(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session16 - GU 4: Quality of Life Outcomes after Prostate Radiotherapy. Dr. William Jackson discussed the six presentations from the quality of life outcomes after Prostate Radiotherapy Session.
Dr. Jackson began by emphasizing that in prostate cancer radiotherapy, efforts to reduce treatment burden and improve quality of life focus on treatment techniques and technologies. These can be divided into approaches related to dose and fractionation, image guidance with adaptive treatment planning, and the use of rectal spacers.
Dose and fractionationIn terms of dose and fractionation, Dr. Jackson highlighted findings from the EMPIRE-2 trial, presented by Dr. Jani. EMPIRE-2 builds upon advances in molecular imaging by randomizing patients to ^18F-fluciclovine versus ^68Ga-PSMA PET to guide radiotherapy planning. The study incorporates a simultaneous integrated boost (SIB) to PET-avid disease sites within the prostate and pelvis, with the goal of determining whether imaging-directed intensification can improve oncologic outcomes without compromising quality of life. Early results demonstrated no significant differences in EPIC-CP domains, including incontinence, irritative, and bowel function, when comparing boost versus no boost strategies.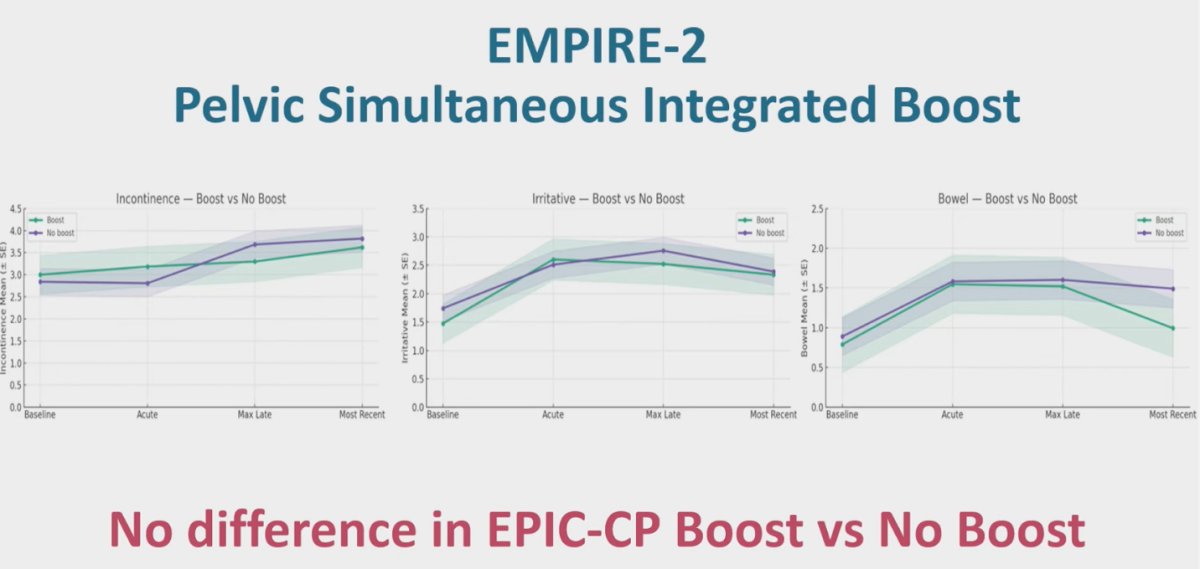
Notably, the same was also true for sexual function, as shown below.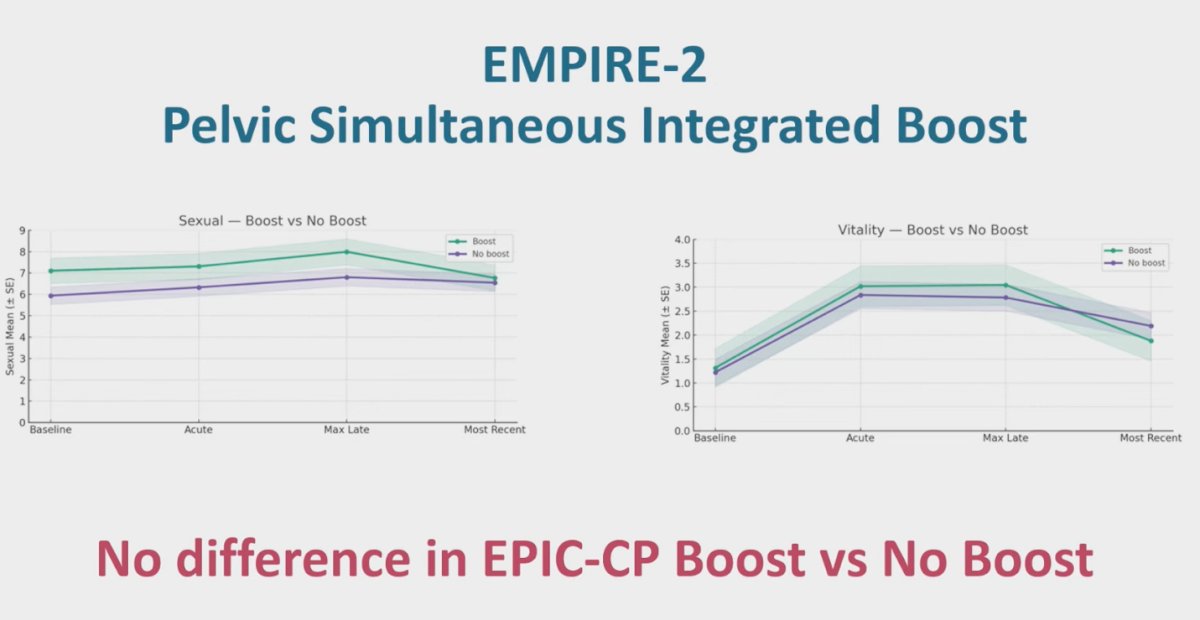
Moving on, Dr. Jackson reviewed Dr. Davis’s randomized phase II trial from Mayo Clinic, which evaluated whether moderate hypofractionated