(UroToday.com) The 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting held in San Francisco, CA between September 28th and 30th, 2025, was host to a bladder and post-prostatectomy radiation session. Dr. Kent Mouw delivered the discussant for the following six abstract presentations addressing bladder and post-prostatectomy radiation therapy:
SCIMITAR and POP-ART are two prospective trials evaluating post-operative SBRT to the prostate bed. Both trials included 100 patients, delivered SBRT in 5 fractions (30-34 Gy), and the median pre-radiotherapy serum PSA level was 0.3 ng/ml.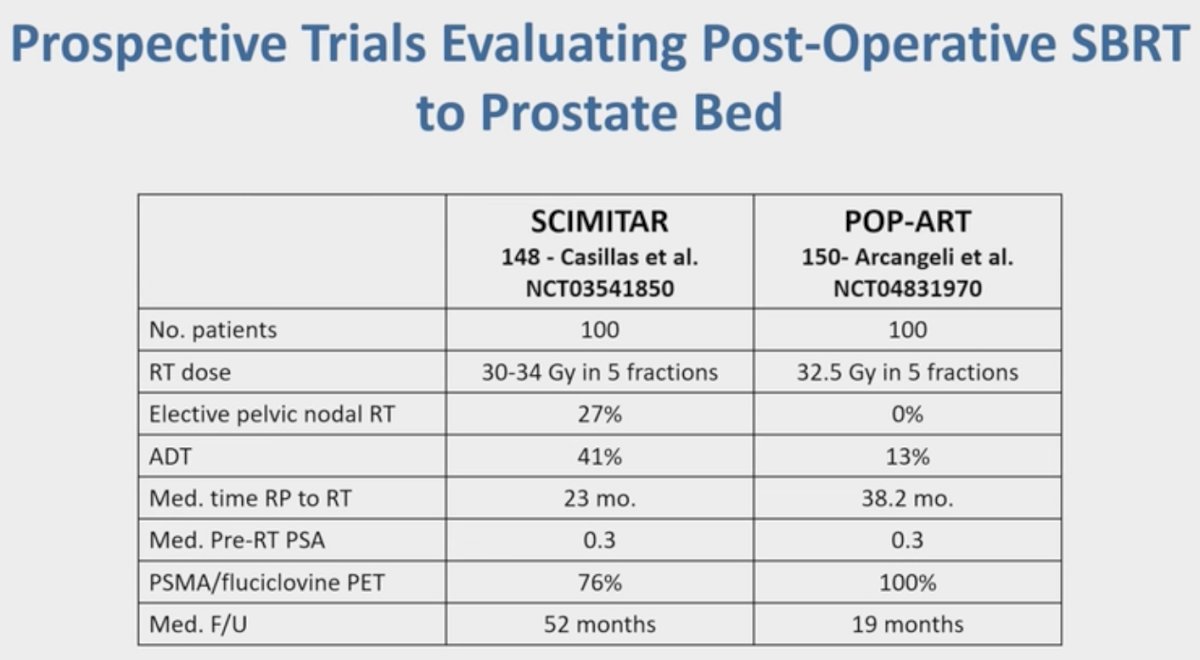
The early efficacy results demonstrated that the 4-year biochemical recurrence-free survival (BC-RFS) in the SCIMITAR trial was 62%, which was similar to that observed in the conventionally fractionated post-operative radiotherapy trial, GETUG-AFU 16.1 In the POP-ART trial, the two-year BC-RFS was 79%.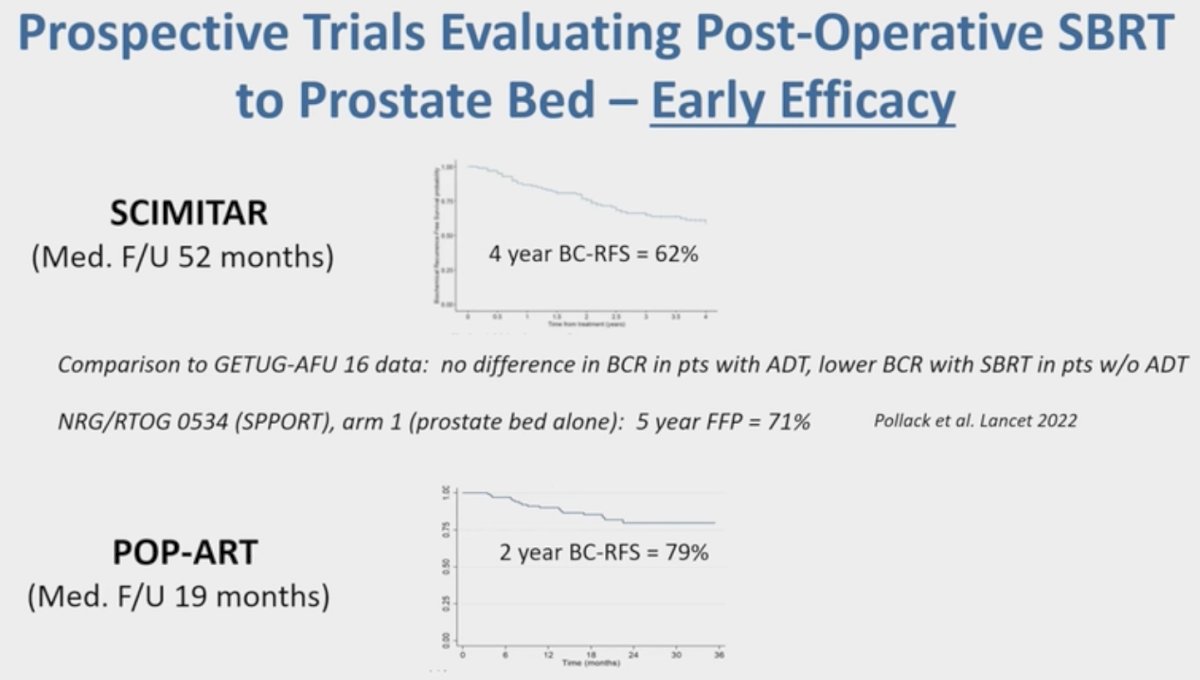
