(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco, was host to the Genitourinary Cancer, Patient Safety, Nursing/Supportive Care session. Dr. Dustin Boothe presented the poster: ProstACT Global: A Phase 3 Study of Lutetium (Lu177) Rosopatamab Tetraxetan plus Standard of Care vs. Standard of Care Alone in Patients with Metastatic Castration-Resistant Prostate Cancer (mCRPC).
Dr. Boothe began by introducing 177Lu-rosopatamab tetraxetan, a radio-antibody drug conjugate (rADC) targeting PSMA-expressing mCRPC. This therapy leverages a PSMA-directed monoclonal antibody, a validated theranostic target, to deliver targeted radiotherapy. It has demonstrated anti-tumor activity and an overall survival benefit in clinical testing.1,2
To date, 177Lu-rosopatamab has been evaluated in more than 240 patients across eight phase 1/2 studies. Notably, published data reported a median overall survival of 42.3 months in heavily pretreated patients with two lines of treatment in the mCRPC setting, underscoring its potential as a novel therapeutic option in this space.1
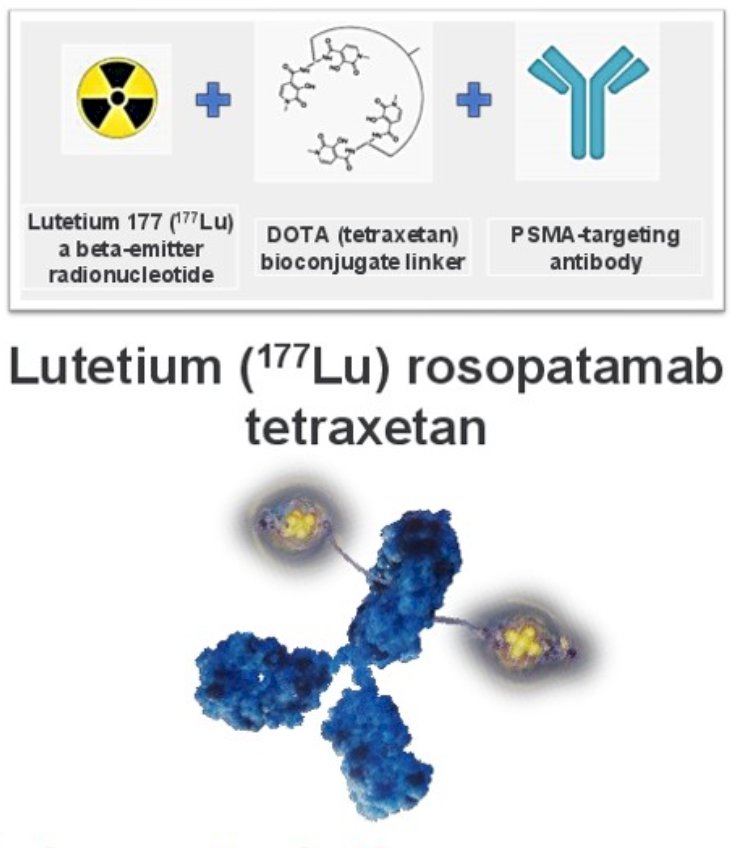
177Lu-rosopatamab tetraxetan (shown below) is a radio-antibody drug conjugate (rADC) that combines three key components: lutetium-177, a beta-emitting radionuclide; a DOTA (tetraxetan) bioconjugate linker; and a PSMA-targeting monoclonal antibody. This design enables targeted delivery of radiation to PSMA-expressing prostate cancer cells, aiming to maximize anti-tumor activity while limiting off-target toxicity.
