(UroToday.com) The 2025 ASTRO annual meeting featured a metastatic prostate cancer session and a presentation by Dr. Patrick Cheung discussing results of a prospective trial assessing intermittent ADT + comprehensive stereotactic body radiotherapy for hormone sensitive oligometastatic prostate cancer. In the setting of hormone sensitive metachronous oligometastatic prostate cancer, there have been 4 small randomized phase 2 studies: STOMP,1 ORIOLE,2 EXTEND,3 and RADIOSA.4 Two trials (STOMP and ORIOLE) compared stereotactic body radiotherapy/surgery to observation (no systemic therapy at all), and both revealed that metastasis directed therapy may be able to delay progression and to delay the need to start ADT (compared to doing nothing). However, stereotactic body radiotherapy/surgery alone rarely led to any durable cancer control. The EXTEND trial compared stopping ADT versus stopping ADT + stereotactic body radiotherapy to the metastases in patients who were already on ADT for various durations, showing that adding stereotactic body radiotherapy improved progression free survival and delayed re-starting ADT (this study also included patients with CRPC). Finally, the RADIOSA trial compared stereotactic body radiotherapy to the metastases versus stereotactic body radiotherapy + 6 months of ADT, showing that adding ADT improved progression free survival compared to stereotactic body radiotherapy alone.
The rationale for the CROP study is that systemic therapy is an established standard of care for hormone sensitive prostate cancer. Intermittent ADT has previously been shown to be equivalent to continuous ADT in meta-analyses of randomized trials (prior to the current era of systemic therapy intensification with androgen receptor pathway inhibitors or chemotherapy). Intermittent ADT is an ideal approach to combine with metastasis directed therapy (like stereotactic body radiotherapy), as ADT will stop after a period of time (which will allow for assessment when there is no active treatment), and we know historically what the results are from intermittent ADT alone.
The hypothesis for CROP was that adding stereotactic body radiotherapy to intermittent ADT is safe and will improve the outcomes compared to using systemic therapy alone in hormone sensitive oligometastatic prostate cancer. This was a prospective phase I/II single arm trial at two University of Toronto academic centers. The objectives of the trial were to (i) determine the incidence of grade 3+ late toxicities (especially radiation induced bone fractures) associated with stereotactic body radiotherapy to all metastatic disease sites, and (ii) determine the long term efficacy of stereotactic body radiotherapy + intermittent ADT for hormone sensitive oligometastatic prostate cancer.
Synchronous and metachronous metastatic disease patients were eligible if there were <= 5 metastases, with <= 3 metastases in any one organ system. Conventional scans (CT/bone scan +/- MRI) were used to stage patients at baseline, although novel PET imaging was optional. Stereotactic body radiotherapy was delivered to all sites of disease, including the prostate, if not previously treated. ADT was started prior to or immediately after stereotactic body radiotherapy and was continued for 1 year before moving to an intermittent approach. ADT was restarted for another year when the PSA reached >10-15 ng/mL or earlier if clinically indicated (development of new metastases or rapidly rising PSA). If new metastases developed in an oligometastatic fashion, stereotactic body radiotherapy was delivered to the new lesions in conjunction with restarting ADT. Toxicity (CTCAE v4.0) and PSA measurements were collected every 4 months during follow-up. Conventional scans were performed at a minimum of once per year, but more frequent imaging was allowed at the discretion of the physician.
There were 89 evaluable patients with 171 metastases accrued with a median age of 74 years. The median follow-up time was 74.7 months (IQR 62.3-84.0), and the median baseline PSA was 8.3 ng/mL (IQR 4.2 – 16.3). There were 39 (43.8%) patients with Gleason score of 8-10 prostate cancer, 33 (37.1%) patients had synchronous presentation, and 10 (11.2%) patients had additional PET staging. Overall, 40 (44.9%) patients had 1 metastasis, 25 (28.1%) had 2 metastases, 18 (20.2%) patients had 3 metastases, and 6 (6.7%) of patients had >3 metastases at baseline. The majority of the 171 metastases were in the bone (62.5%) and lymph nodes (31.6%).
