(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session16 - GU 4: Quality of Life Outcomes after Prostate Radiotherapy. Dr. Ashesh Jani, presented abstract 198 - Patient-Reported Outcomes in a Randomized Trial of 18F-Fluciclovine vs. 68Ga-PSMA-11 PET/CT-Guided Post-Prostatectomy Radiation with Simultaneous Integrated Boosts.
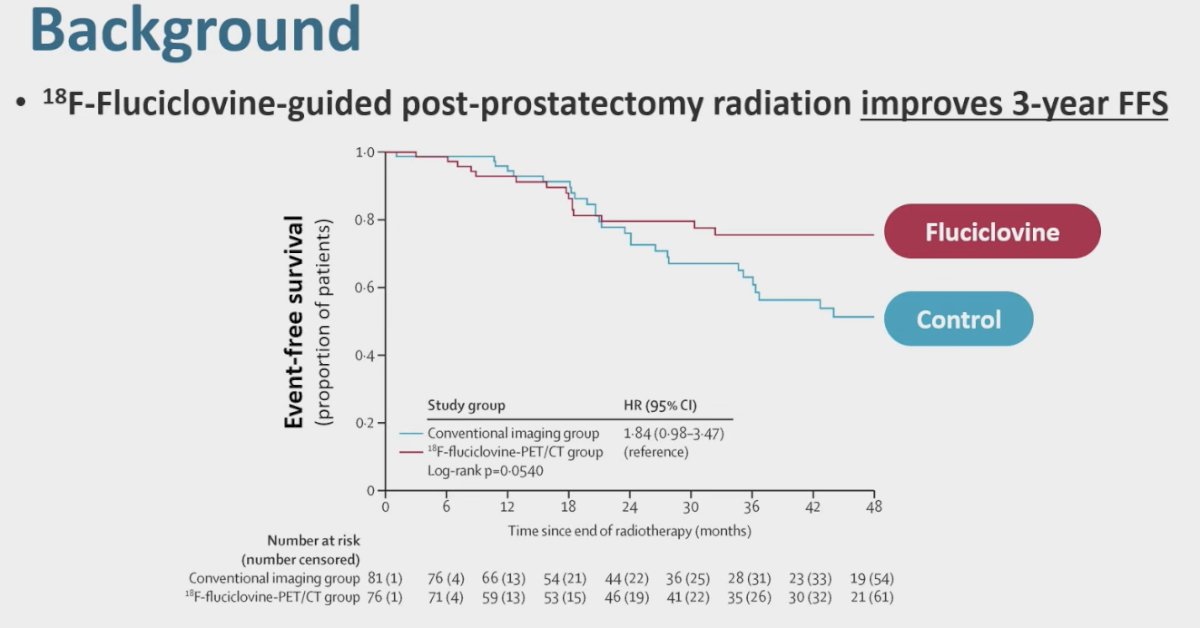
Dr. Jani highlighted the EMPIRE-1 trial, which evaluated the role of 18F-fluciclovine PET in guiding post-prostatectomy radiotherapy. The study demonstrated an improvement in 3-year freedom from progression with PET-guided treatment compared to conventional imaging, with separation of the survival curves favoring the fluciclovine arm. Importantly, incorporation of PET imaging into radiotherapy planning did