With regards to toxicity, late grade ≥2 GU events were observed in 31% of patients in the SCIMITAR trial and late grade ≥2 GI events in 6.2% of patients. The corresponding proportions in the POP-ART trial were 7.5% and 1.1%, respectively. There was a 23-24% decline in urinary incontinence post-radiotherapy in both arms. While these results appear favorable, Dr. Mouw highlighted that length of follow-up matters, and grade ≥3 toxicities do not occur until >2 years of follow-up, as evidenced in the NRG GU-003 and HYPORT trials.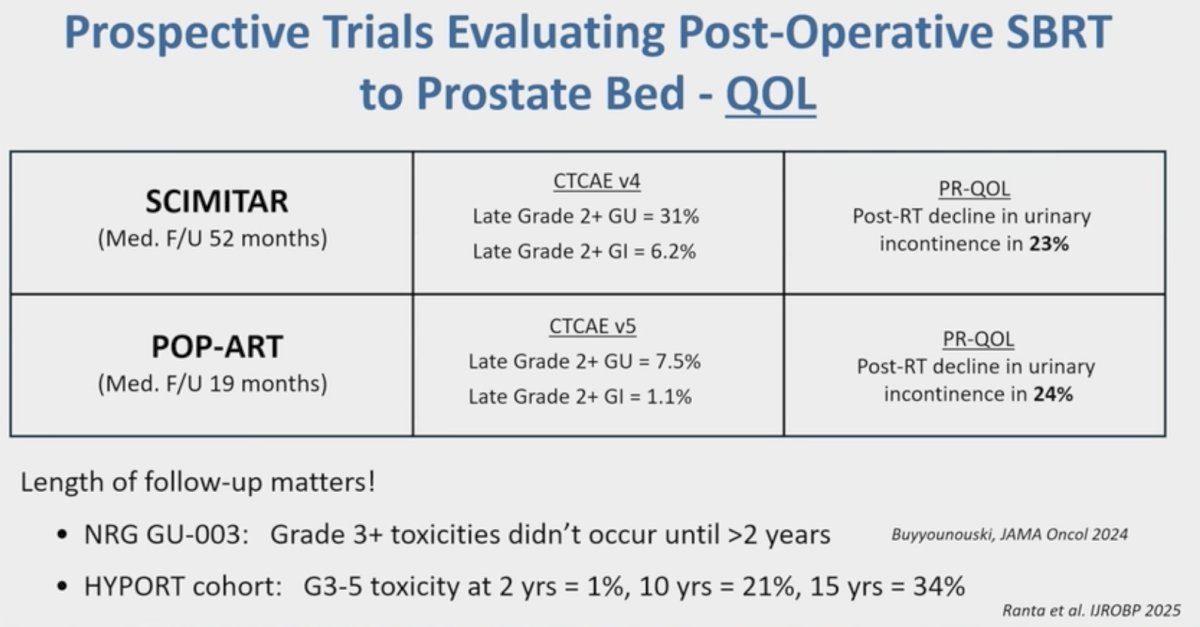
Next, Dr. Mouw addressed the secondary analysis of the RAVES trial, which compared adjuvant and early salvage radiotherapy in the post-prostatectomy setting. This