(UroToday.com) The 2025 ASTRO annual meeting featured a metastatic prostate cancer session and a presentation by Dr. Kara Ruicci discussing the phase II RADIANT trial assessing the role of stereotactic body radiotherapy in oligoprogressive prostate cancer. Systemic therapy is the standard of care option for patients with either metastatic hormone-sensitive prostate cancer (mHSPC) or metastatic castration resistant prostate cancer (mCRPC). Regardless of castration status, changing to next-line systemic therapy is the standard of care for patients with progressive metastatic prostate cancer.
Challenges include (i) limited subsequent therapy lines, (ii) toxicity, and (iii) limited disease progression. To preserve systemic therapy options and minimize toxicity, stereotactic body radiation therapy is being increasingly considered for patients with limited disease progression (‘oligoprogression’). However, this is disease site and context specific, as well as there being limited evidence supporting stereotactic body radiation therapy for oligoprogressive prostate cancer. At ASTRO 2025, Dr. Ruicci and colleagues analyzed clinical, toxicity and quality of life data for an oligoprogressive prostate cancer cohort from the prospective RADIANT clinical trial.1
RADIANT (NCT04122469) was a single institution, single-arm, phase II basket trial (launched in 2019) which included patients with metastatic prostate cancer (as well as breast or gastrointestinal cancers) who had been on systemic therapy >3 months, with radiographic evidence of oligoprogression in <5 sites. Analysis by disease site was planned a priori, and the data presented at ASTRO 2025 were specific to prostate cancer patients. Patients received stereotactic body radiation therapy in 1 to 5 fractions to all progressive sites and were maintained on their current systemic therapy. The primary endpoint was the cumulative incidence of change in systemic therapy, estimated with the Aalen-Johnson method. Secondary endpoints included local and distant failure, progression-free survival, overall survival, toxicity, and health-related quality of life. Univariate Fine and Gray competing risk models were applied to examine associations between clinical characteristics and oncologic outcomes.