not negatively impact patient-reported outcomes, as no significant differences were observed across EPIC domains, including urinary incontinence, irritative, bowel, sexual, and vitality scores.1
Dr. Jani next discussed the EMPIRE-2 trial, which builds upon the principles of EMPIRE-1. While EMPIRE-1 focused on the use of 18F-fluciclovine PET to guide post-prostatectomy radiotherapy, EMPIRE-2 takes this a step further by randomizing patients to 18F-fluciclovine versus 68Ga-PSMA PET imaging to direct treatment. Importantly, the trial incorporates simultaneous integrated boost (SIB) strategies to PET-avid disease sites within the prostate and pelvis, aiming to evaluate whether molecular imaging-guided intensification can further improve oncologic outcomes while maintaining acceptable toxicity profiles.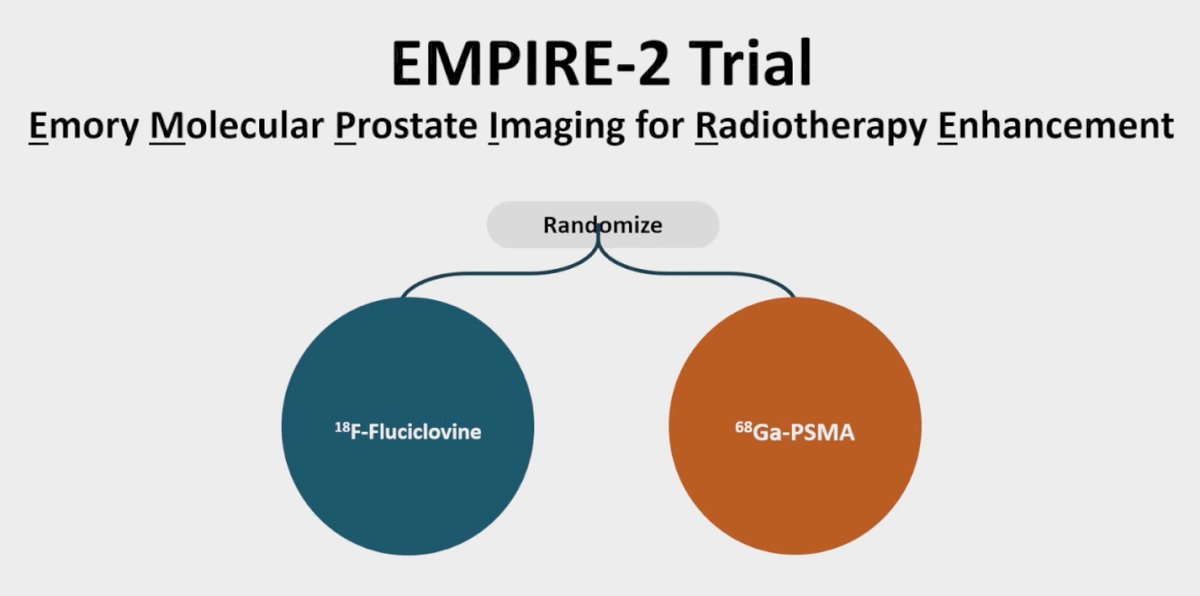
