(UroToday.com) The 2025 ASTRO annual meeting featured a metastatic prostate cancer session and a discussant presentation by Dr. Comron Hassanzadeh. Dr. Hassanzadeh started his presentation by highlighting the metastatic prostate cancer disease spectrum: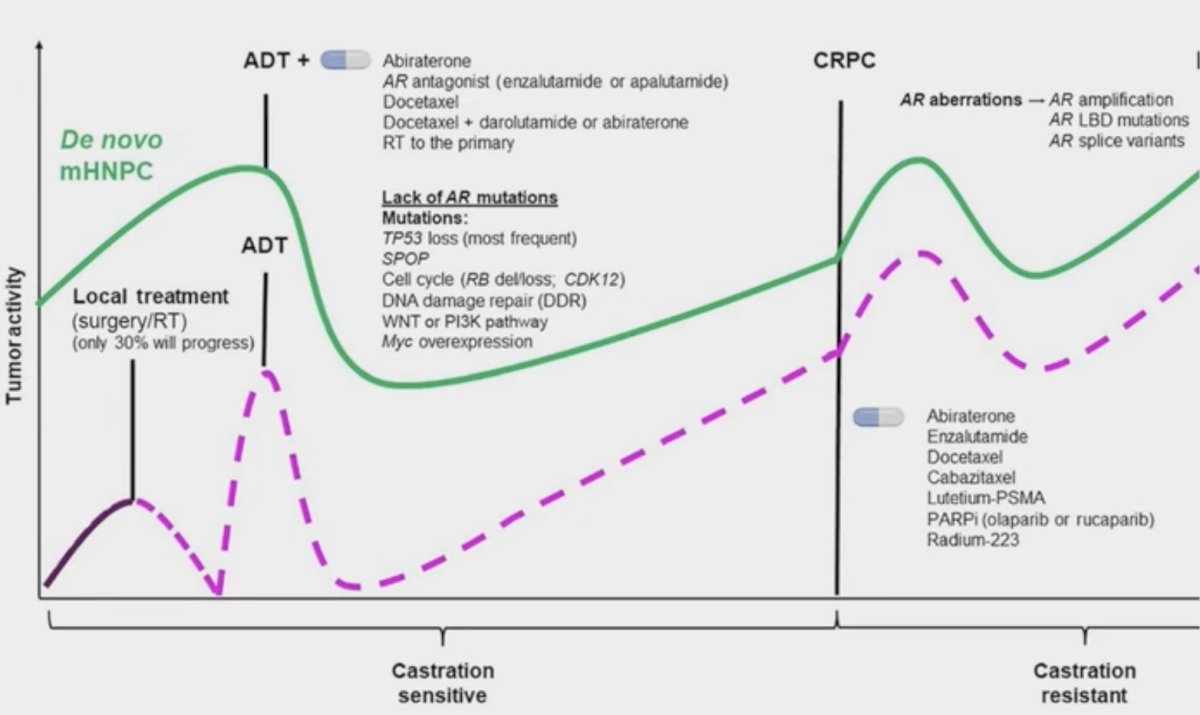
The first abstract discussed by Dr. Hassanzadeh was “Intermittent ADT + Comprehensive Stereotactic Body Radiotherapy for Hormone Sensitive Oligometastatic Prostate Cancer (CROP): Mature Results of a Prospective Trial” by Dr. Patrick Cheung. To put this study into context, he highlighted the STOMP1 and ORIOLE2 trials (which did not incorporate hormone therapy into their trial design), and more recently the EXTEND trial3 which utilized intermittent hormone therapy:![The first abstract discussed by Dr. Hassanzadeh was “Intermittent ADT + Comprehensive Stereotactic Body Radiotherapy for Hormone Sensitive Oligometastatic Prostate Cancer (CROP): Mature Results of a Prospective Trial” by Dr. Patrick Cheung. To put this study into context, he highlighted the STOMP [1] and ORIOLE [2] trials (which did not incorporate hormone therapy into their trial design), and more recently the EXTEND [3] trial which utilized intermittent hormone therapy:](/images/com-doc-importer/229-astro-2025/astro-2025-discussant-milestones-in-metastatic-prostate-cancer/image-1.jpg)