pelvic and/or para-aortic radiotherapy increases GI or GU toxicity compared to conventional fractionation in patients with recurrent prostate cancer involving pelvic (N1) or para-aortic (M1a) nodes. Notably, 22% of patients were treated to both the pelvis and para-aortic nodes. The study demonstrated no increase in acute GI or GU toxicity with hypofractionation, and importantly, no grade 3 toxicities were observed in either arm. These findings are consistent with prior data, supporting the safety of moderate hypofractionation in the pelvic setting without compromising tolerability.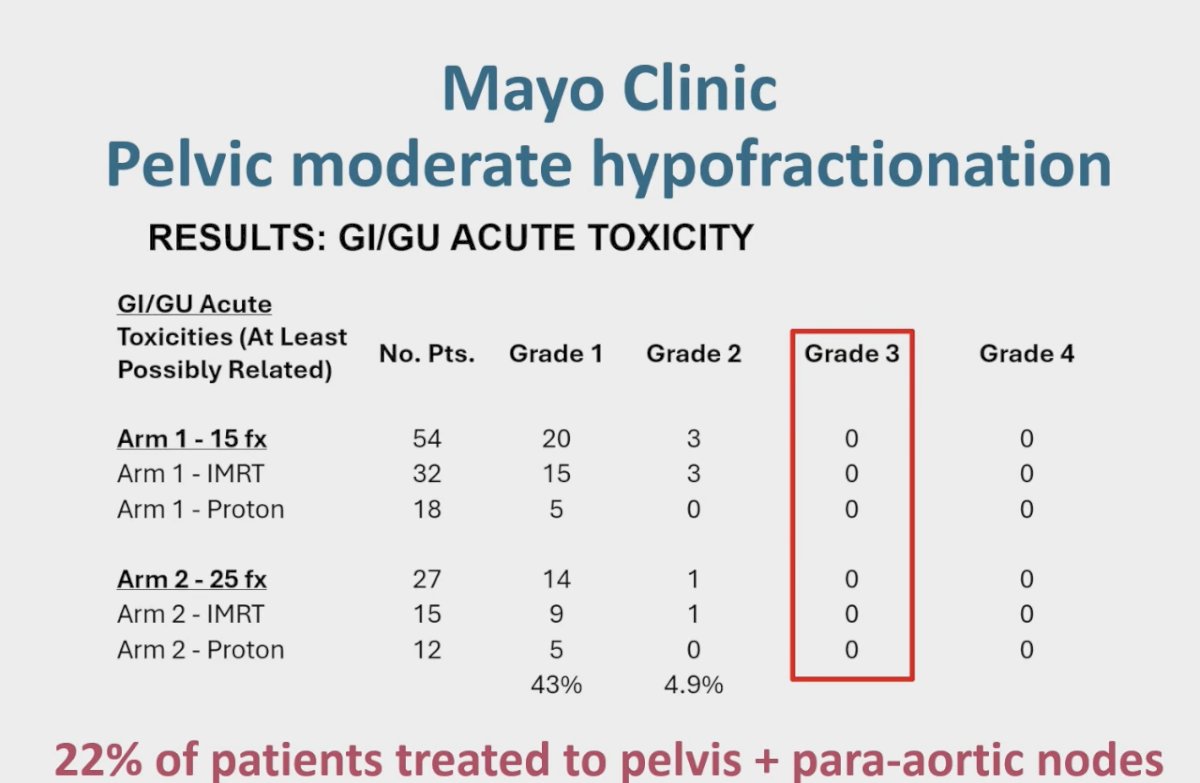
The NRG-GU005 trial, presented by Dr. Yu, randomized patients with localized intermediate-risk prostate cancer to Stereotactic Body Radiotherapy (SBRT) versus