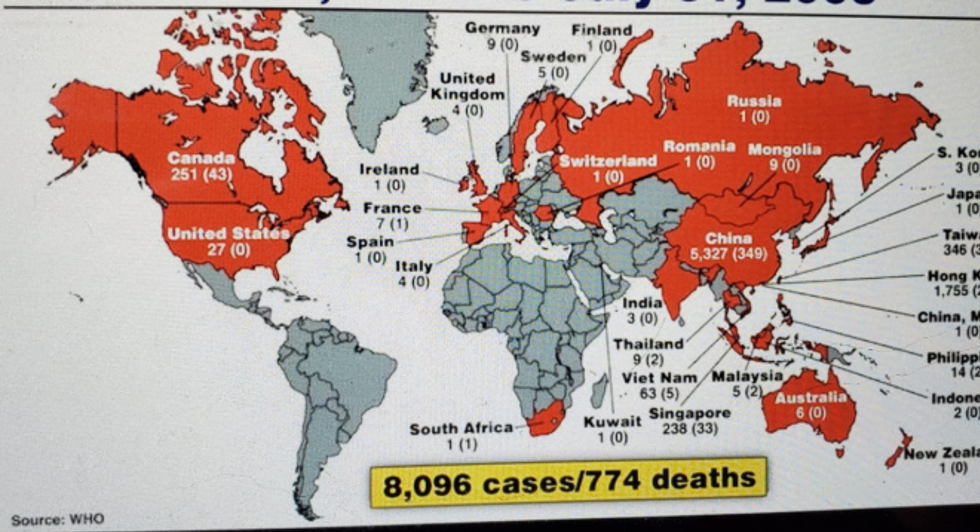
When assessing the spread of MERS, originating from a bat, and transferring to a camel and later on to a human carrier. MERS had a total of 2519 confirmed cases up to 2020, with 886 deaths, resulting in a very high case fatality rate of 37.1%, with 80% of cases in Saudi Arabia (Figure 3).
Figure 3 – MERS global cases 2012-2020:
Dr. Fauci moved on to discuss the current COVID-19 pandemic.
COVID-19 is the name of the disease caused by the novel coronavirus SARS-CoV-2. To date, there are 9.5 million cases in 215 countries and territories, with 483,878 deaths. In the United States, there are 2.46 million cases, with 124,247 confirmed deaths (Figure 4). Most cases in the USA have occurred in the northeast region.
Figure 4 – USA reported COVID-19 cases and deaths: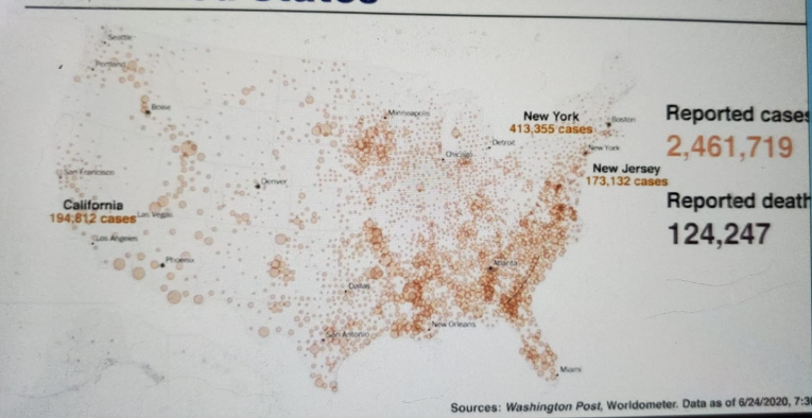
Figure 5 demonstrates the new cases in the United States vs. Europe.
Figure 5 – COVID-19 cases in the US compared to Europe:
Next, Dr. Fauci discussed the virology of the SARS-CoV-2 virus. This is a beta coronavirus in the same subgenus as the SARS virus. It is enveloped, positive-sense single-stranded RNA (+ssRNA) virus with a large genome of 30,000 kilobases. It has 4 structural proteins (S, E, M, N) with the S protein allowing the virus to attach and fuse with the membrane of the host cell. It has an ACE2 cellular receptor (Figure 6).