pre-planned secondary analysis of quality-of-life outcomes demonstrated that patients who received early salvage radiotherapy (prior to 2.5 years) did not have significantly worse GI or GU symptoms compared to those who received late salvage radiotherapy, which Dr. Mouw noted was reassuring for patients who require early salvage radiotherapy.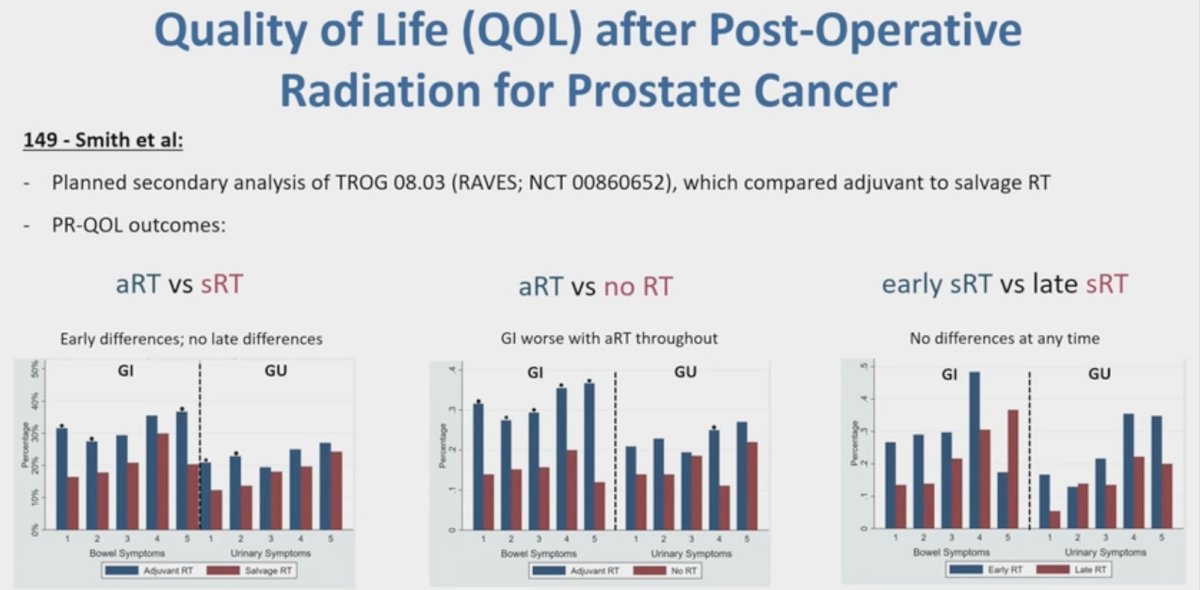
Dr. Mouw’s key takeaways from these three abstracts were as follows:
- Improvements in radiation techniques provide an opportunity for shorter treatment courses for our patients, which have implications for patient convenience and costs.
- Early readouts from post-operative SBRT trials suggest safety and feasibility, but further work is needed in this space:
- Longer follow-up to better evaluate late toxicity
- What is the role of nodal irradiation? ADT? Spacer?