moderately hypofractionated Intensity-Modulated Radiation Therapy (IMRT). At one year, outcomes favored SBRT, with fewer declines in bowel and sexual domains.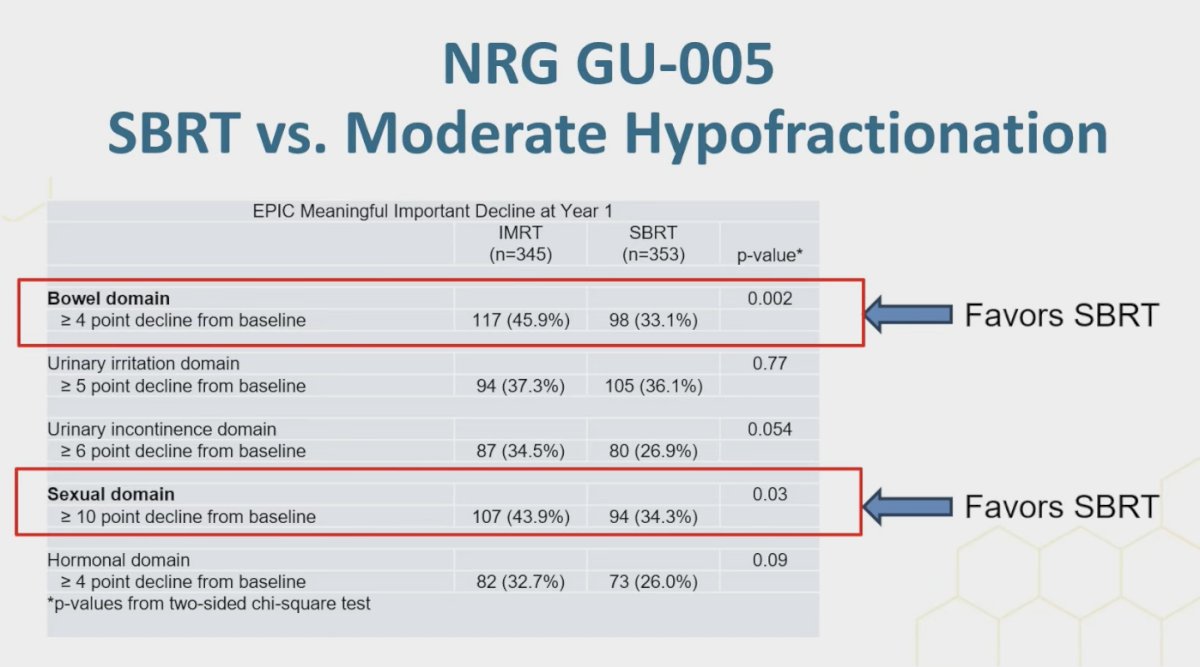
Similarly, significantly fewer patients in the SBRT arm experienced a minimal clinically important decline in the urinary incontinence domain compared with those in the MH-IMRT arm (p=0.023).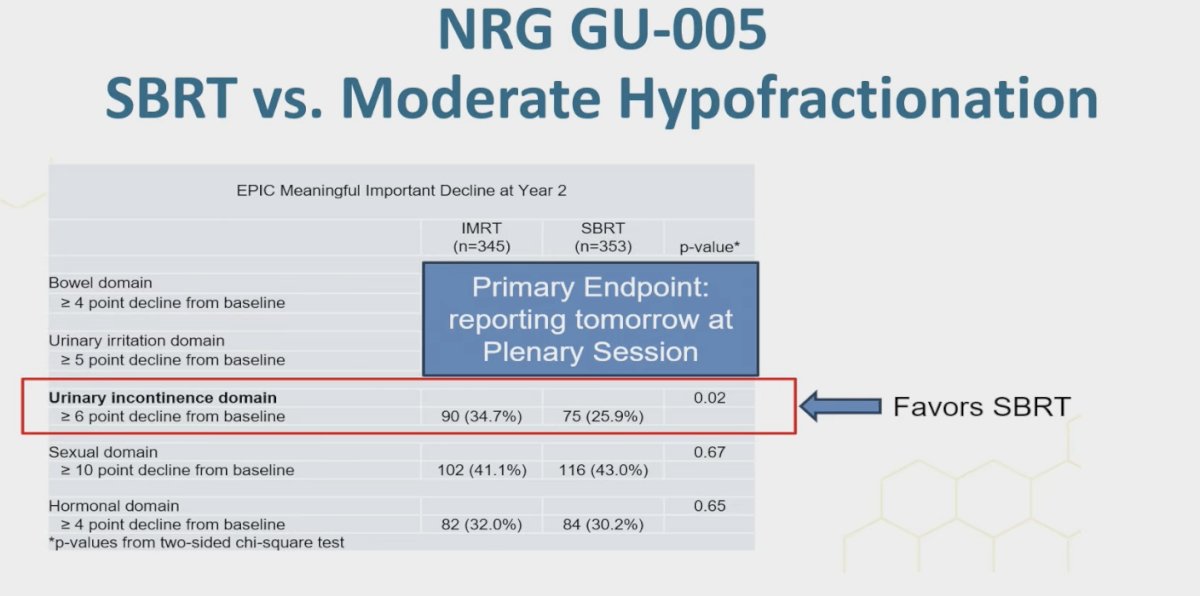
Dr. Jackson raised the question of whether the observed benefits with SBRT were in part driven by the use of smaller PTV margins. He emphasized the caveat regarding the dose and margins permitted in these trials but nonetheless noted that together these studies have established SBRT as a standard of care option for patients with intermediate-risk prostate cancer.
