(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session QP 13 - GU 7: Quick Pitch: Optimizing Treatment of Recurrent Prostate Cancer. Dr. Piero Bettoli presented abstract 1077 - A Dynamic Treatment Strategy for Oligometastatic CSPC: Integrating Molecular Imaging and SBRT to Personalize Systemic Therapy Intensification and De-Intensification.
Dr. Bettoli opened his presentation by highlighting how PET-PSMA and novel systemic therapies have reshaped the management of oligometastatic castration-sensitive prostate cancer (OM-CSPC), making personalized care feasible. He described the coexistence of two opposing strategies: treatment intensification (continuous androgen deprivation therapy [CADT] plus androgen receptor pathway inhibitor [ARPI] with or without docetaxel) to maximize tumor control, and treatment de-intensification (intermittent androgen deprivation therapy [iADT] plus stereotactic body radiotherapy [SBRT]) to delay systemic therapy and preserve quality of life.
Current approaches typically apply these strategies separately, missing the chance for adaptive integration. He proposed that combining both through PSA- and PET-guided models may optimize treatment response, limit toxicity, and improve resource utilization. The objective is to evaluate whether this dynamic, integrative approach can balance efficacy, safety, and cost-effectiveness while preserving quality of life.
Dr. Bettoli explained that patient selection was restricted to men with OM-CSPC defined as ≤5 lesions, no visceral metastases, and staging with PSMA PET. Structured follow-up was performed every 3 months with PSA and testosterone monitoring, with PSMA PET triggered if PSA rose above 2 ng/mL, either at switch-off or prior to reinitiating intermittent ADT.
Patients start with de-intensification, receiving intermittent ADT (iADT) for 3–9 months plus SBRT to PET-positive lesions, including the primary. iADT is paused if PSA falls to ≤0.2 ng/mL and restarted if PSA rises above 8 ng/mL, with repeat SBRT allowed at the physician’s discretion. A decision node then determines whether to escalate therapy based on three criteria: a PSA nadir >0.2 ng/mL during iADT, PSA doubling time <6 months during the off-treatment interval, or PET evidence of disease progression (>5 lesions or visceral metastases). If escalation is warranted, patients transition to systemic intensification with continuous ADT (cADT) plus an ARPI ± docetaxel, adjusted according to disease volume. The Dynamic strategy schema is shown below.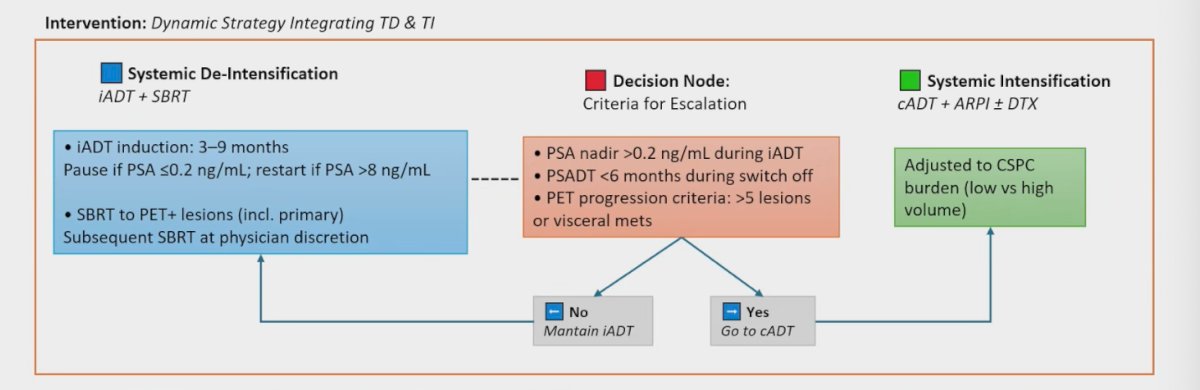
In early results from this adaptive strategy, 33 patients were recruited with a median follow-up of 25 months. CRPC-free survival was 97%, and notably, 81% of patients were able to remain on intermittent ADT, thereby avoiding systemic intensification.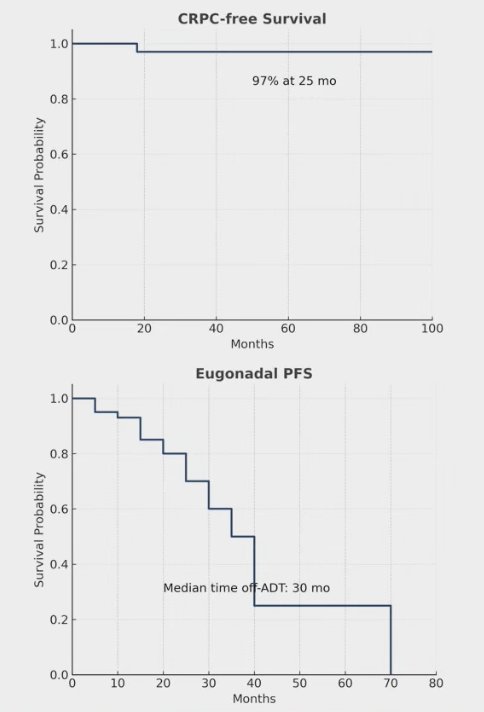
The median off-ADT time was 30 months, reflecting the ability of this approach to delay continuous therapy. The regimen was also well tolerated, with no grade ≥3 toxicities reported, only 3% experiencing grade 2 ADT-related events, and no SBRT-related toxicities of grade ≥2. These findings suggest the feasibility and safety of integrating de-intensification and intensification strategies in a dynamic manner.