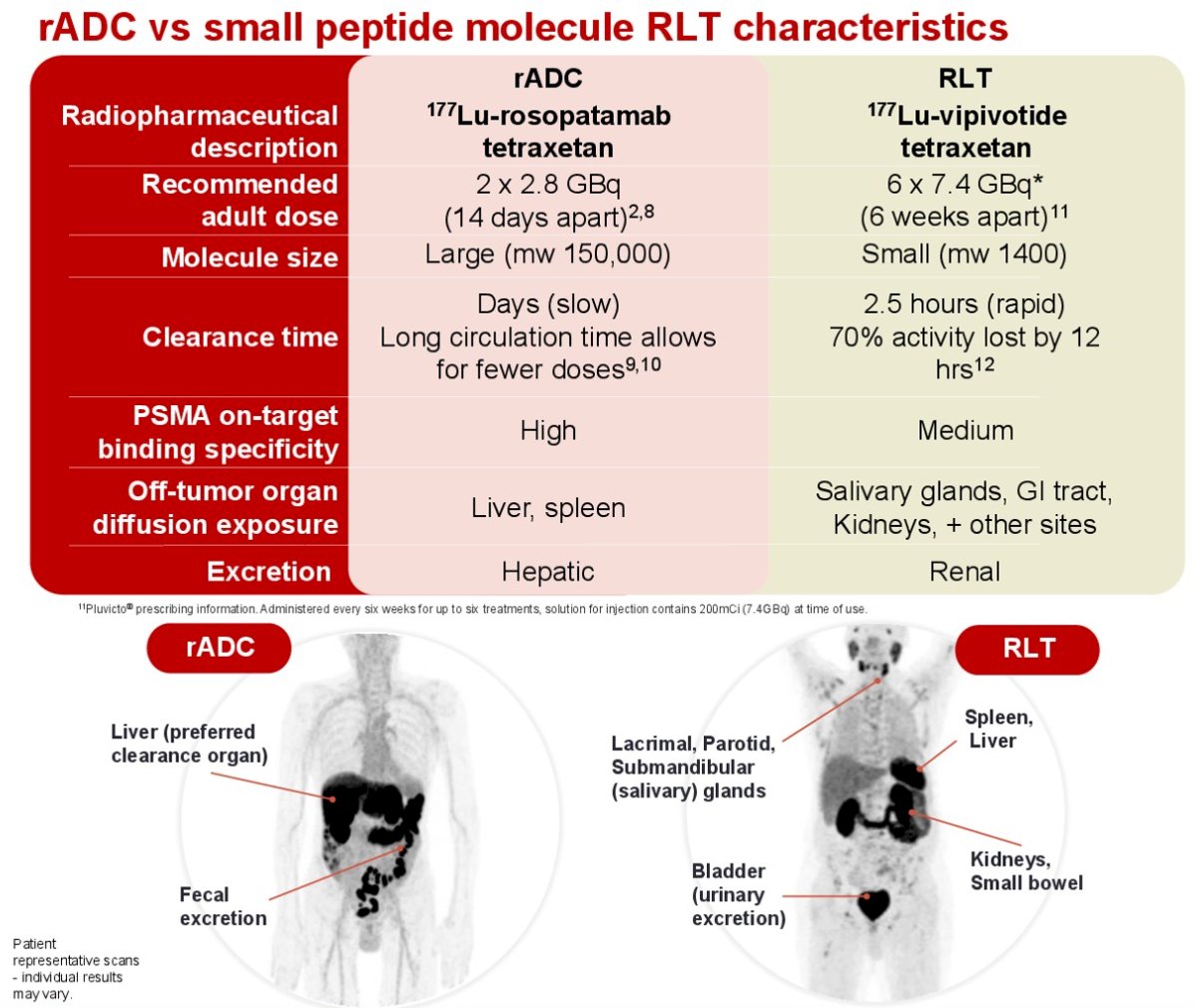
177Lu-rosopatamab tetraxetan differs substantially from small peptide-based radioligand therapies such as 177Lu-vipivotide tetraxetan. The rADC has a large molecular weight (~150,000) with slow clearance, allowing for fewer doses (2 × 2.8 GBq, 14 days apart) compared to the smaller peptide-based agent (~1,400), which requires six cycles (7.4 GBq every 6 weeks) due to rapid clearance (half-life ~2.5 hours). Rosopatamab demonstrates high PSMA binding specificity, with primary off-target exposure in the liver and spleen, and is excreted hepatically. In contrast, peptide-based therapy shows medium binding specificity, broader off-target uptake in salivary glands, GI tract, kidneys, and other organs, and is excreted renally. These pharmacologic differences highlight potentially distinct safety and efficacy profiles between rADC and small peptide PSMA-targeted therapies.