There were no acute grade 3+ toxicities due stereotactic body radiotherapy, with 6 (6.7%) of patients developing late grade 3+ toxicity due to stereotactic body radiotherapy. This included one (1.1%) patient with late grade 3 genitourinary toxicity, and 5 (5.6%) patients developing a stereotactic body radiotherapy induced bone fracture; there were no grade 4/5 toxicities were observed.
The median PSA nadir was 0.03 ng/mL (IQR 0.02 – 0.13 ng/mL) after stereotactic body radiotherapy and 1 year of ADT, and the median time to reach PSA nadir was 9.7 months (IQR 6.9 – 15.0 months). Importantly, no patients received systemic therapy intensification with an androgen receptor pathway inhibitor or chemotherapy within the initial year of ADT. Moreover, 72 (80.9%) patients reached a PSA nadir of <= 0.2 ng/mL. The proportion of patients reaching a PSA nadir <= 0.2 ng/mL in this study was higher than all recent trials looking at ADT + androgen receptor pathway inhibitor/chemotherapy. In all of those systemic therapy trials, 16-68% of patients reached a PSA nadir <= 0.2 ng/mL, which was very predictive of overall survival.
Overall, 55 (61.8%) patients restarted ADT at some point after the initial cycle of ADT. The median PSA prior to re-starting ADT was 5.9 ng/mL (IQR 1.5-12.0 ng/mL), with a corresponding mean PSA of 9.0 ng/mL. There were 34 patients (38.2%) who had only 1 cycle of ADT, 19 (21.4%) had 2 cycles of ADT, 20 (22.5%) had 3 cycles of ADT, 10 (11.2%) had 4 cycles of ADT, and 6 (6.7%) had > 4 cycles of ADT. Furthermore, 26 (29.2%) patients moved on to continuous ADT prior to developing CRPC, and 11 (12.4%) patients received an androgen receptor pathway inhibitor or chemotherapy with their ADT at any point after their 1 year of initial ADT. At the last time of follow-up, 35 (39.3%) patients were alive and off ADT.
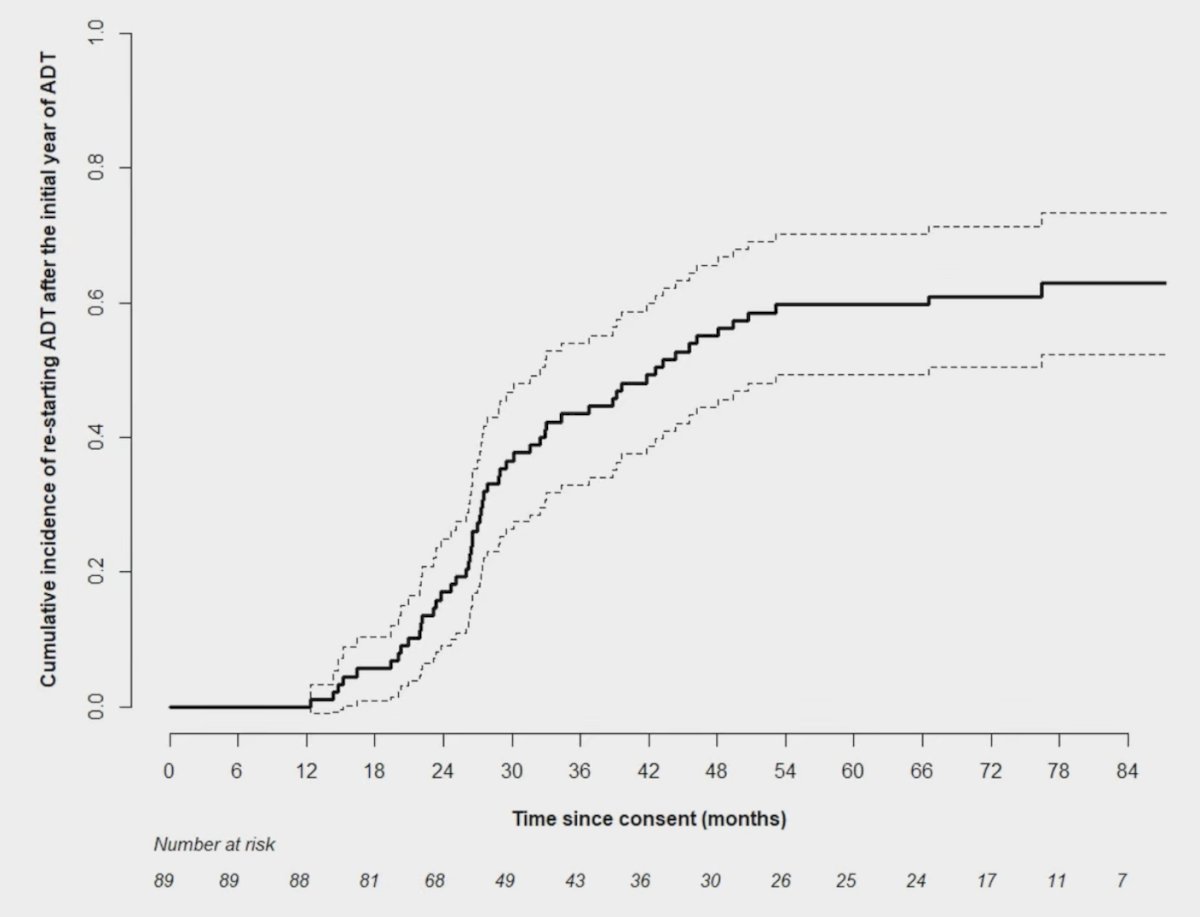