The CROP trial was a phase I/II, single-arm trial with a median follow-up of 6 years. This trial included 89 patients with <= 5 metastatic sites (<3 metastases in one organ), with stereotactic body radiotherapy to all sites (prostate included), and ADT for 12 months followed by intermittent ADT. Failure was defined as biochemical failure, radiographic progression, or restarting ADT, and freedom from any failure rate was 16.1% at 5 years in this trial: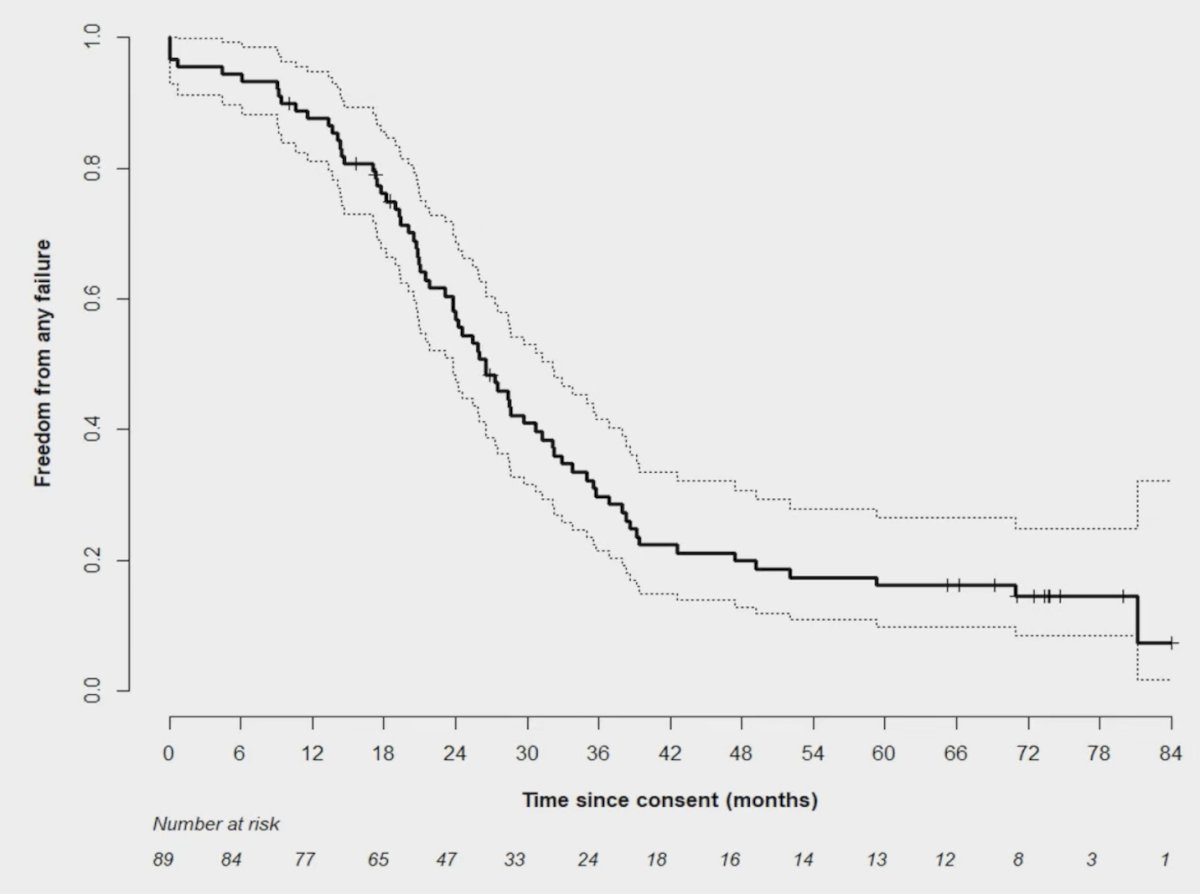
The cumulative incidence of developing CRPC was 22.8% at 5 years, with a median time to CRPC not reached. In the 34 patients who developed CRPC, the median time to the event was 47.7 months: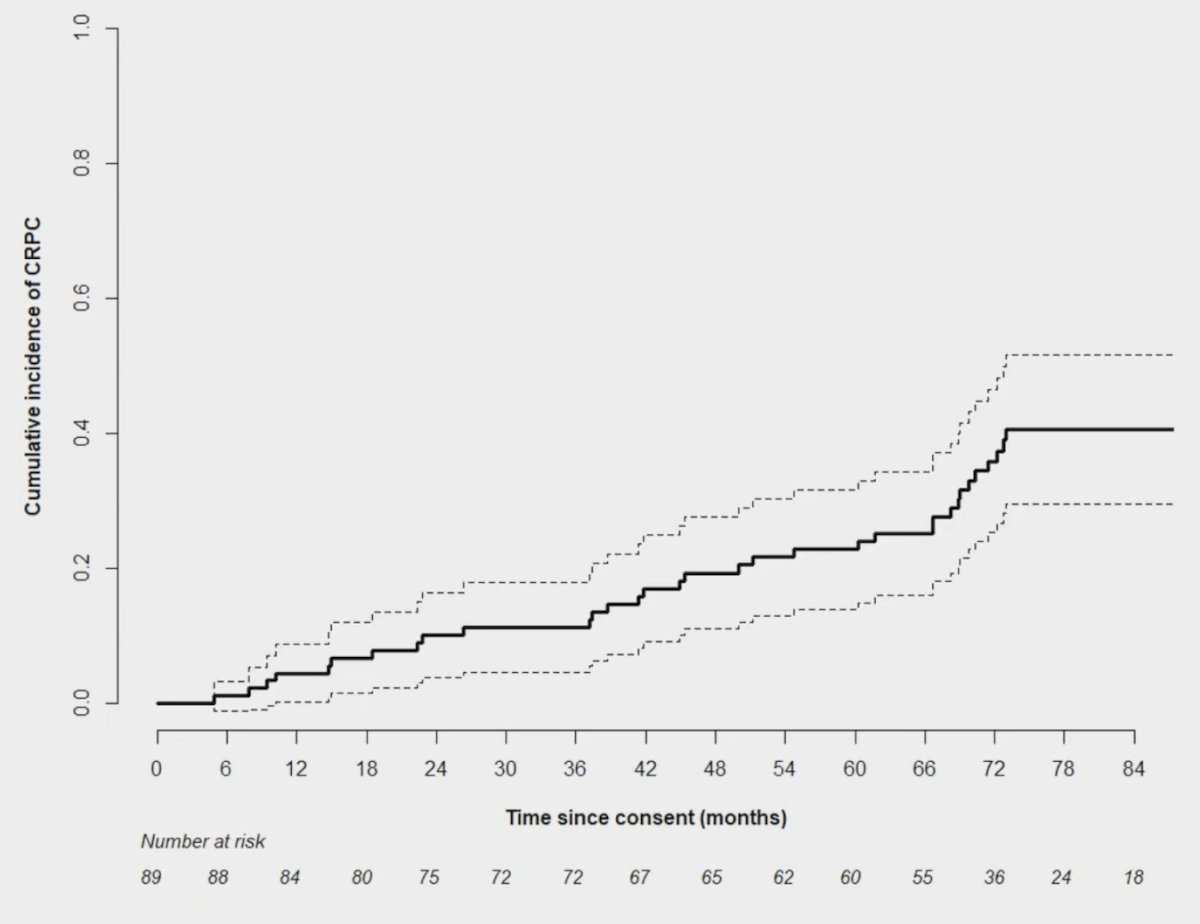
Furthermore, overall survival was significant when stratified by PSA nadir < 0.2 ng/mL versus > 0.2 ng/mL (p = 0.0005), notably with the EXTEND trial reporting that metastasis-directed therapy improved progression-free survival for patients with a PSA nadir <= 0.2 ng/mL. In summary for the CROP trial, Dr. Hassanzadeh emphasized that:
- 39% of patients were alive and off ADT at the last follow-up – a potential for a cure
- There was a low incidence of CRPC: 23% at 5 years
- More incorporation of PSMA PET staging and surveillance into metastasis-directed therapy is needed
- Improved biomarkers are needed to determine intermittent ADT versus doublet or triplet therapy
The second study discussed by Dr. Hassanzadeh was “Local Therapy and Outcome in de novo Metastatic Prostate Cancer: Individual Patient Data Analysis of the TITAN and ARASENS trials” by Dr. Soumyajit Roy. Does local therapy benefit de novo mCSPC? This has been assessed in the context of several clinical trials:
In HORRAD4 there was a benefit for radiotherapy in low burden mHSPC patients on subgroup analysis, which was also seen in the STAMPEDE arm H trial,5 but not in the PEACE-1 trial.6 Dr. Roy reported that 2,201 patients were included in this study of whom 1,853 patients presented with de novo metastatic prostate cancer. A total of 942 patients received ADT alone and 911 received ADT plus androgen receptor pathway inhibitor. Overall, 70 in the ADT group and 56 in the ADT + androgen receptor pathway inhibitor group received local therapy: 30 received radical prostatectomy alone, 93 received radiotherapy alone, and 3 received radical prostatectomy + radiotherapy, respectively:
There was no evidence of differential treatment effect from ADT + androgen receptor pathway inhibitor on overall survival across patients stratified by receipt of local therapy (p = 0.70). Importantly, in the de novo M1 population, compared to no local therapy, radiotherapy was associated with superior overall survival (HR 0.68, 95% CI 0.50-0.98). Dr. Hassanzadeh notes that the confidence intervals are less convincing for a benefit with androgen receptor pathway inhibitors (HR 0.69, 95% CI 0.41-1.07), which may be consistent with PEACE-1. In summary, for the ARASENS/TITAN analysis for the benefit of local therapy, Dr. Hassanzadeh emphasized that:
- The benefit of prostate radiotherapy needs improved patient selection beyond low versus high volume
- We are in need of improved biomarkers, liquid biopsies, etc
- Is there a reduced benefit in the androgen receptor pathway inhibitor era?
- Does radical prostatectomy provide the same benefit as radiotherapy?