PostACT Global is a prospective, open-label phase 3 trial (NCT06520345) enrolling 520 patients with PSMA-positive mCRPC, confirmed by 68Ga-PSMA-11 PET/CT. Eligible patients must have experienced disease progression after at least 12 weeks of prior therapy with one androgen receptor pathway inhibitor (abiraterone, apalutamide, darolutamide, or enzalutamide), administered in the mCSPC, mCRPC, or both settings. Patients previously treated with docetaxel for mCSPC are permitted, provided their last dose was given at least six months before trial screening.
Notably, the PostACT trial is divided into two parts. Part 1 is a safety and dosimetry lead-in (n=30) designed to characterize the biodistribution and safety profile of 177Lu-rosopatamab tetraxetan in combination with standard-of-care (SOC) therapy. Patients are assigned to abiraterone, enzalutamide, or docetaxel, with fractionated dosing of 177Lu-rosopatamab given two weeks apart.
Part 2 is the randomized treatment expansion (n=490), where patients are randomized 2:1 to 177Lu-rosopatamab tetraxetan plus SOC versus SOC alone. The primary endpoint is radiographic progression-free survival (rPFS), with key secondary endpoints including overall survival. Other secondary measures include objective response rate (ORR), skeletal-related events (SSE), PSA response, and health-related quality of life (HRQoL). Stratification factors include SOC choice (docetaxel or ARPI) and prior docetaxel exposure.

Eligibility criteria for the ProstACT Global study are summarized below:

Moreover, patients were excluded if they had prior exposure to the monoclonal antibody HuJ591 or any other PSMA-targeted radioligand therapy, or if they had received chemotherapy in the first- or second-line mCRPC setting (though prior taxane use in mCSPC was permitted). Exclusion also applied to those with pathologic findings consistent with small cell carcinoma or non-adenocarcinoma histology, except for minor neuroendocrine elements.
Additional criteria included the presence of another malignancy likely to affect survival or interfere with disease assessment, increased risk of hemorrhage or a recent thromboembolic event, known brain metastases or hepatic metastases >1 cm, history of stroke or seizure within six months, or prior treatment with PARP inhibitors or platinum-based chemotherapy.
Presented by: Dustin Boothe, MD, Radiation Oncologist, System Co-Leader of Theranostics, Intermountain Health, Director of Theranostics Research, Intermountain Health, Director of Radiopharmaceuticals, Utah Cancer Specialists, Salt Lake City, UTWritten by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC) Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025
Reference:
- Tagawa ST, Vallabhajosula S, Christos PJ, Jhanwar YS, Batra JS, Lam L, Osborne J, Beltran H, Molina AM, Goldsmith SJ, Bander NH, Nanus DM. Phase 1/2 study of fractionated dose lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 (177 Lu-J591) for metastatic castration-resistant prostate cancer. Cancer. 2019 Aug 1;125(15):2561-2569. doi: 10.1002/cncr.32072. Epub 2019 Apr 23. PMID: 31012963.
- Bander NH, Milowsky MI, Nanus DM, Kostakoglu L, Vallabhajosula S, Goldsmith SJ. Phase I trial of 177lutetium-labeled J591, a monoclonal antibody to prostate-specific membrane antigen, in patients with androgen-independent prostate cancer. J Clin Oncol. 2005 Jul 20;23(21):4591-601. doi: 10.1200/JCO.2005.05.160. Epub 2005 Apr 18. PMID: 15837970.