The cumulative incidence of restarting ADT was 43.5% at 3 years and 59.7% at 5 years, with a median time to restarting ADT of 42.6 months. In those who did restart ADT, the median time to the event was 27.6 months:
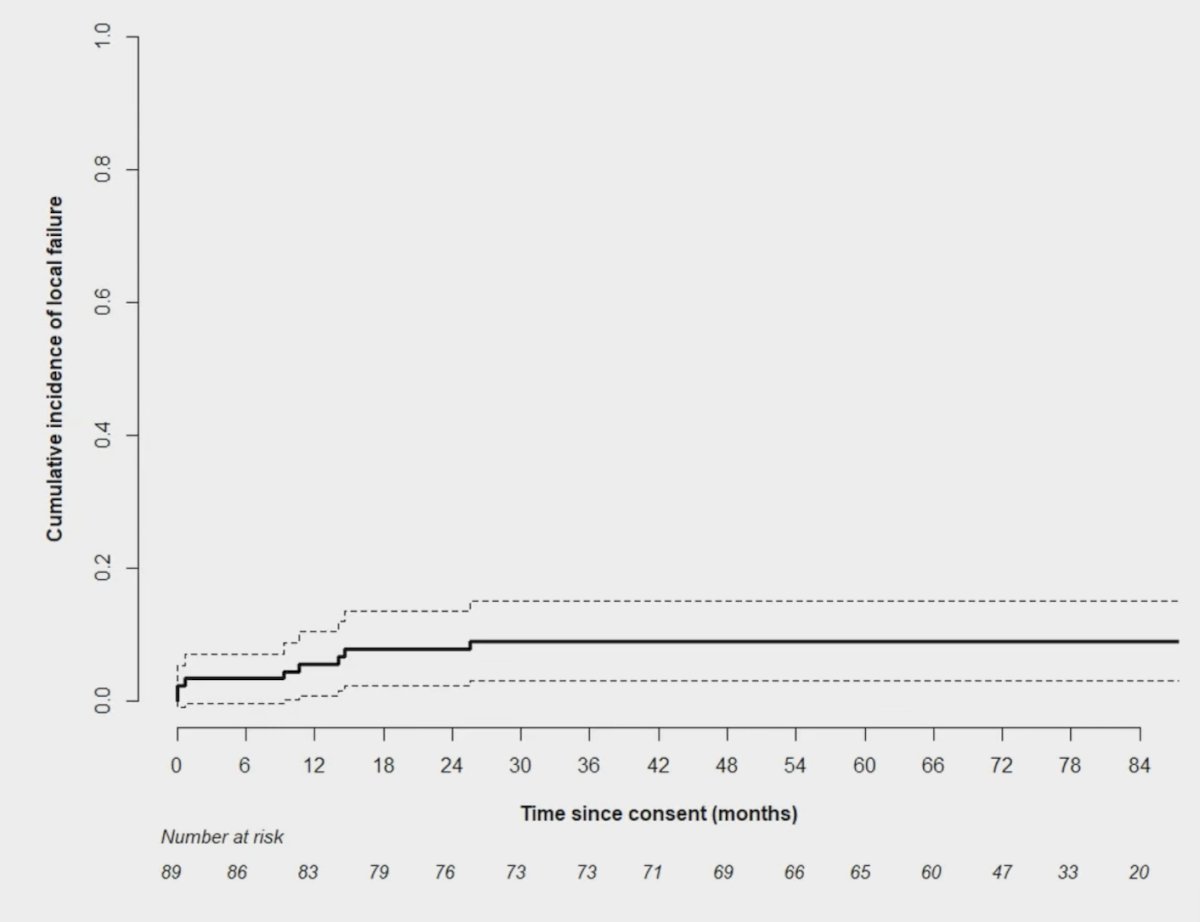
The cumulative incidence of developing local failure at irradiated sites was 9.0% at 5 years:
The cumulative incidence of developing new metastases was 56.1% at 5 years, and the median time to develop new metastases was 45.1 months. There were 55 patients that developed new metastases; the majority (89%) did so in a limited fashion (<= 5 months). There were 36 patients that had subsequent radiotherapy to 72 new metastases:

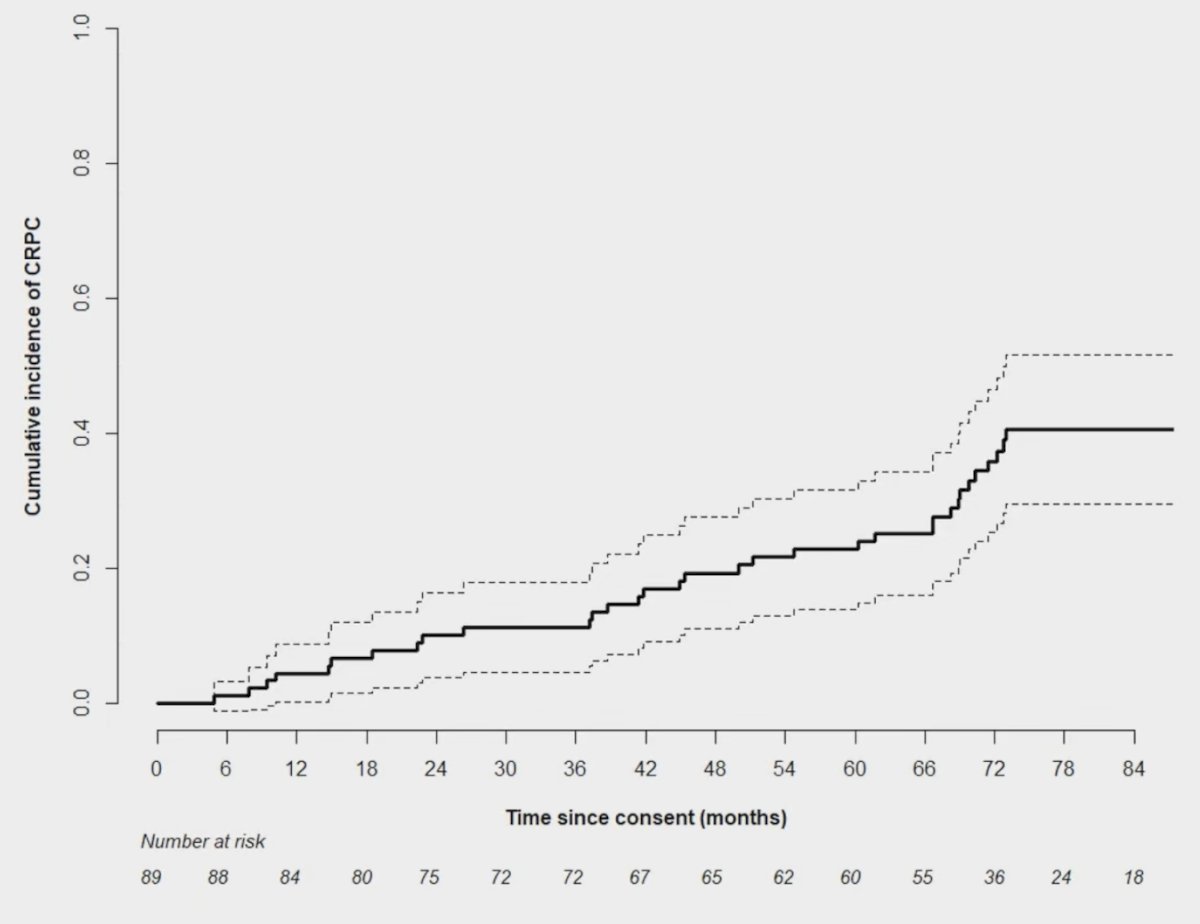
The cumulative incidence of developing CRPC was 22.8% at 5 years, with a median time to CRPC not reached. In the 34 patients who developed CRPC, the median time to the event was 47.7 months:
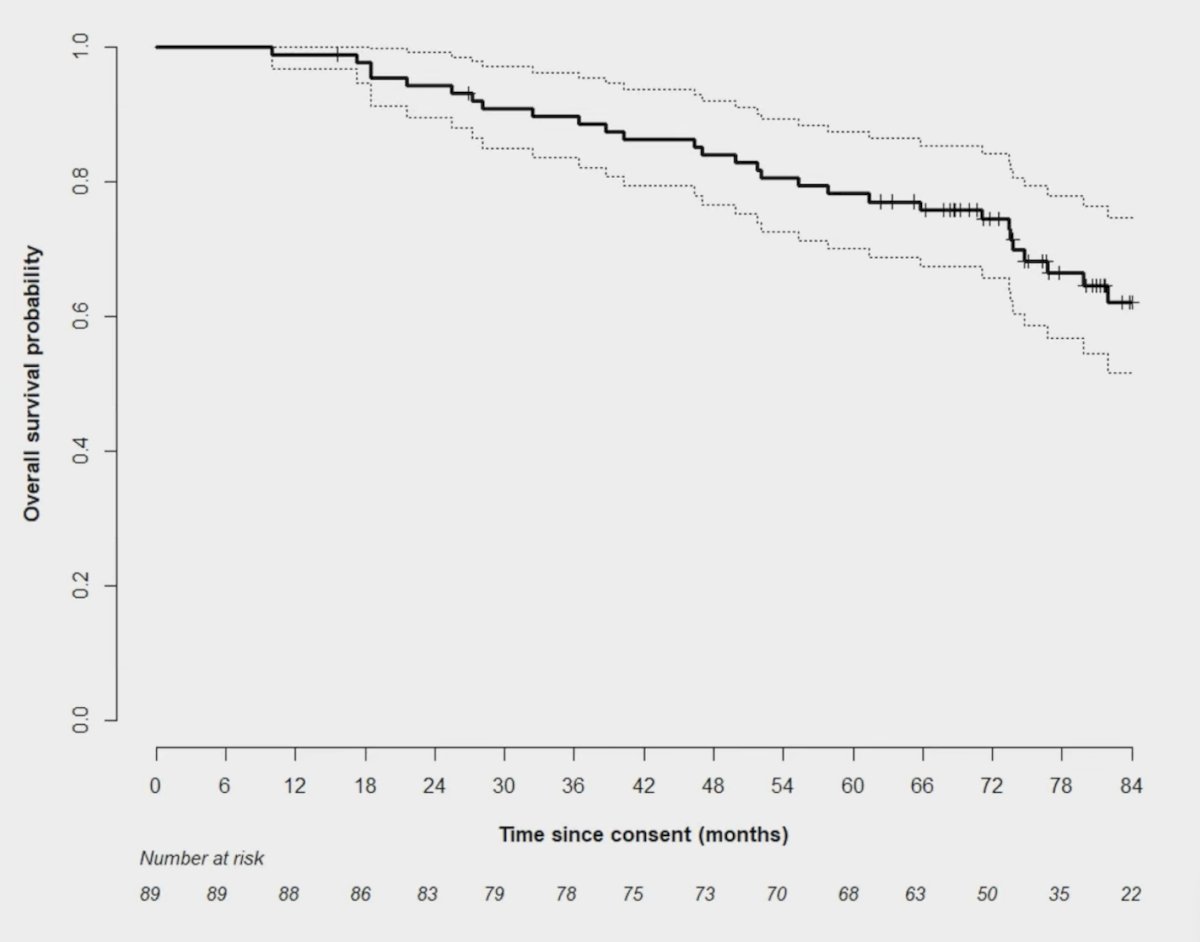
Overall survival was 78.2% at 5 years, and the median time to overall survival was not reached:
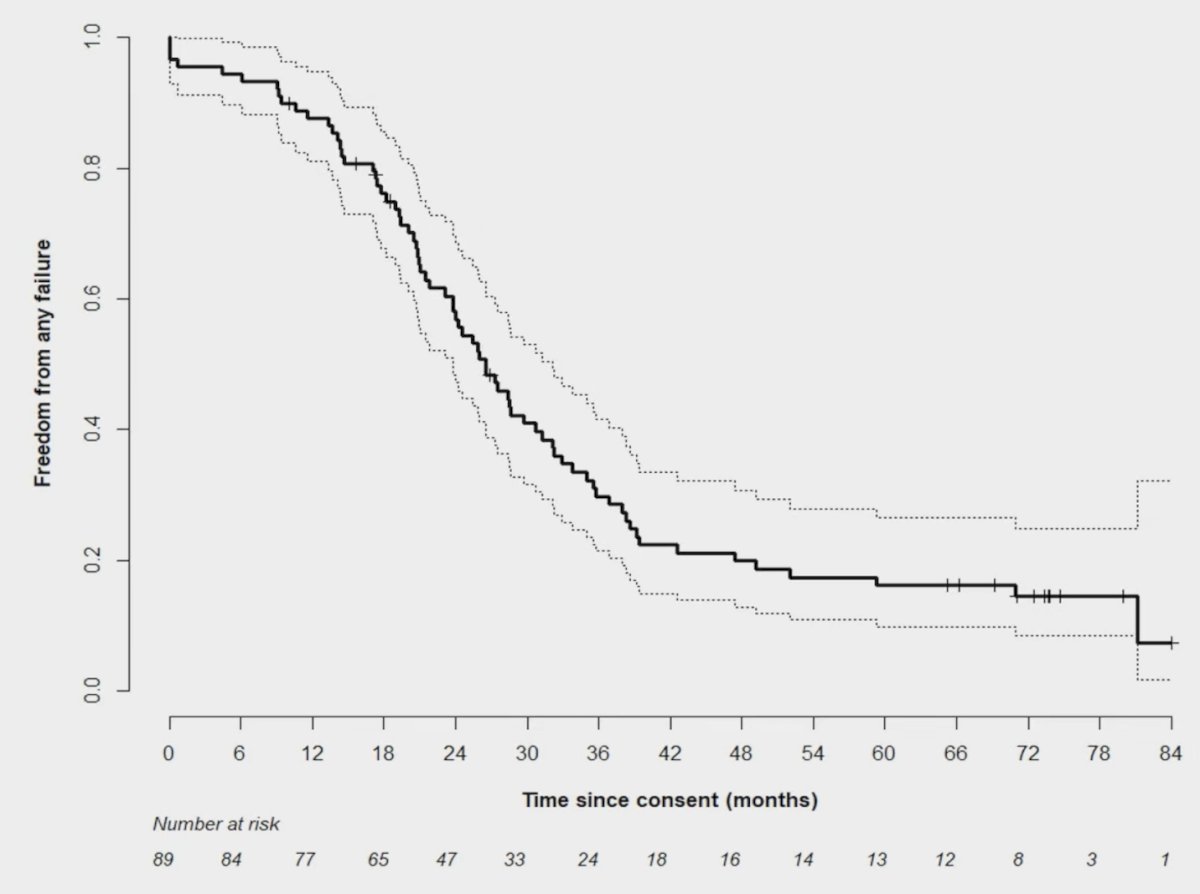
Failure was defined as biochemical failure, radiographic progression, or restarting ADT. Freedom from any failure rate was 16.1% at 5 years:
On multivariable analyses, there were no predictive factors for the cumulative incidence of restarting ADT. For the cumulative incidence of developing new metastases, higher PSA nadir (sHR 1.20, p = 0.016), and >2 organ systems involved (sHR 2.3, p = 0.004) were predictive. For cumulative incidence of developing CRPC, a higher PSA nadir (sHR 1.50, p = 0.001) was predictive, as was PSA nadir (sHR 1.60, p < 0.001) predictive for overall survival. Finally, for freedom from any failure (curative intent definition), higher PSA nadir (HR 1.60, p < 0.001) and synchronous presentation (HR 2.0, p = 0.011) were predictive.
Dr. Cheung concluded his presentation discussing results of a prospective trial assessing intermittent ADT + comprehensive stereotactic body radiotherapy for hormone sensitive oligometastatic prostate cancer with the following take home points:
- Stereotactic body radiotherapy + intermittent ADT resulted in a low incidence of stereotactic body radiotherapy grade 3+ toxicity
- The majority of hormone sensitive oligometastatic prostate cancer patients are not cured, but a small proportion do not progress at all after stereotactic body radiotherapy + 1 year of ADT
- With a median follow-up of > 6 years, the majority of patients have remained on an intermittent ADT strategy. A good proportion of patients were alive and not on ADT at the time of last follow-up
- Efficacy outcomes with stereotactic body radiotherapy + intermittent ADT are very favorable compared to outcomes of using continuous ADT +/- intensification with androgen receptor pathway inhibitor/chemotherapy in patients with low volume metastatic disease
- PSA nadir is a strong predictor of multiple outcomes. The mature favorable outcomes from this study support the strategy of treating hormone sensitive oligometastatic prostate cancer with stereotactic body radiotherapy + 1 year of ADT and using PSA nadir as a biomarker to decide whether to stick with an intermittent approach or whether to move to a continuous ADT approach +/- systemic therapy intensification
Presented by: Patrick Cheung, MD, Sunnybrook Odette Cancer Centre, Toronto, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
References:
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018 Feb 10;36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Tang C, Sherry AD, Haymaker C, et al. Addition of metastasis-directed therapy to intermittent hormone therapy for oligometastatic prostate cancer: The EXTEND phase 2 randomized clinical trial. JAMA Oncol. 2023 Jun 1;9(6):825-834.
- Marvaso G, Corrao G, Zaffaroni M, et al. ADT with SBRT versus SBRT alone for hormone-sensitive oligorecurrent prostate cancer (RADIOSA): A randomized, open-label, phase 2 clinical trial. Lancet Oncol. 2025 Mar;26(3):300-311.