Figure 6 – SARS-CoV-2 virus:
This virus can cause a direct person to person transmission when in close contact (<6 feet distance) via respiratory droplets. It can also be transmitted through infected surfaces and through aerosol particles (<5 um) that may remain in the air over time and distance. It has been detected in non-respiratory specimens, including stool, blood, ocular secretions, and semen, but their role in transmission is currently uncertain. There is no evidence that animals, including domesticated animals, are a major source of infection in humans.
Data from 16 cohorts with more than 45,000 patients have shown that asymptomatic persons account for ~40-45% of SARS-CoV-2 infections.1 Most patients experience fever (between 83 to 99%), cough in 69 to 82%, fatigue in 44 to 70%, anorexia in 42-84%, shortness of breath in 31 to 40% of cases, and myalgia in 11 to 35% of cases. Other nonspecific symptoms have been reported, including sore throat, nasal congestion, headaches, diarrhea, nausea, vomiting, and loss of smell or taste that can precede the onset of respiratory symptoms.
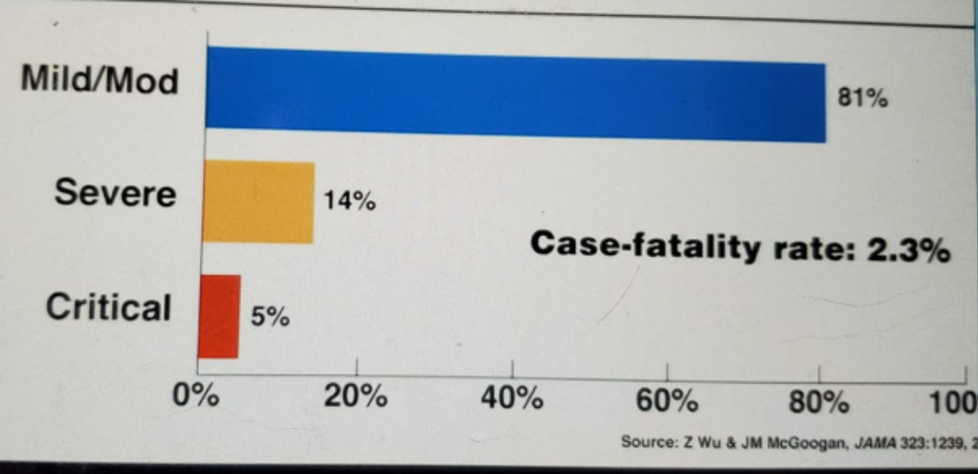
The disease caused by this virus has a wide spectrum of manifestations. This can range from asymptomatic illness with no symptoms whatsoever up to critical illness manifesting in ARDS, sepsis, septic shock, and multiple organ dysfunction or failure, with a case fatality rate of 2.3% (Figure 7).
Figure 7 – Spectrum of COVID-19 disease:
- age above 65 years
- living in nursing homes or long-term care facilities
- hypertension
- Chronic kidney disease
- chronic lung disease
- diabetes
- hemoglobin disorders
- immunocompromised patients
- liver disease
- serious heart disease
- obesity with a BMI of above 40
The cumulative rates of laboratory-confirmed COVID-19 associated hospitalizations by age and race in the USA are shown in Figures 8 and 9, respectively.
Figure 8:
Figure 9:
The manifestations of severe COVID-19 disease include:
- Acute respiratory distress syndrome (ARDS)
- hyper inflammation
- Acute cardiac injury, arrhythmias, cardiomyopathy
- acute kidney injury
- neurological disorders
- hypercoagulability leading to thromboembolic complications, including pulmonary embolism an acute stroke
- multisystem inflammatory syndrome in children (MIS-C)
As of today, there are several available tests for COVID-19, including:
- Molecular tests that detect genetic material
- Antigen tests, detecting proteins from the virus
- Antibody tests, detecting proteins in blood made in response to infection with the virus.