Enrollment was between October 2019 and December 2023, during which time 41 patients were assessed for eligibility and 32 patients were enrolled. The median age was 74.0 years (range: 61.0-82.0), the median PSA was 6.7 ng/mL (range: 0.03-86.6), 25% had visceral metastases, and a median of 2 prior lines of systemic therapy were used:

In terms of Stereotactic Body Radiotherapy (SBRT) details, 50% of patients had 1 lesion treated, the most common treatment was to the lymph nodes and bone (43.8%), and the median stereotactic body radiation therapy dose was 35 Gy (range: 24-50):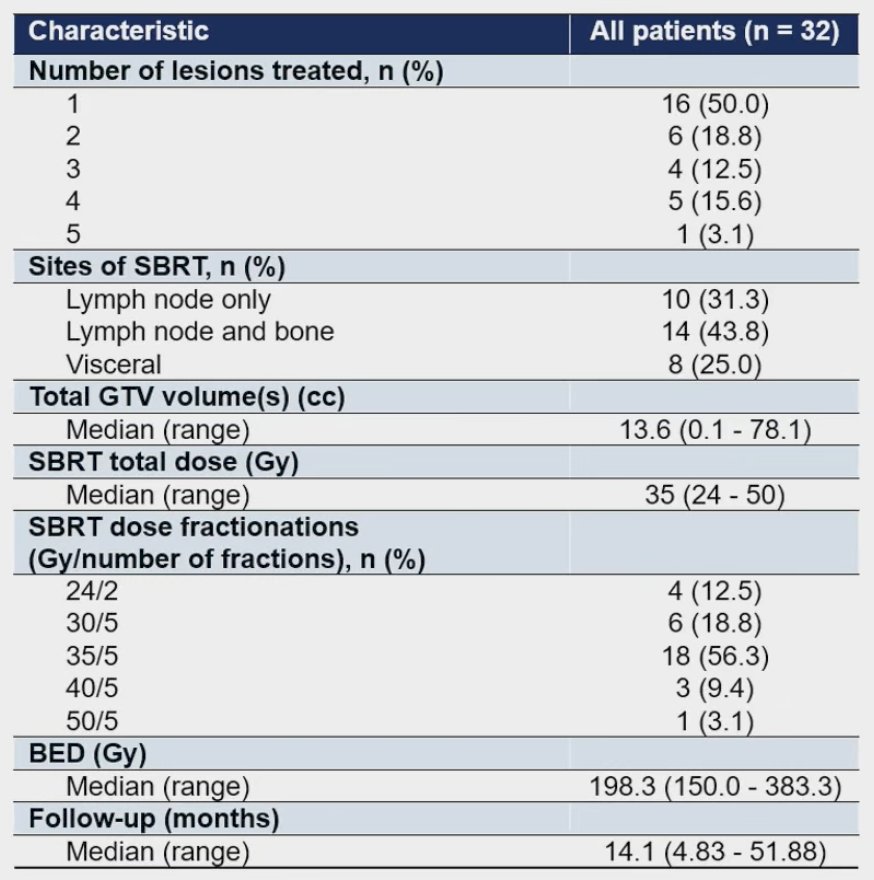
The median follow-up time was 14.1 months (range 4.8 - 51.9 months). The cumulative incidence of change in systemic therapy was 25.3% (95% CI 13.7-46.5) at 6 months, and 44.9% (95% CI 30.1-67.0) at 1 year: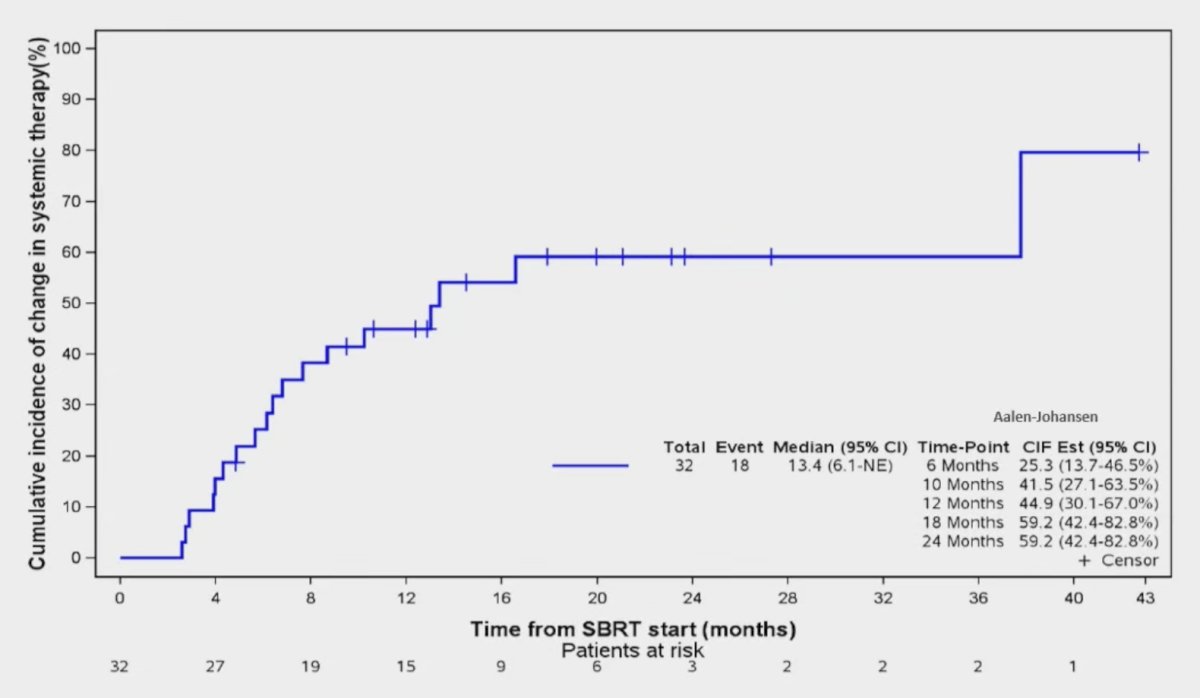
The median time from stereotactic body radiation therapy delivery to change in systemic therapy was 13.4 months, and all patients who changed systemic therapy did so secondary to disease progression. The cumulative incidence of local failure was 12.6% (95% CI 5.0-32.0) at 6 months, and 16.0% (95% CI 7.0-36.2%) at 1 year. The cumulative incidence of distant failure was 28.1% (95% CI 16.0-49.5) at 6 months, and 60.3% (95% CI 45.0-80.9%) at 1 year. Among the patients who experienced distant failure, 52.0% developed new lesions, and 48.0% had progression of pre-existing non-irradiated lesions. The median progression-free survival was 10.2 months (95% CI 6.7-18.4), and at 1 year the overall survival rate was 92.6% (95% CI 83.3-100). The maximal biochemical response after stereotactic body radiation therapy was a decrease in PSA for 62.5% of patients, no change in 3.1%, and an increase in PSA for 34.4% of patients: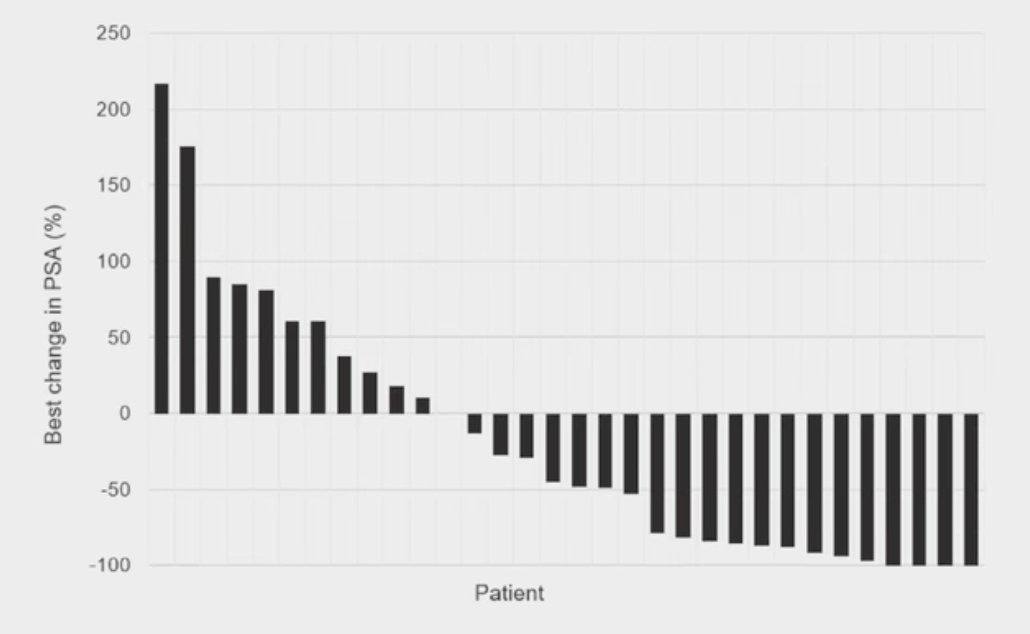