The third abstract discussed by Dr. Hassanzadeh was “The Role of Stereotactic Body Radiotherapy in Oligoprogressive Prostate Cancer: A Site-Specific Analysis of the Prospective, Phase II RADIANT Trial” by Dr. Kara Ruicci. In this disease space, the MEDCARE trial assessed 20 patients, of whom 65% had 1 oligoprogressive metastasis based on conventional imaging (but included 95% of patients receiving a PSMA PET/CT off trial). Also, the TRAP trial included 81 patients, of which 71 had 1 oligoprogressive metastasis, 17% were staged with PSMA PET/CT, and 25% of patients had visceral metastases. The median delay in time to next systemic therapy in MEDCARE was 17 months, and in TRAP was 27 months.
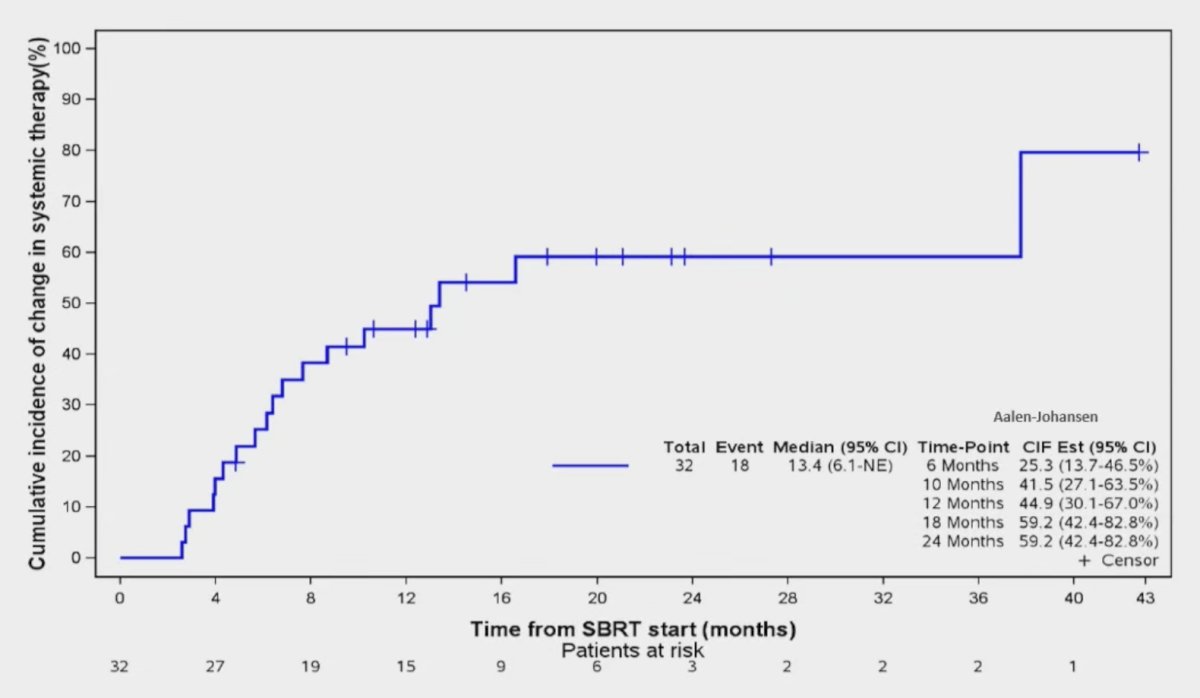
The RADIANT study was a phase II, single-arm study with a primary endpoint of change in systemic therapy. Among 32 patients, all had oligoprogressive mCRPC for >3 months on therapy, 19% of patients were staged with PSMA PET/CT, and all patients received stereotactic body radiotherapy to all sites. The cumulative incidence of change in systemic therapy was 25.3% (95% CI 13.7-46.5) at 6 months, and 44.9% (95% CI 30.1-67.0) at 1 year. The median time from stereotactic body radiation therapy delivery to change in systemic therapy was 13.4 months, and all patients who changed systemic therapy did so secondary to disease progression:
TRAP had a higher median time to next line therapy at 27 months (but only allowed up to 2 sites of metastases), thus, should we define oligoprogressive disease as <2-3 metastases and not <5 metastases? As such, we need more studies incorporating PSMA PET/CT into oligoprogressive mCRPC.