- We need prospective comparisons to current standards of care
Next, shifting to discuss the bladder cancer abstracts, Dr. Mouw noted that TMT includes maximal, safe TURBT with concurrent radiotherapy + radio-sensitizing chemotherapy. TMT has been demonstrated to have similar survival outcomes compared to radical cystectomy in well-selected patients.4 This treatment approach is well supported by expert guidelines (e.g., NCCN), and Dr. Mouw emphasized that radiation oncologists should lead efforts to optimize and expand TMT.
In the abstract presentation by Li et al, the study investigators combined bulk and single-cell RNA sequencing analysis of MIBC cohorts to identify genes associated with progression-free survival in a TMT cohort. They identified 18 radiation-responsive genes associated with progression-free survival. Blad-RadPI integrated the radiation-responsive genes and radiosensitivity index (RSI)-related biomarkers. Using Blad-RadPI, they stratified patients into high- and low-score groups with the high-score group enriched in pro-tumorigenic pathways (e.g., epithelial cell proliferation), whereas the low-score group was enriched in immune-activating pathways (e.g., leukocyte migration).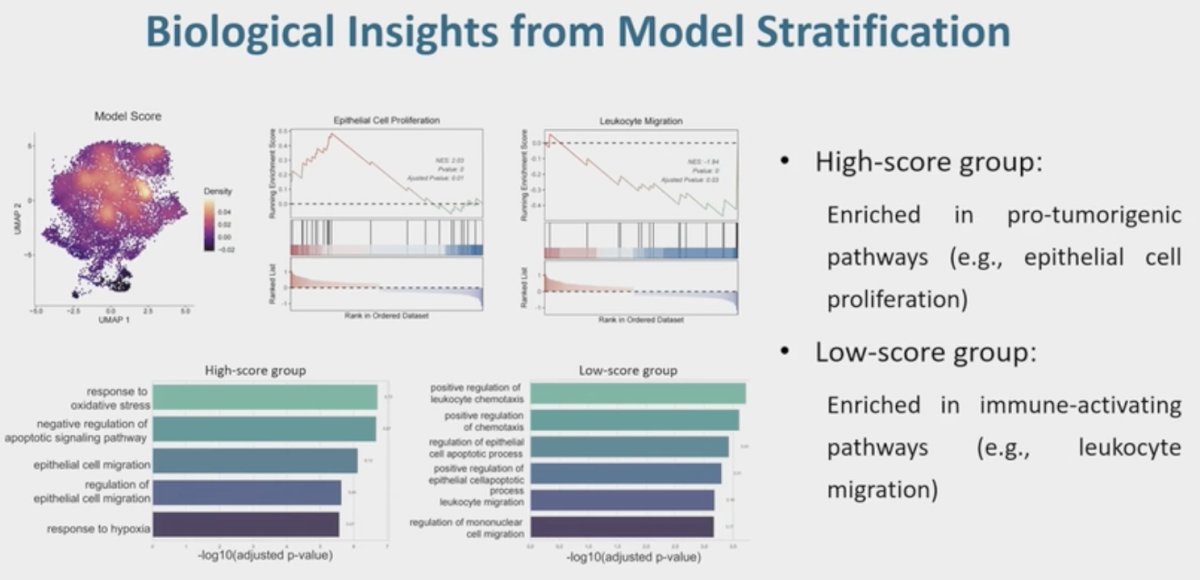
Next, Dr. Mou addressed the abstract presentation by Zhao and colleagues that evaluated circulating tumor DNA (ctDNA) post-TMT. ctDNA has been shown to be strongly correlated with outcomes in metastatic urothelial and MIBC radical cystectomy cohorts. To date, the significance of ctDNA dynamics in TMT cohorts remains unclear.