The EMPIRE-2 trial further refined molecular imaging–guided radiotherapy by tailoring treatment based on PET findings. Patients with extra-pelvic uptake had radiotherapy aborted, while those with pelvic nodal uptake received prostate bed plus pelvic RT with a boost to the PET-avid sites. If uptake was limited to the prostate bed, RT was delivered to the prostate bed with a boost to involved areas, whereas patients with no uptake received standard prostate bed RT without a boost. Boost doses were at the discretion of the provider, with pelvic nodes receiving 54–56 Gy and prostate bed lesions escalated to 70–76 Gy. This adaptive design highlights how advanced PET imaging can personalize RT fields and intensities to maximize efficacy while limiting unnecessary exposure.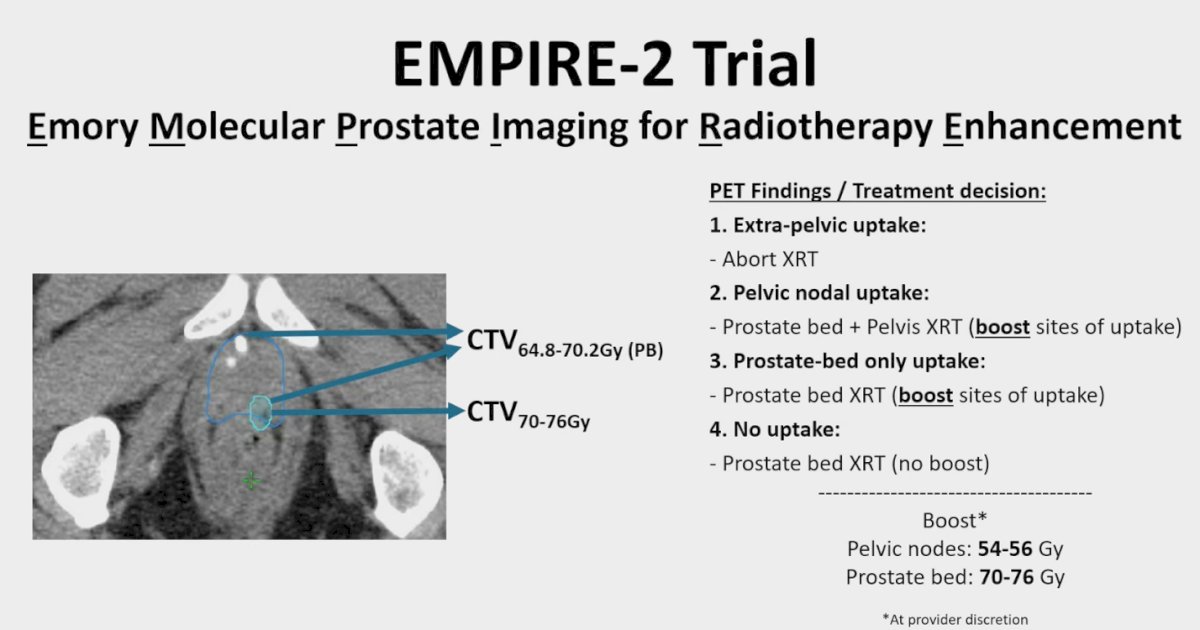
