(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session QP 13 - GU 7: Quick Pitch: Optimizing Treatment of Recurrent Prostate Cancer. Dr. Giulio Francolini presented abstract 1076 - Early Results from a Randomized Phase II Trial Testing Apalutamide and Stereotactic Body Radiation Therapy for low-burden metastatic hormone-sensitive prostate cancer (NCT05717660).
Dr. Francolini highlighted that apalutamide combined with ADT has been shown to significantly improve overall survival in both low- and high-volume metastatic hormone-sensitive prostate cancer (mHSPC) compared to ADT alone.1 He referenced the ARTO phase II trial, which demonstrated that stereotactic body radiotherapy (SBRT) improved outcomes when given with abiraterone in metastatic castration-resistant prostate cancer (mCRPC).2 However, evidence supporting the role of SBRT in addition to androgen receptor pathway inhibitors (ARPIs) in oligometastatic HSPC remains limited. The ongoing PERSIAN trial is designed to test whether metastasis-directed SBRT can further improve outcomes in patients with oligometastatic mHSPC treated with apalutamide plus ADT.
The study schema is presented below. Notably, patients with metachronous oligometastatic hormone-sensitive prostate cancer (≤5 metastases amenable to SBRT) are randomized to receive apalutamide plus ADT alone or in combination with stereotactic body radiotherapy to all metastatic sites. Exclusion criteria include visceral metastases and de novo metastatic disease. The primary endpoint is the proportion of patients achieving complete biochemical response (PSA <0.2 ng/mL) at 6 months, the current analysis focusing on biochemical response at 3 months after initiation of apalutamide plus ADT. Secondary endpoints include PSA and radiographic progression-free survival, treatment-emergent adverse events, overall and cancer-specific survival, and quality of life.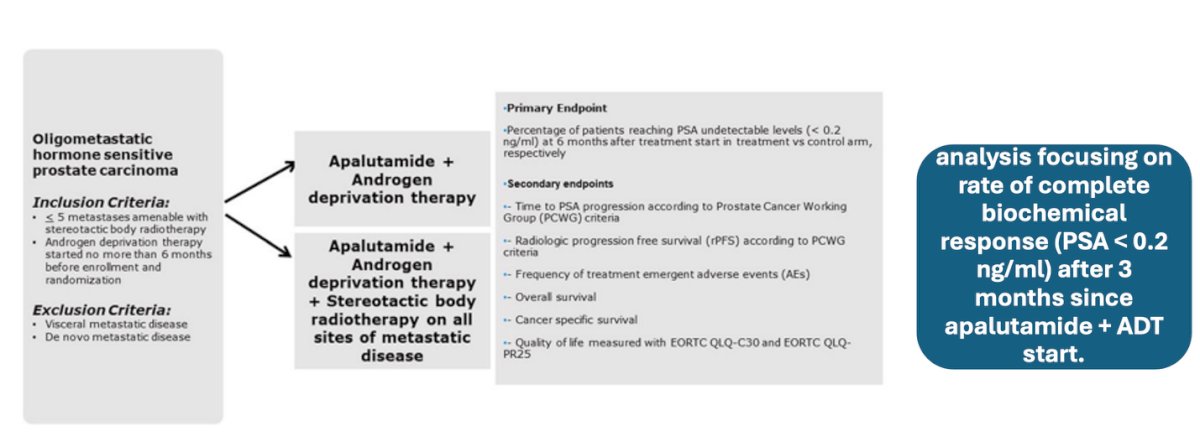
Baseline characteristics showed a median age of 73–74 years and baseline PSA around 1 ng/mL across both arms. Most patients had one or two metastatic lesions (87%), with bone being the predominant site (64%), followed by nodal-only disease (36%). PSMA versus conventional imaging discrepancies were noted in 18% overall, slightly more common in the apalutamide-only arm (24.5%) compared to apalutamide plus SBRT (11.9%). Patients were stratified by prior pelvic or prostate bed radiotherapy and the presence of locoregional disease, defined as pelvic nodes <2 cm.
A total of 180 patients have been enrolled in the trial, with 87 having at least 3 months of follow-up at the time of analysis. The rate of complete biochemical response (PSA <0.2 ng/mL) was comparable between the control and experimental arms, 91.1% versus 92.9%, respectively (OR 1.27; 95% CI 0.27–6.03; p=0.765). Importantly, neither the presence of PSMA-positive lesions undetected on conventional imaging nor the presence of bone metastases had a significant impact on achieving a complete biochemical response.
