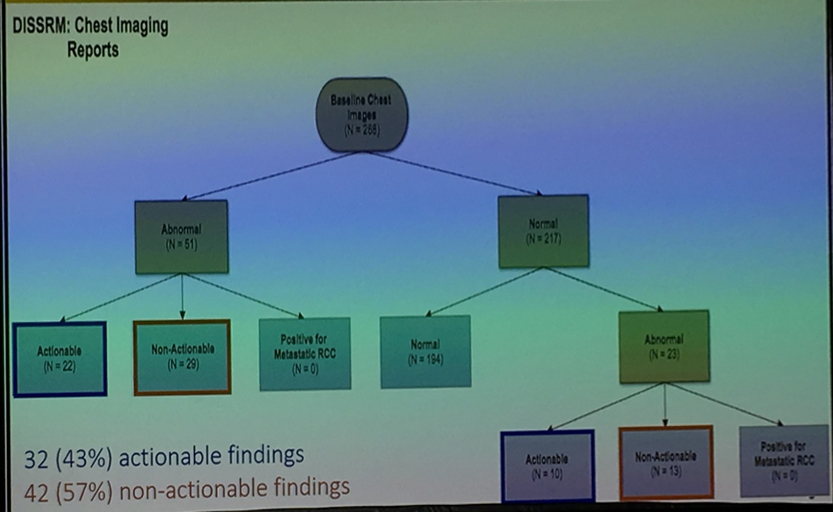
The authors identified 268 eligible patients who received active surveillance for small renal masses at their institution. Of these, 51 patients (19% of the cohort) had identifiable abnormalities on their baseline chest images. The majority of these (29/51, 57%) were not actionable findings while the remaining 22 (43%) lead to intervention either initially or in a delayed fashion. Of the remaining 217 patients who had no discernable pathology on baseline thoracic imaging, 23 patients (11%) developed abnormal findings on repeat imaging. Again, the majority of these did not lead to any interventions (13/23; 57%) while 10 (of 23, 43%) were actionable. Of the 13 patients with new, non-actionable findings (total non-actionable findings n=42), the majority of these were stable pulmonary nodules less than 5mm (n=24) and scarring or post-inflammatory changes (n=8). Among the 10 patients with actionable findings, 32 actionable abnormalities were detected including pulmonary nodules greater than 5mm (n=20) and thyroid nodules (n=8). This led to further investigations including chest CT (n=14), lung biopsy (n=6), and thyroid ultrasound (n=8). None of these investigations identified metastatic renal cell carcinoma.
The authors demonstrate that ongoing thoracic imaging is not associated with the identification of metastatic disease in patients on active surveillance for small renal masses. Thus, the value of these tests must be questioned. The authors argue that yearly thoracic imaging may be indicated in (1) patients with indeterminate pulmonary findings at baseline (for whom ongoing assessment would likely be recommended, even in the absence of a small renal mass); (2) patients with a growing small renal mass (though no data to support this was provided); and (3) patients who opt for surgical intervention for their small renal mass (for whom routine pre-operative chest x-ray is likely to be required for anesthesia).
Presented by: Borna Kassiri, Medical Student, Johns Hopkins School of Medicine, Baltimore Maryland
Co-authors: Joseph Cheaib and Phillip Pierorazio
Written by: Christopher J.D. Wallis, Urology Resident, University of Toronto, @WallisCJD on Twitter at the American Urological Association's 2019 Annual Meeting (AUA 2019), May 3 – 6, 2019 in Chicago, Illinois