The CONSORT diagram for the EMPIRE-2 trial presented below, shows that 140 patients signed consent and were randomized equally to either 18F-fluciclovine (n=70) or 68Ga-PSMA (n=70). In the fluciclovine arm, 65 patients underwent PET/CT, with 59 ultimately receiving radiation; 5 had extra-pelvic disease on PET and 1 declined treatment. In the PSMA arm, 69 underwent PET/CT, with 60 receiving radiation; 8 had extra-pelvic disease and 1 declined treatment. This resulted in 59 and 60 patients, respectively, being included in the final analysis.
At ASCO GU, the EMPIRE-2 trial reported its primary endpoint of 2-year biochemical relapse-free survival (bRFS). Compared with the experimental arm of EMPIRE-1, EMPIRE-2 demonstrated a statistically significant improvement in bRFS, with a p-value of 0.008.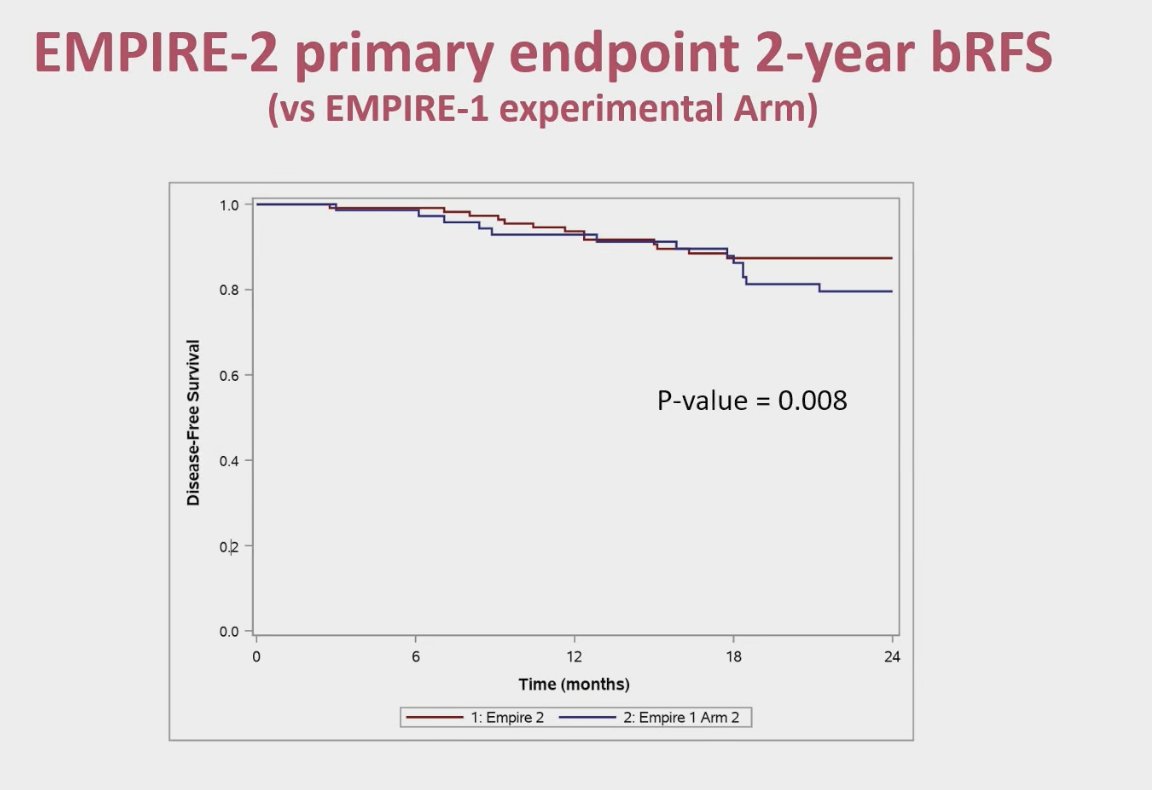
A year ago, the investigators reported acute toxicity outcomes using CTCAE v5.0. There were no significant differences between the two arms. Rates of grade 2 GU events were 16.9% with fluciclovine versus 6.7% with PSMA (p=0.15), while grade 2 GI events were 5.1% and 1.7%, respectively (p=0.53). No grade 3 toxicities were observed in either group.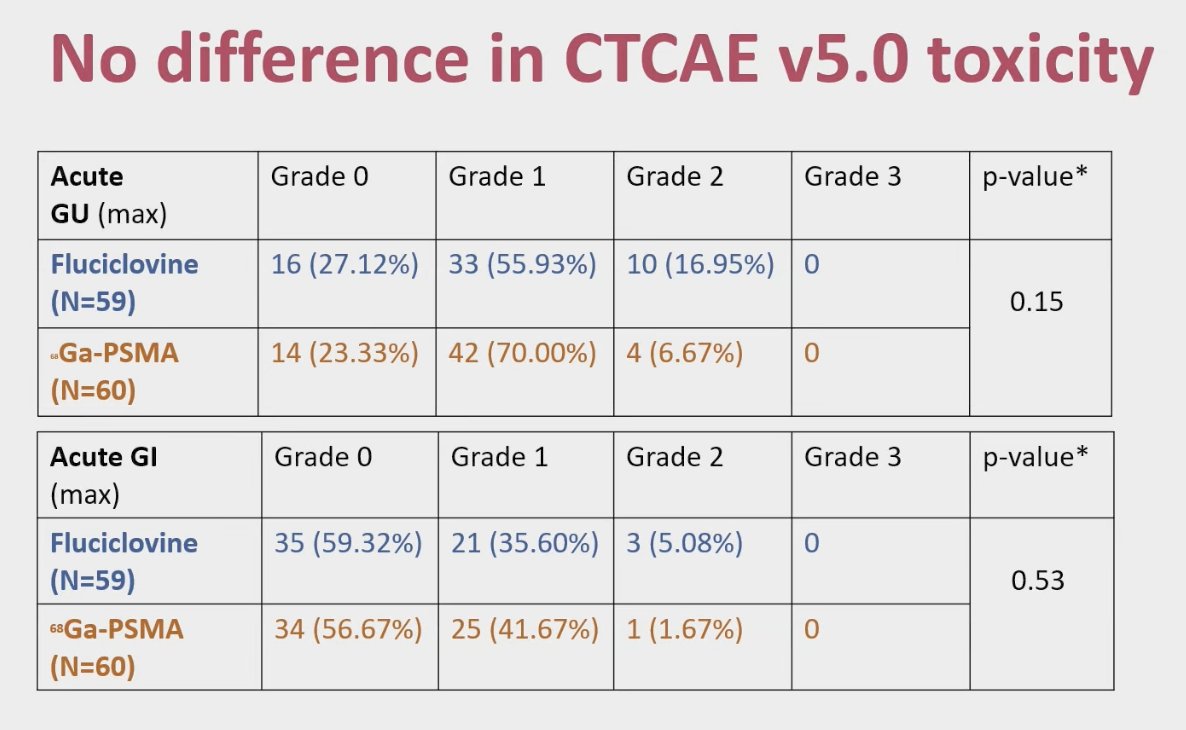
The hypothesis for this analysis was that incorporation of 68Ga-PSMA or 18F-fluciclovine PET/CT-guided post-prostatectomy radiation with PET-guided boost would result in similar changes in patient-reported outcomes (PROs), as measured by the