BPH is a histologic diagnosis with a proliferation of smooth muscle and epithelial cells. The etiology of BPH is still unknown, but LUTS resulting from BPH is quite common, and can tremendously impact patient quality of life.
The current AUA guidelines are the 4th published version and were created by a multi-disciplinary panel consisting of urologists, primary care physicians, and patients. The guidelines emphasize the principle of shared decision making with the patient. The type of guidelines statements is divided into a strong, moderate and conditional recommendation. The rating strength of the evidence includes level A = well-constructed and generalizable randomized controlled trials (RCTs) (High certainty), level B = RCTs with weakness or strong and consistent cohort studies (Moderate certainty), level C = cohort studies with weaknesses or inconsistencies (Low certainty). Additional statement types include:
- Clinical Principle – Widely agreed upon by urologists or other clinicians for which there may or may not be evidence in the medical literature
- Expert Opinion – Achieved by consensus of the panel, that is based on members’ clinical training, experience, knowledge, and judgment for which there is no published evidence.
Surgical therapy is recommended when BPH causes:
- Renal insufficiency
- Refractory urinary retention
- Recurrent urinary tract infections
- Recurrent bladder stones
- Refractory Gross hematuria
- Refractory LUTS
- Unwilling to use other therapies (Clinical principle)
Dr. Breau then described the various modalities available for the surgical treatment of BPH. These include 11 potential therapeutic options that the guidelines discuss:
- Transurethral resection of the prostate (TURP) is still regarded as the surgical gold standard (moderate recommendation, evidence level: grade B). TURP can be performed using either monopolar or bipolar technique.
- Open/laparoscopic or robotic simple prostatectomy can be performed in patients with large prostates, usually greater than 100 cc (moderate recommendation; evidence level grade C).
- Transurethral incision of the prostate (TUIP) should be offered as an option for patients with small prostates (<=30 gr) (moderate recommendation; evidence level grade B).
- Bipolar transurethral vaporization of the prostate (TUVP) may be offered to patients with LUTS attributed to BPH (conditional recommendation, evidence level: grade B).
- Photoselective vaporization of the prostate (PVP) should be considered, using 120 W or 180 W platforms for patients with LUTS attributable to BPH (Moderate recommendation; evidence level: Grade B).
- Transurethral microwave therapy (TUMT) is an optional treatment for BPH, but patients should be informed that that surgical retreatment rates are higher compared to TURP (Conditional recommendation; evidence level: Grade C).
- Prostatic Urethral Lift (PUL) should be considered as an option for patients with LUTS attributed to BPH, as long as these conditions are met:
- Prostate volume <80 cc
- No obstructive middle lobe
- Patients are informed that symptom reduction and a flow rate is improved but not as well when compared to results of TURP
- - Water Vapor Thermal Therapy may be offered to patients provided their prostate volume is smaller than 80 gr; however, patients should be informed that evidence of efficacy, including longer-term retreatment rates, remains limited (Conditional recommendation; evidence level: Grade C). This treatment offers better preservation of erectile and ejaculatory function (Conditional recommendation; evidence level: Grade C)
- - Holmium laser enucleation of the prostate (HoLEP) or thulium laser enucleation of the prostate (ThuLEP) is a size-independent modality and should be considered according to the expertise with either technique of the performing surgeon (Moderate recommendation; evidence level: Grade B).
- - Transurethral needle ablation (TUNA) and prostatic artery embolization are no longer recommended treatments for BPH (Expert opinion for both).
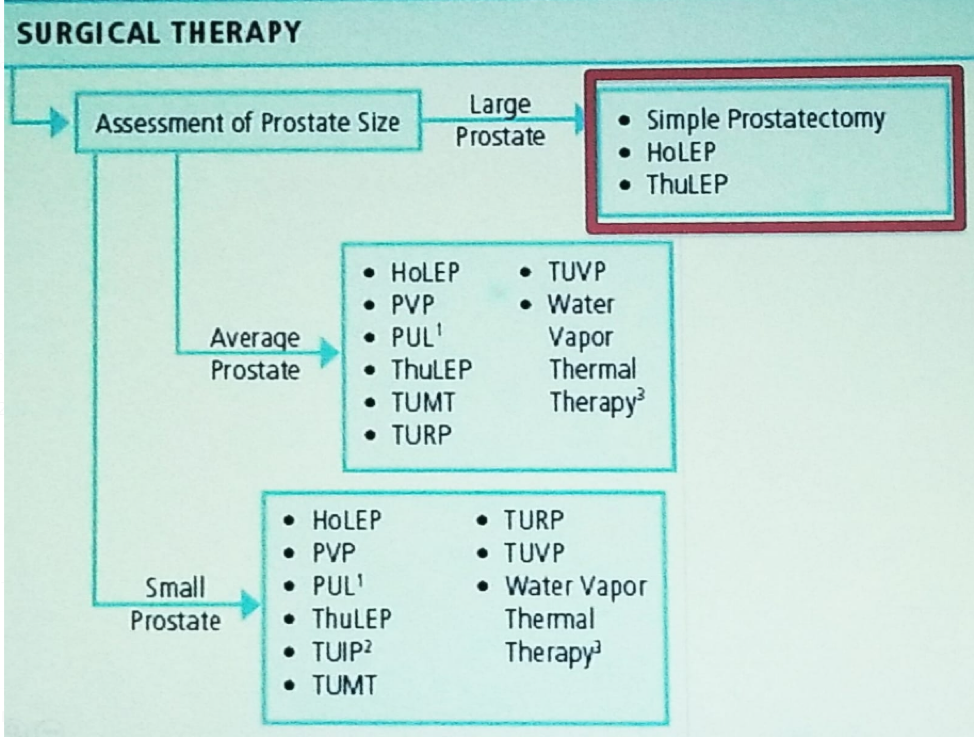
Figure 1- Potential surgical modalities for the treatment of BPH
Presented by: Rodney Breau, MD University of Ottawa, Canada
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, @GoldbergHanan at the 70th Northeastern Section of the American Urological Association (NSAUA) - October 11-13, 2018 - Fairmont Royal York Toronto, ON Canada