The statement of evidence rating used for the guideline is as follows:
- A (High): Very confident that the true effect lies close to that of the estimate of the effect
- B (Moderate): Moderately confident in the effect estimate, whereby the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
- C (Low): Confidence in the effect estimate is limited, whereby the true effect may be substantially different from the estimate of the effect
- C (Very Low): Very little confidence in the effect estimate, whereby the true effect is likely to be substantially different from the estimate of the effect
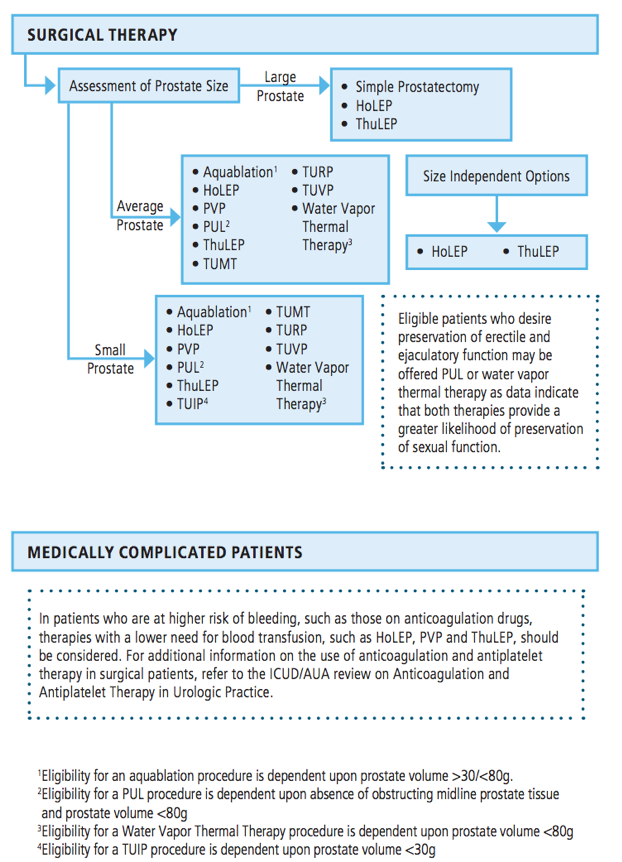
Several additional statements have been amended in the updated guidelines. Guideline Statement 15 states that prostatic urethral lift may be offered as an option for patients with lower urinary tract symptoms attributed to BPH provided the prostate volume is <80 g and verified absence of an obstructive median lobe (Moderate Recommendation, Grade C). Previous information on retreatment rates was removed from this statement and added to the new statement 6 (above). Guideline Statement 16 notes that prostatic urethral lift may be offered to eligible patients who desire the preservation of erectile and ejaculatory function (Conditional Recommendation, Grade C). Guideline Statement 17 states that transurethral microwave therapy may be offered to patients with lower urinary tract symptoms attributed to BPH (Clinical Recommendation, Grade C). Similar to statement 15, information on retreatment rates were removed from this statement and added to the new statement 6.
Guideline Statement 18 states that water vapor thermal therapy may be offered to patients with lower urinary tract symptoms attributed to BPH provided they have a prostate volume <80 g (Moderate Recommendation, Grade C). Information on retreatment was also removed from this statement and added to the new statement 6. Guideline Statement 19 notes that water vapor thermal therapy may be offered to eligible patients who desire the preservation of erectile and ejaculatory function (Conditional Recommendation, Grade C). Of note, no change was made to this statement, however supporting text was updated based on new literature. Guideline Statement 21 states that clinicians should consider holmium laser enucleation of the prostate (HoLEP) or thulium laser enucleation of the prostate (ThuLEP), depending on their expertise with either technique, as prostate size-independent options for the treatment of lower urinary tract symptoms attributed to BPH (Moderate Recommendation, Grade B).
For this statement, the word “suitable” was removed before the word options, and supporting text was updated based on new literature. Guideline Statement 22 notes that aquablation may be offered to patients with lower urinary tract symptoms attributed to BPH provided that the prostate volume is >30g/<80g (Conditional Recommendation, Grade C). Similar to some of the aforementioned statements, information on retreatment rates was removed from this statement and added to a new statement 6. Guideline Statement 23 notes that prostatic artery embolization for the treatment of lower urinary tract symptoms secondary to BPH is not supported by the current data and trial designs, and benefit over risk remains unclear; therefore, prostatic artery embolization is not recommended outside of the context of clinical trials (Expert Opinion).
A summary of the surgical management of the guideline is as follows:
There are enormous gaps in the knowledge and, therefore, ensuing opportunities for discovery. These include but are not limited to many unanswered questions related to the role of inflammation, metabolic dysfunction, obesity, and environmental factors in etiology, as well as the role of behavior modification, self-management, and evolving therapeutic algorithms in both the prevention and progression of disease.
Dr. Kaplan noted that the panel is currently working on the medical management of BPH guideline and algorithm and expect it to be released in 2021. For this guideline, literature was pulled from 2010-December 2019, which included 107 randomized controlled trials observational studies. Certain statements from the 2010 BPH guideline will be incorporated into the 2021 guideline and updated based on the current literature.
Presented by: Steven Kaplan, MD, Director of Men's Health Program, Professor of Urology, Mount Sinai Medical Center, New York, NY, USA
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Augusta, GA, USa, Twitter: @zklaassen_md, at the 2020 American Urological Association (AUA) Annual Meeting, Virtual Experience #AUA20, June 27- 28, 2020.
Related Content:
AUA 2019: AUA Guidelines Update: Surgical Management of BPH