International Prostate Symptom Score (IPSS) and the Expanded Prostate Cancer Index Composite for Clinical Practice (EPIC-CP) short form.
Patient characteristics were well balanced between both arms and are summarized in the table below.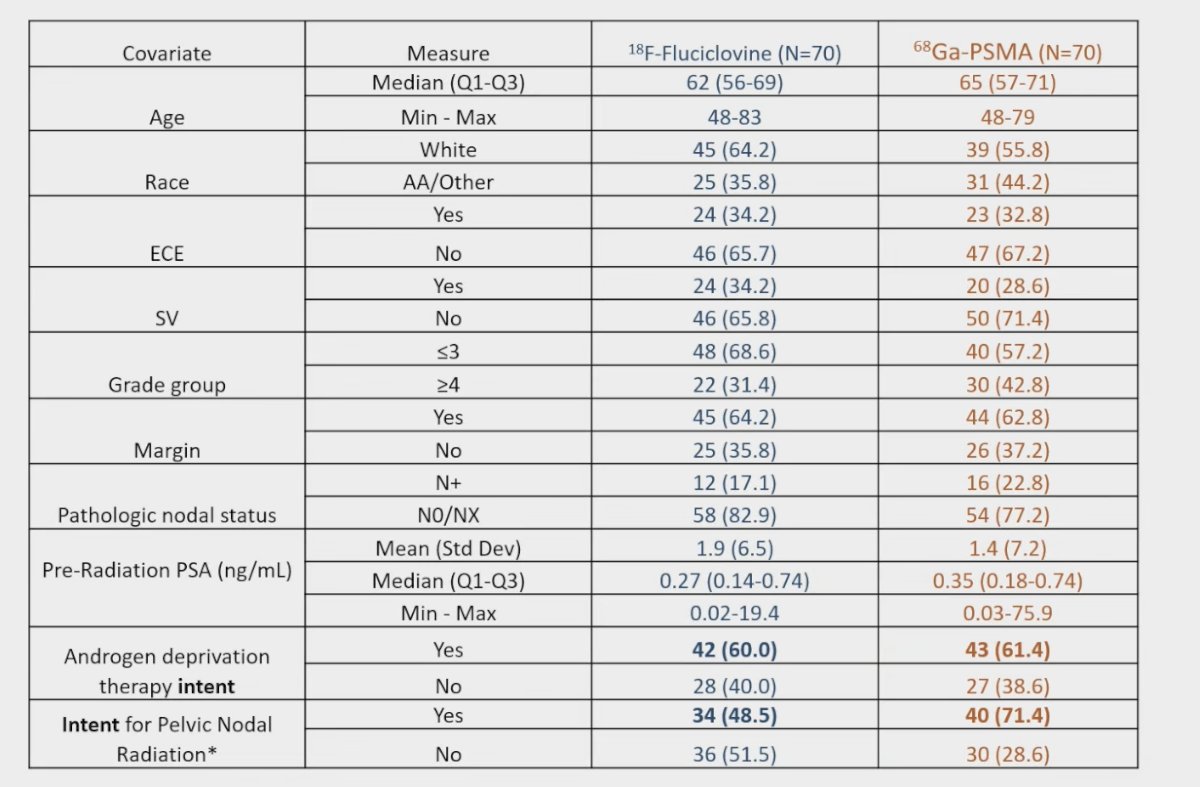
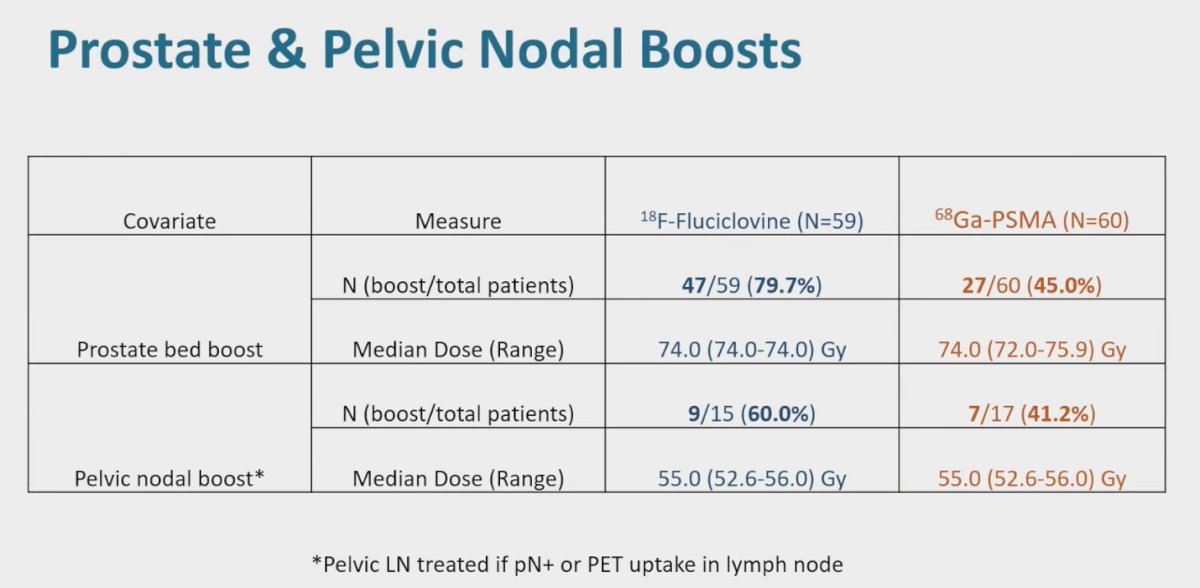
Prostate and pelvic nodal boost delivery was generally well balanced between the two imaging arms. In the 18F-fluciclovine group, 79.7% of patients received a prostate bed boost compared with 45.0% in the 68Ga-PSMA cohort, with nearly identical median doses administered across groups. Similarly, pelvic nodal boosts were delivered in 60% of evaluable patients in the fluciclovine arm and 41.2% in the PSMA arm, with consistent median doses of approximately 55 Gy.