Dr. Jackson concluded by noting that with modern treatment techniques and iso-toxic planning, the incorporation of simultaneous integrated boosts does not appear to negatively affect quality of life, moderately hypofractionated pelvic RT with or without para-aortic nodes is safe in a randomized setting, and that two-year quality of life outcomes after SBRT compare favorably to moderate hypofractionation. He emphasized that these findings align with prior trials such as PACE-B, and ongoing studies like NRG-GU013 will further define the role of SBRT, particularly in the high-risk setting.
Image guidance/ adaptive treatment planningDr. Hall presented results from the MOMENTUM study, a large prospective registry across 12 institutions where prostate cancer patients received five-fraction SABR. Two strategies were compared: adapt-to-shape (daily recontouring) versus adapt-to-position (adjusting without recontouring), with patients blinded to assignment. He showed that daily adaptive recontouring was associated with less worsening of urinary quality of life.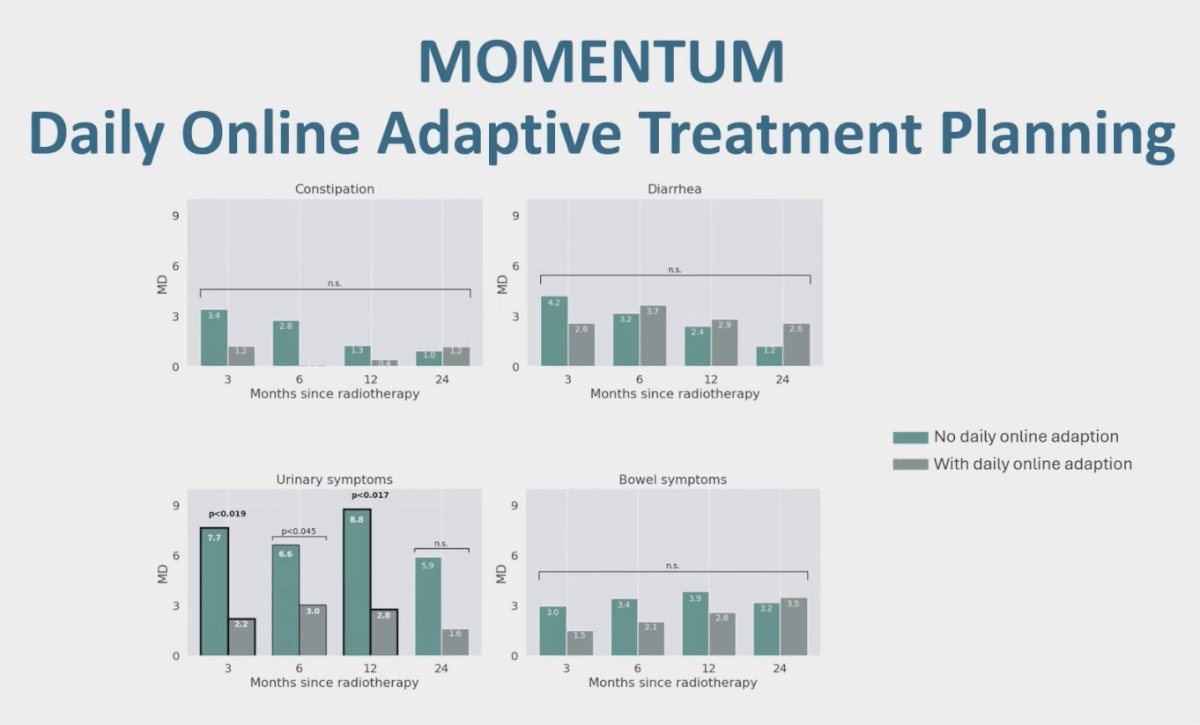
Dr. Jackson highlighted that this study included a large number of patients, making the findings particularly compelling. His key takeaways were that MOMENTUM demonstrates the power of large, international prospective registries and provides convincing evidence that MRI-linac–based daily adaptive radiotherapy with recontouring may improve quality of life. He concluded by raising the question: are these benefits truly driven by daily adaptation, or are they simply the result of more accurate treatment delivery?