The fourth and fifth abstracts discussed by Dr. Hassanzadeh were “Efficacy and Safety of All-Site Radiation Therapy and Standard of Care Therapy with or without Docetaxel for Hormone-Sensitive High Gleason Score Prostate Cancer: 6-Year Results from a Long-Term Study” and “Efficacy of All-Site Radiotherapy at the Hormone-Sensitive Stage in Combination with Systemic Therapy in Gleason Grade Group 5 Metastatic Prostate Cancer: Long-Term Data from a Single-Institution”, both presented by Dr. Huizhu Chen. Oligometastatic disease in this study was defined as <10 oligometastases, with a median follow-up of 18 months. The intervention of all-site radiotherapy at the hormone-sensitive prostate cancer stage among low-volume patients significantly prolonged castration resistant prostate cancer-free survival in patients with any systemic treatment strategy: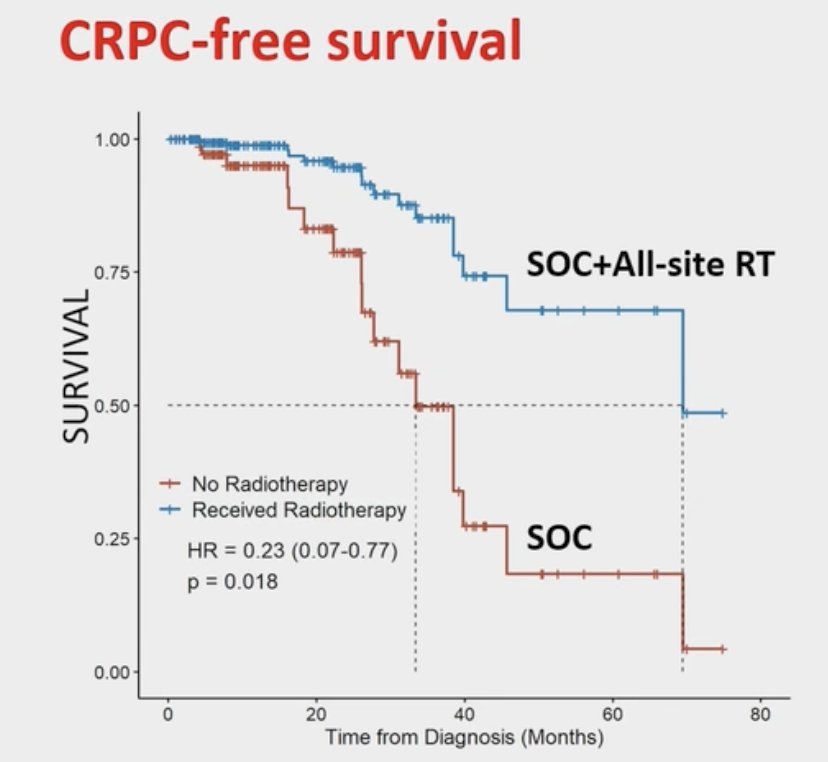
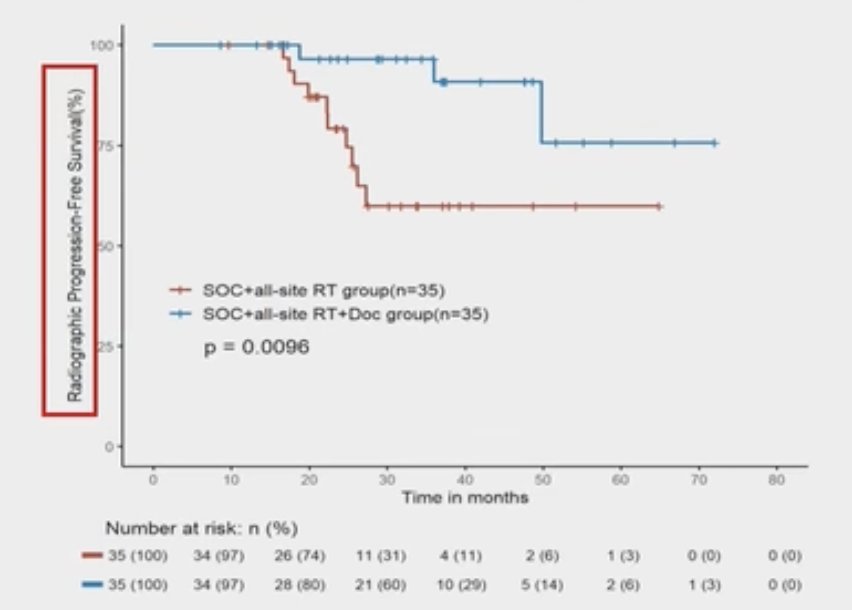
For metastasis-directed therapy with doublet versus triplet therapy, there were 39 patients receiving triplet therapy + radiotherapy versus 127 patients receiving doublet therapy + radiotherapy. Of note, PEACE-1 had 50% of patients treated with docetaxel, but no subgroup analysis looking at triplet therapy + radiotherapy. In this analysis presented by Dr. Chen, the standard of care + all-site radiation therapy + docetaxel group had significantly better 5-year radiographic progression-free survival (p = 0.0096):
Dr. Hassanzadeh notes that two questions remain outstanding:
- How can we de-escalate systemic therapy with stereotactic body radiotherapy strategies?
- Who really needs triplet therapy? We need biomarkers beyond low and high volume burden of disease
Dr. Hassanzadeh concluded this discussant presentation with the following future directions:
- CROP: De-escalated intermittent hormone therapy + stereotactic body radiotherapy in low-volume mHSPC, a potential cure
- Local therapy: Local prostate radiotherapy needs further investigation in PSMA PET staged and the metastasis-directed therapy era
- RADIANT: Metastasis-directed therapy for oligoprogressive mCRPC delays time to next line of therapy switch, with randomized clinical trials coming
- All site radiotherapy: Comprehensive metastasis-directed therapy +/- triplet therapy provides benefit for high burden disease
Presented by: Comron Hassanzadeh, MD, MPH, Clinical Director of Bone Metastasis, Assistant Professor of Radiation Oncology, The University of Texas, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
References:
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018 Feb 10;36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Tang C, Sherry AD, Haymaker C, et al. Addition of metastasis-directed therapy to intermittent hormone therapy for oligometastatic prostate cancer: The EXTEND phase 2 randomized clinical trial. JAMA Oncol. 2023 Jun 1;9(6):825-834.
- Boeve LMS, Hulshof MCCM, Vis AN, et al. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur Urol. 2019 Mar;75(3):410-418.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.