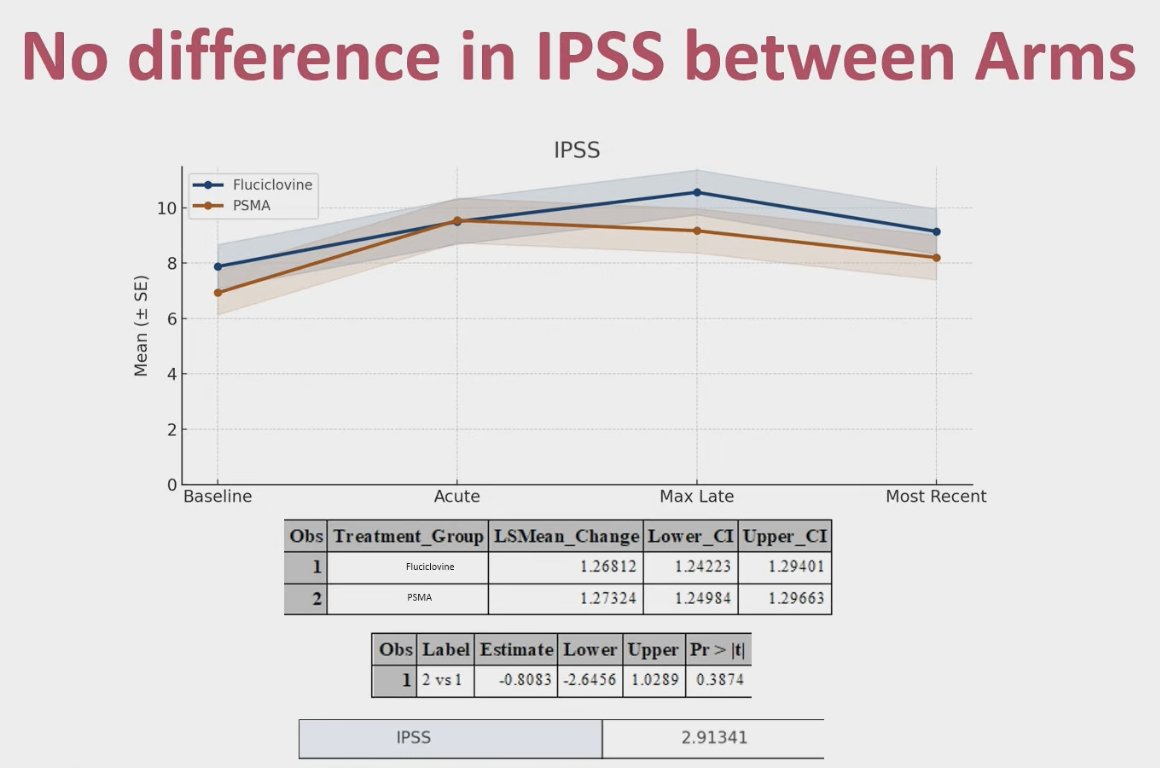
The analysis of IPSS demonstrated that both treatment groups experienced a rise in urinary symptom scores during the acute phase, peaking in the late period and then declining slightly at the most recent follow-up. Importantly, there was no significant difference between the fluciclovine and PSMA arms, including at the window of maximum late toxicity (6–12 months).
The investigators also reported no difference in EPIC-CP domain scores between the Fluciclovine and PSMA arms. Across incontinence, irritative, and bowel domains, the change from baseline and estimated differences between the two groups were comparable over