However, when outcomes were adjusted for the number of metastatic sites, a significant benefit emerged in favor of the experimental arm among patients with fewer than three metastases. In this subgroup, the odds of achieving a complete biochemical response were nearly six-fold higher (OR 5.88, 95% CI 1.13–33.3; p=0.03), highlighting the potential value of metastasis-directed therapy in carefully selected patients.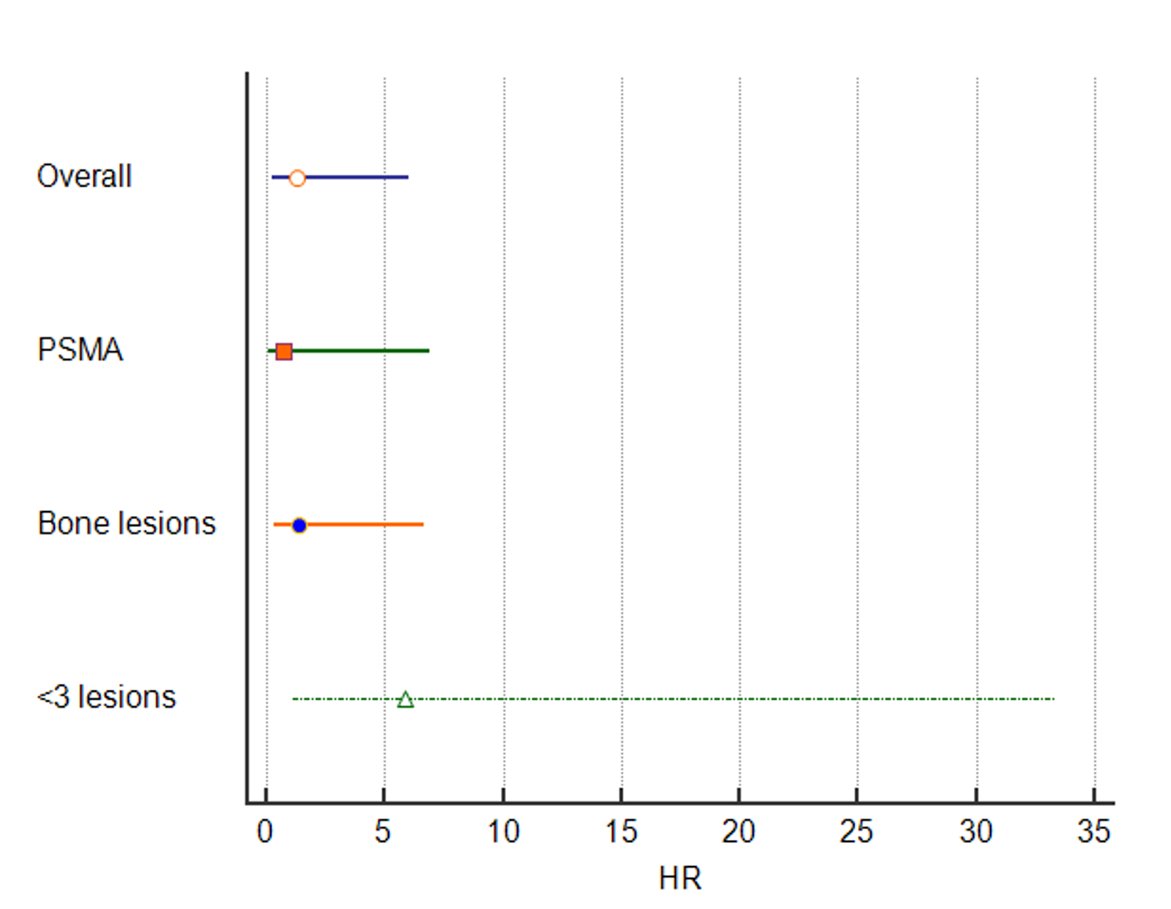
Adverse events were generally mild and consistent with the known safety profile of apalutamide. The most common events included hot flashes, skin disorders, fatigue, and arthralgia (adverse events are summarized below). Importantly, the addition of SBRT did not result in additive toxicity, with the safety profile of the combination arm remaining comparable to apalutamide alone.
Dr. Francolini concluded his presentation with the following key takeaways:
- Early complete biochemical response showed a non-significant trend favoring the experimental arm, with a 27% odds increase for patients receiving SBRT.
- The clinical benefit of SBRT was most pronounced in patients with a lower disease burden (<3 metastatic lesions).
- Adverse events were mild and largely consistent with the known tolerability profile of systemic therapy.
- Trial accrual was completed in December 2024, with the primary endpoint analysis expected in early 2026.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.
References:
- Chi KN, Chowdhury S, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, Juárez A, Merseburger AS, Özgüroğlu M, Uemura H, Ye D, Brookman-May S, Mundle SD, McCarthy SA, Larsen JS, Sun W, Bevans KB, Zhang K, Bandyopadhyay N, Agarwal N. Apalutamide in Patients With Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J Clin Oncol. 2021 Jul 10;39(20):2294-2303. doi: 10.1200/JCO.20.03488. Epub 2021 Apr 29. PMID: 33914595.
- Francolini G, Allegra AG, Detti B, Di Cataldo V, Caini S, Bruni A, Ingrosso G, D'Angelillo RM, Alitto AR, Augugliaro M, Triggiani L, Parisi S, Facchini G, Banini M, Simontacchi G, Desideri I, Meattini I, Valicenti RK, Livi L; ARTO Working Group members. Stereotactic Body Radiation Therapy and Abiraterone Acetate for Patients Affected by Oligometastatic Castrate-Resistant Prostate Cancer: A Randomized Phase II Trial (ARTO). J Clin Oncol. 2023 Dec 20;41(36):5561-5568. doi: 10.1200/JCO.23.00985. Epub 2023 Sep 21. PMID: 37733977.