The PSA50 response rate was 43.8% and biochemical response was not associated with any outcome variables. The cumulative incidence of grade 2 toxicity was 25.0% (95% CI, 13.6 - 46.1%) at 1 year, with no grade 3+ toxicities. The median time from stereotactic body radiation therapy delivery to development of any adverse event was 7.9 months. Health-related quality of life was maintained, with no detriment following stereotactic body radiation therapy delivery.
Limitations of this study include the single institution, non-randomized design, and the small sample size. Moreover, there was cohort heterogeneity with regards to prior therapies and disease burden. Change in systemic therapy as the primary endpoint was also at the discretion of the treating physician.
Dr. Ruicci concluded her presentation discussing the phase II RADIANT trial with the following take-home points:
- Stereotactic body radiation therapy is a safe and effective treatment for oligoprogressive prostate cancer, with the potential to delay next-line systemic therapy
- Compared to the early MEDICARE (NCT04222634) and TRAP (NCT03644303) studies, this cohort included patients with higher-risk disease features (ie, visceral disease, late-line systemic therapy)
- There was a variable pattern of disease progression: progression of pre-existing, non-irradiated lesions versus development of new metastatic lesions
- Future work is needed regarding patient selection and utilization of PSMA PET/CT
Presented by: Kara Ruicci, MD, PhD, University of Toronto, Toronto, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
Reference:
- Ruicci KM, Barry A, Ye XY, et al. The role of stereotactic body radiotherapy in oligoprogressive prostate cancer: A site-specific analysis of the prospective, phase II RADIANT trial. Radiotherapy and Oncology. 2025;210:111041.