Dr. Jackson turned to the POTEN-C trial, presented by Dr Desai, which looked at hydrogel spacer quality assurance. He highlighted that most patients achieved acceptable spacer quality scores, with 68% scoring 1, 22.3% scoring 2, and only 9.7% scoring 0. In terms of rectal wall infiltration, the majority (73.8%) had no evidence of infiltration. He noted that overall, the study demonstrated modest spacer placement with minimal rectal wall infiltration.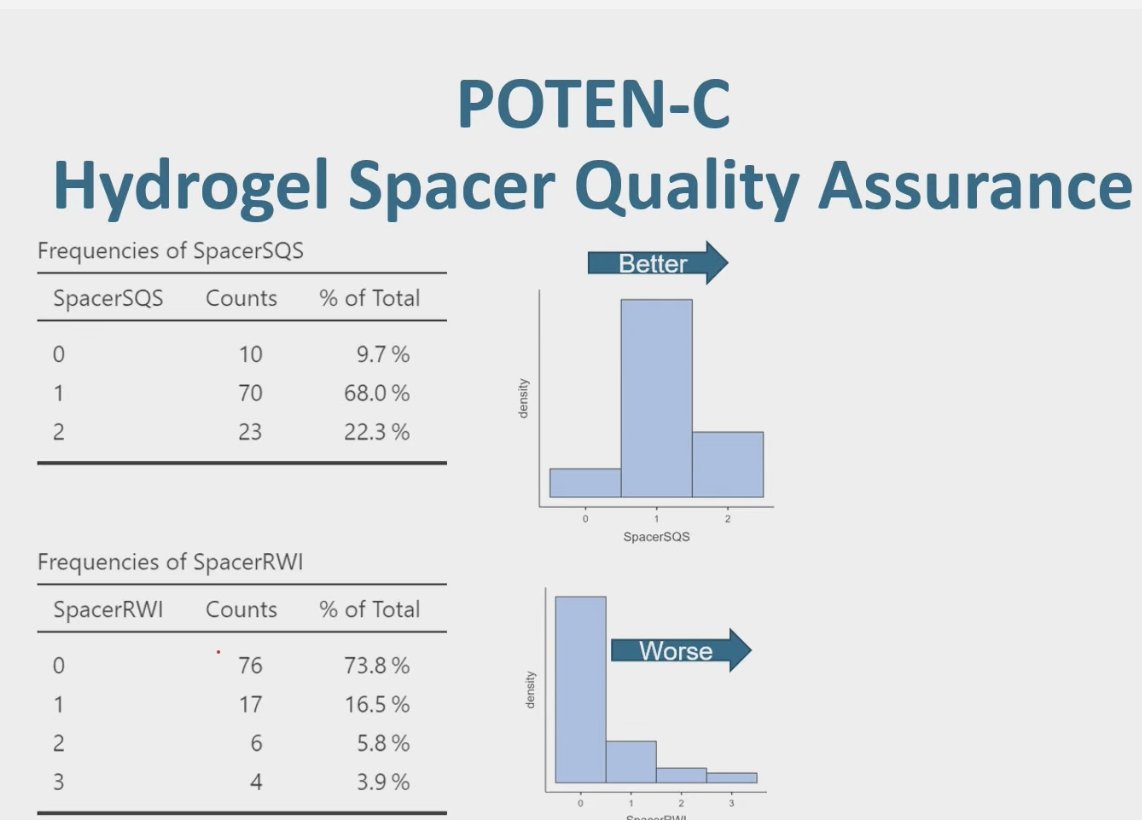
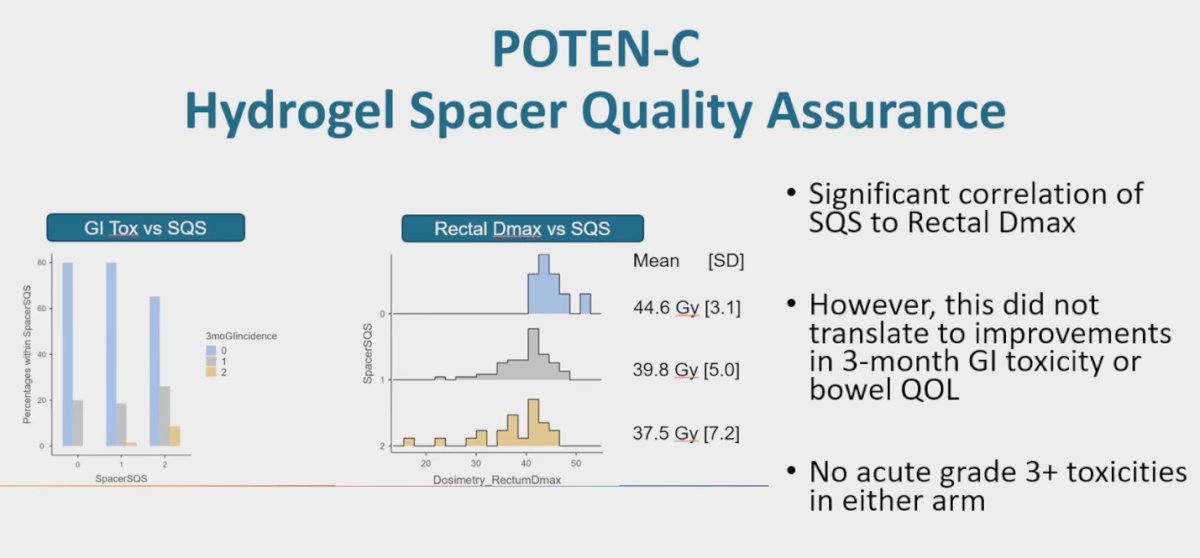
Dr. Jackson pointed out that, not surprisingly, the improvements in spacer quality did not translate into short-term clinical benefits. While there was a significant correlation between spacer quality scores and rectal Dmax, this did not lead to measurable improvements in 3-month GI toxicity or bowel quality of life. Importantly, no acute grade 3 or higher toxicities were reported in either arm.