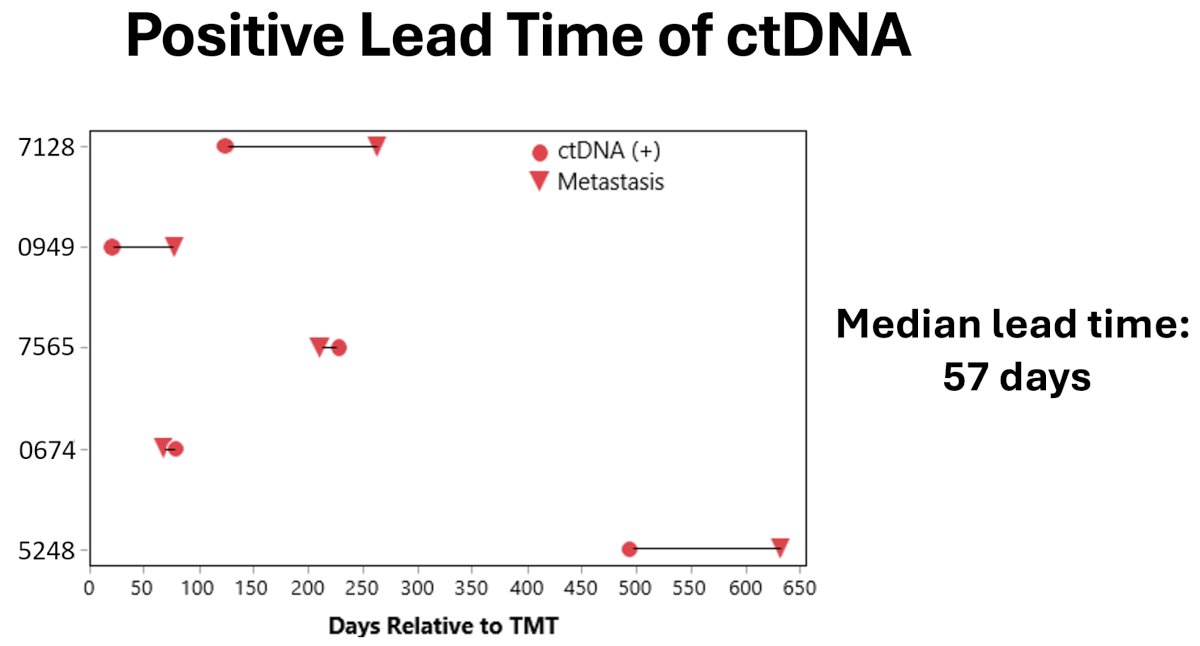
This was a single-center, retrospective analysis of 42 patients with MIBC who underwent TMT at the Moffitt Cancer Center between October 2019 and April 2024 and had ≥1 post-TMT ctDNA (SignateraTM) measurement available. Overall, 6 patients were ctDNA(+), and 36 were ctDNA(-). At a median follow-up of ~15 months, metastatic progression was observed in 5/6 (83%) ctDNA(+) patients, and none of those who were ctDNA(-). The median lead time with ctDNA testing (compared to cross-sectional imaging) was 57 days.
The median recurrence-free survivals were as follows:
- ctDNA(+): 211 days
- ctDNA(-): 1,212 days
The Kaplan Meier-estimated 1-year recurrence-free survivals in the ctDNA(+) and ctDNA(-) groups were 22% and 83%, respectively.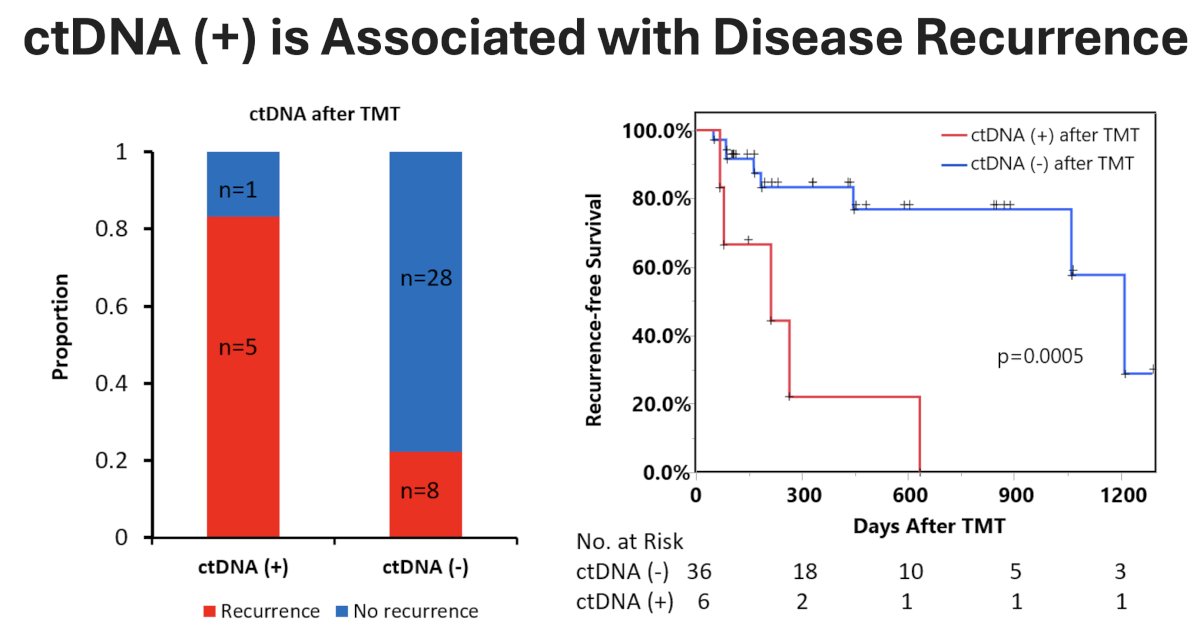
The median recurrence-free survivals were as follows:
- ctDNA(+): 211 days
- ctDNA(-): 1,212 days
The Kaplan Meier-estimated 1-year recurrence-free survivals in the ctDNA(+) and ctDNA(-) groups were 22% and 83%, respectively.
What about elective pelvic nodal irradiation in TMT? Dr. Mouw noted that TROG trials have included treatment of elective pelvic nodes, whereas UK trials have not. Advances in treatment planning and delivery (e.g., IMRT, CBCT) have allowed for improved nodal coverage and OAR sparing.
Dr. Granda and colleagues conducted a meta-analysis of all studies comparing bladder-only (BO-RT) and whole pelvis radiotherapy (WP-RT). They demonstrated the following:
- WP-RT was associated with significant improvements in OS and CSS
- Inclusion of the pelvic lymph nodes in the radiotherapy field may address potential micrometastases in the lymph nodes
- Up to 25% of N0 patients may harbor occult nodal disease
- No DFS benefit was observed with WP-RT. The discrepancy between DFS and OS/CSS may be due to variations in recurrence patterns, success of salvage treatments, and individual patient characteristics
