Dr. Smith then discussed approaches to prostate biopsy, both in this patient and more generally. With respect to the role of multiparametric magnetic resonance imaging (mpMRI), Dr. Smith highlighted three key considerations: the quality of the mpMRI which may be obtained, the ability of radiologists to interpret the mpMRI, and the ability of the center to act on the information of the mpMRI (ie. the ability to perform targeted biopsy). Further, she highlighted three additional considerations regarding the use of biopsy: the ability to change the biopsy approach or treatment offered, addition information (including an extraprostatic extension or seminal vesical invasion) which may be derived from mpMRI, and the cost/benefit of mpMRI. In this particular patient, she emphasized that, given the physical exam findings, the negative predictive value of mpMRI is not sufficiently high to preclude biopsy regardless of mpMRI findings.
Thus, Dr. Thompson went on to say that the patient underwent a standard 12-core systematic biopsy. This demonstrated Gleason score 4+5 disease in 50-90% of 5/6 cores from the right side of the prostate. These cores demonstrated predominate cribriform pattern with areas of comedo necrosis. The left-sided biopsies were benign. Dr. Lucia highlighted the poor prognostic features of this biopsy, including particularly the cribriform pattern.
Dr. Oto then considered the role of staging imaging beyond standard computed tomography (CT) and bone scan. He highlighted a number of clinical scenarios in which the American Society for Clinical Oncology (ASCO) recommended advanced imaging.
This includes newly-diagnosed high-risk prostate cancer as this patient exhibits. Advanced imaging options he discussed include whole-body MRI, Fluciclovine-Axumin® PET, and PSMA-PET imaging.
The panel then considered treatment options including surgery and radiotherapy.
Dr. Liauw considered radiotherapy approaches and recommended long-term concurrent androgen deprivation therapy and local brachy boost, in keeping with the data from ASCENDE-RT. Additionally, based on the data from patients with locally advanced disease in STAMPEDE, he recommended consideration of the addition of abiraterone and prednisone at this time in the patient’s treatment.


Dr. Davis then considered surgical considerations in this patient. His stated goal was to minimize the morbidity and the number of treatments. Whether already performed or not, he recommended prostate mpMRI for assessment of resectability in patients with high-risk or locally advanced disease. He also highlighted the importance of pre-operative potency assessment. He advocated a non-nerve sparing approach with consideration for a unilateral nerve sparing on the basis of the preoperative potency. Additionally, he recommended careful patient counselling with respect to the need for post-operative radiotherapy.
As the case progressed, Dr. Thompson shared that the patient opted for surgical resection. Final pathology demonstrated T3bN0M0 prostate cancer with a positive surgical margin. The initial post-operative PSA was undetectable. The patient was referred for and underwent adjuvant radiotherapy with two years of concurrent androgen deprivation therapy. Six months following cessation of ADT, the PSA remained undetectable. Two months later, PSA was 0.4 and two subsequent months later the PSA was 1.9ng/mL. Axumin®scan was performed which demonstrated a solitary 3cm nodal mass at the aortic bifurcation. The remainder of staging imaging was negative.
Dr. Klotz then considered the biology of such “oligo-metastatic disease”.
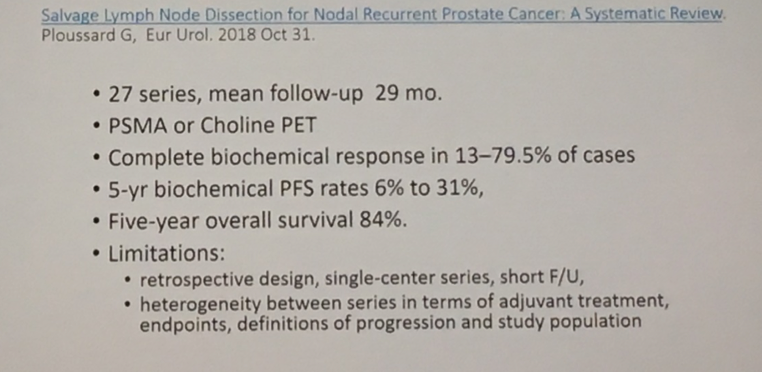
He discussed a recent systematic review by Ploussard and colleagues examined salvage lymphadenectomy for nodal recurrent prostate cancer which demonstrated a highly variable response both in terms of biochemical response and biochemical recurrence free-survival.


Dr. Kuzel then presented the rationale for systemic therapy in this patient. Given the lack of available information on testosterone levels, he highlighted that it was unclear whether this patient was castrate-resistant or castrate-sensitive. In either case, he recommended systemic therapy. On the basis of the data from CHAARTED, he suggested that, as this patient has a low volume of metastatic disease, docetaxel may not necessarily be the preferred approach. Instead, on the basis of the LATITUDE data, he suggested abiraterone may be more appropriate. He also highlighted that genetic testing may be valuable in this patient and may open further systemic therapy options if there is evidence of mismatch repair defects.
Dr. Liauw then discussed the role of radiotherapy in patients with oligo-metastatic disease. In particularly, data using PSMA-PET have demonstrated that the vast majority of patients eligible for salvage radiotherapy have disease limited to the pelvis. Dr. Ost demonstrated, in a phase 2 trial, that metastasis-directed therapy with radiotherapy or surgery could prolong ADT-free survival in patients following initial local therapy.

Thus, Dr. Liauw recommended radiotherapy, including to the local lymph nodes, with concurrent ADT.

This concluded the prostate cancer tumor board discussion.

Presented by: Ian Thompson, Jr., Rodney Davis, Laurence Klotz, Armine Smith, Stanley Liauw, Dr. Aytekin Oto, and Timothy Kuzel
Written by: Christopher J.D. Wallis, Urology Resident, University of Toronto, @WallisCJD on Twitter at the American Urological Association's 2019 Annual Meeting (AUA 2019), May 3 – 6, 2019 in Chicago, Illinois