Dr. Jackson then discussed the BioProtect multinational pivotal randomized phase III trial, presented by Dr Song, which evaluated the use of a biodegradable balloon spacer in prostate cancer IMRT delivered as either moderately hypofractionated or conventional. The study demonstrated improved long-term bowel quality of life as well as improved long-term sexual quality of life, with these benefits persisting across extended follow-up.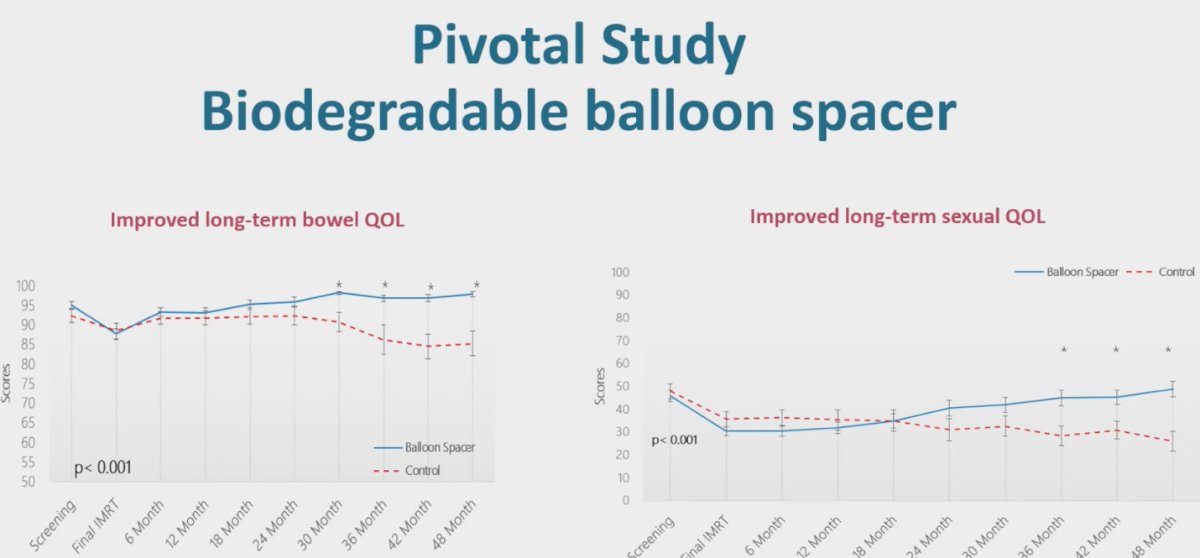
In addition to improved bowel and sexual quality of life, the study also showed numerically improved long-term urinary incontinence QOL, though this did not reach statistical significance, and a significant improvement in long-term urinary irritative QOL.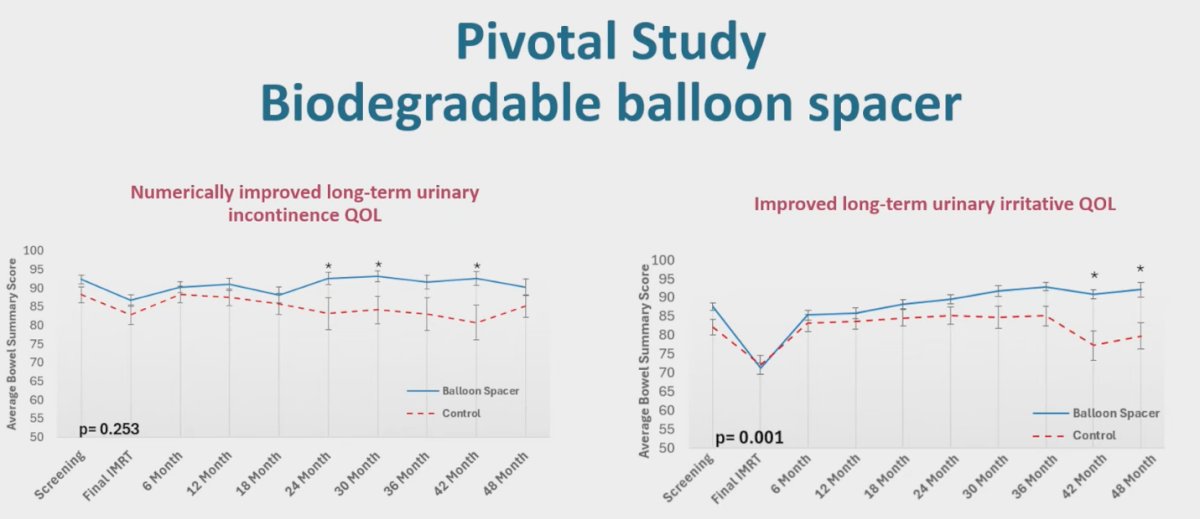
Dr. Jackson cautioned that if we are causing patients toxicity from these devices, it should not be acceptable given how safe modern radiotherapy already is. Since grade 3+ rectal toxicity is very rare with current techniques, rectal spacer placement must itself be extremely safe. He emphasized that the quality of spacer placement directly influences improvements in rectal dosimetry, and that the strongest benefits appear beyond two years after treatment, underscoring the need for long-term follow-up.
Dr. Jackson wrapped up his discussion of this session with the following conclusions:
- Most patients with localized prostate cancer have excellent disease control and long life expectancies, highlighting the emphasis on patient-reported QOL
- Modern radiation techniques result in a favorable overall toxicity profile (minimal grade 3+ toxicity in studies presented in this session)
- We have a rapidly expanding set of treatment techniques and technologies that reduce treatment burden for patients and can make OAR dose-volume histograms profiles look better
- The onus is on us as a field to continue to assess the impact that these new treatment techniques have on patient-reported QOL
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.