Some of the investigational therapeutics for COVID 19 include remdesivir, broad-spectrum antivirals, convalescent plasma/hyperimmune immunoglobulin, repurposed drugs such as hydroxychloroquine, lopinavir, and ritonavir, host modifiers/immune-based therapies, and anti-SARS-CoV-2 monoclonal antibodies, among others.
Remdesivir had been shown to result in 32% faster time to recovery compared to placebo and might have a survival benefit as well.2
Dexamethasone has been shown to reduce 8-day mortality rate by 35% in ventilated patients and by 20% in other patients receiving oxygen.3
There is an expert United States panel that has developed NIH treatment guidelines for COVID-19, creating a “living document” expected to be updated as often as new clinical data accrue. This document can be found here: COVID19TREATMENTGUIDELINES.NIH.GOV.
Dr. Fauci continued by discussing the public health measures that were taken during this pandemic. These include social and physical distancing orders, stay at home orders, school, venue and non-essential business closures, bans on public gatherings and travel restriction with exit and/or entry screening, aggressive case identification and isolation, alongside contact tracing and quarantine. It is believed that in over three months, shutdown orders and other interventions had averted approximately 16,000,000 COVID-19 infections In the U.S.4 and prevented 3.1 million deaths in 11 countries in Europe.5
The personal preventative measures that are currently recommended include:
- Diligent hand washing
- Avoiding close contact
- Covering mouth and nose with mask or cloth cover
- Covering sneezes and coughs
- Avoidance of face touching
- Regular cleaning and disinfecting of frequently touched objects
In a study assessing physical distancing — comprised of over 172 studies and over 25000 patients — it was shown that over one meter of physical distancing was associated with an 82% reduction in infection, and each additional meter doubled that protection. Masks and respirators reduce the risk of infection by 85%, and the effectiveness was greater in the healthcare setting than in the community. Eye protection also reduced the risk of infection by 78%.
Dr. Fauci concluded his talk by stating that there has been unprecedented collaboration and that there will continue to be resources that will be required to research and develop safe and effective vaccines for COVID-19. Once a successful therapy or vaccine is found, this needs to be manufactured and delivered to the scale of billions of doses to people globally. There are currently several potential vaccine candidates that are in different stages of phase one and phase two studies.
Dr. Fauci also discussed some lessons that have been learned throughout the ongoing COVID-19 pandemic. These include the fact that coronaviruses have pandemic potential — and that novel coronavirus will likely continue to emerge. Good public health measures are critical to controlling an epidemic, as mild presentations of the disease can complicate the control of the epidemic. Importantly, global collaboration and transparency are critical in managing this kind of pandemic. Lastly, experience with prototype pathogens and vaccine platforms can accelerate countermeasure development.
Presented by: Anthony S. Fauci, MD, NIAID Director of the National Institute of Allergy and Infectious Diseases, NIH
Written by: Hanan Goldberg, MD, MSc., Urology Department, SUNY Upstate Medical University, Syracuse, NY, USA, @GoldbergHanan, at the 2020 American Urological Association (AUA) Annual Meeting, Virtual Experience #AUA20, June 27- 28, 2020
References:
- Oran DP, Topol EJ. Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann Intern Med. 2020:M20-3012.
- Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the Treatment of Covid-19 — Preliminary Report. New England Journal of Medicine. 2020.
- Horby P, Lim WS, Emberson J, Mafham M, Bell J, Linsell L, et al. Effect of Dexamethasone in Hospitalized Patients with COVID-19: Preliminary Report. medRxiv. 2020:2020.06.22.20137273.
- Hsiang S, Allen D, Annan-Phan S, Bell K, Bolliger I, Chong T, et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature. 2020.
- Flaxman S, Mishra S, Gandy A, Unwin HJT, Mellan TA, Coupland H, et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature. 2020.