- Time to any recurrence was similar, but survival after recurrence favored WP-RT
- WP-RT did not prevent all recurrences but improves salvage outcomes
- BO-RT may be associated with lower odds of acute GI toxicity (p=0.06), but with similar rates of late GI and both acute/late GU toxicities
- Smaller irradiated volume in BO-RT Reduced bowel exposure
Open questions that remain unanswered with TMT include the following:
- What is the role of novel systemic therapy options (e.g., enfortumab vedotin + pembrolizumab)?
- What is the role of new bladder radiotherapy approaches (e.g., shorter course, SBRT/adaptive radiotherapy)?
- What are the best salvage options?
Presented by: Kent Mouw, MD, PhD, Assistant Professor of Radiation Oncology, Harvard Medical School, Radiation Oncologist, Dana-Farber Cancer Institute, Brigham and Women’s Hospital, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc, Urologic Oncologist, Department of Urology, The University of Arizona, @rksayyid on X during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025
- Carrie C, Hasbini A, de Laroche G, et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): A randomized, multicentre, open-label phase 3 trial. Lancet Oncol. 2016;17(6):747-756.
- Buyyounouski MK, Pugh SL, Chen RC, et al. Noninferiority of Hypofractionated vs Conventional Postprostatectomy Radiotherapy for Genitourinary and Gastrointestinal Symptoms: The NRG-GU003 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2024; 10(5):584-591.
- Ranta K, Wojcieszynski AP, Zhao SG, et al. Severe Late Toxicities (Grade 3-5) With 13 Years of Follow-up after Hypofractionated Postprostatectomy Radiotherapy. Int J Radiat Oncol Biol Phys. 2025; 123(2):374-380.
- Zlotta AR, Ballas LK, Niemierko A, et al. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: a multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023; 24(6):669-681.