The study also incorporated a cost-effectiveness analysis comparing the dynamic strategy (treatment de-intensification followed by escalation when needed) versus a continuous treatment intensification approach (cADT + ARPI ± docetaxel). The dynamic model resulted in a ~40% cost reduction (US$255,000 vs US$405,000), largely driven by the decreased use of systemic therapies such as ARPIs and docetaxel. This highlights the potential economic advantage of tailoring treatment based on disease biology and structured monitoring rather than applying continuous intensification across all patients.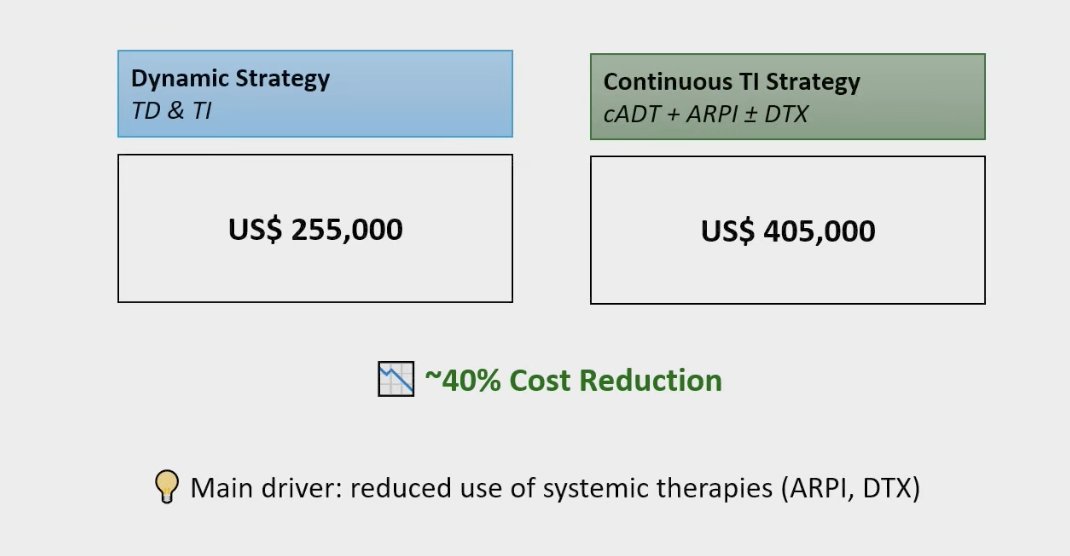
Dr. Bettoli wrapped up his presentation with the following remarks:
- Integrating treatment intensification and treatment de-intensification provides a feasible, effective approach for OM-CSPC.
- This strategy balances tumor control and quality of life preservation while adapting to disease progression and individual needs.
- PSMA PET molecular imaging enables personalized treatment selection.
- SBRT plays a pivotal role in prolonging systemic therapy-free intervals and delaying systemic therapy escalation, optimizing interventions and resource use.
- This model improves both clinical outcomes and cost efficiency, offering a transformative approach to metastatic CSPC management.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.