time, reinforcing that patient-reported quality-of-life outcomes were similar regardless of tracer used.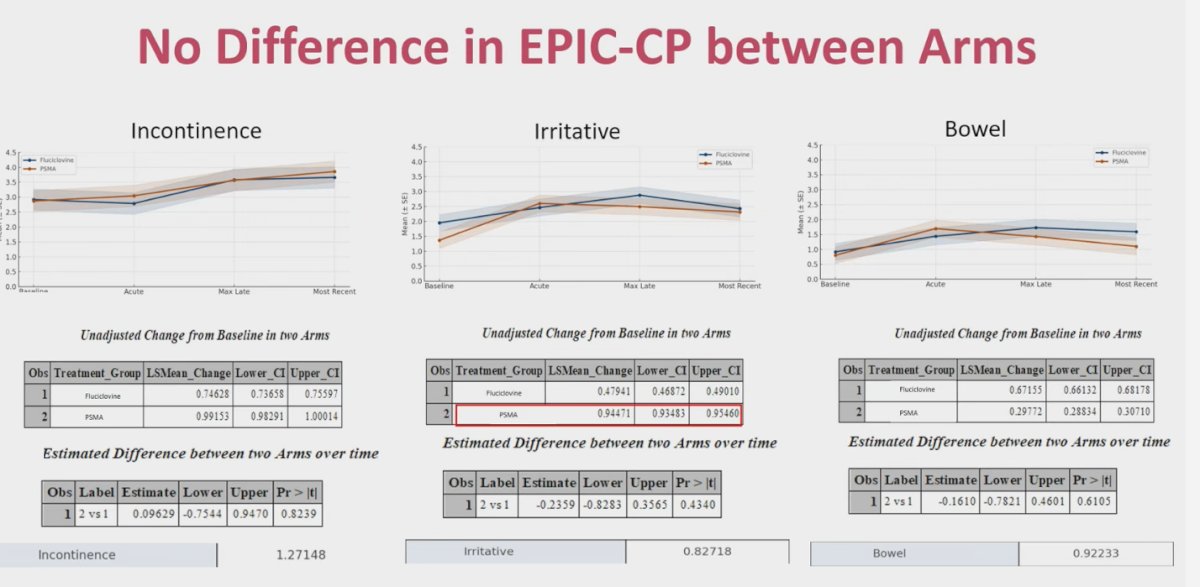
The same pattern was observed for the sexual and vitality domains, with no significant differences detected between the Fluciclovine and PSMA groups.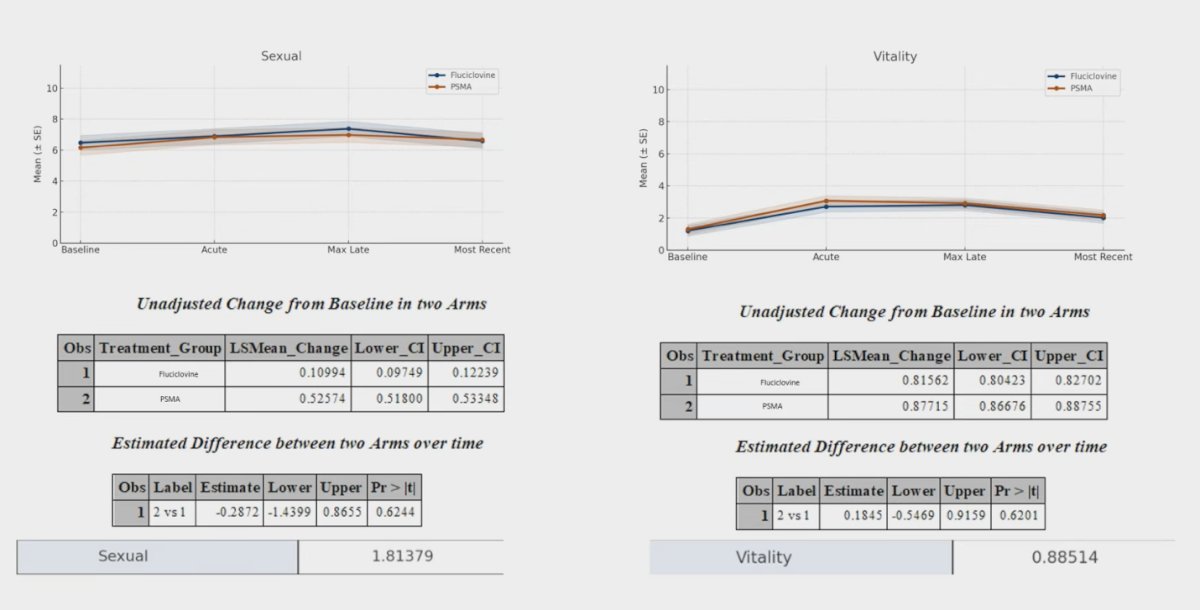
The investigators also evaluated whether outcomes differed in patients who received a radiation boost compared to those who did not. There was no difference in IPSS scores between the boost and no boost groups when analyzed in aggregate, and similarly, no significant differences were observed in bowel or sexual function outcomes.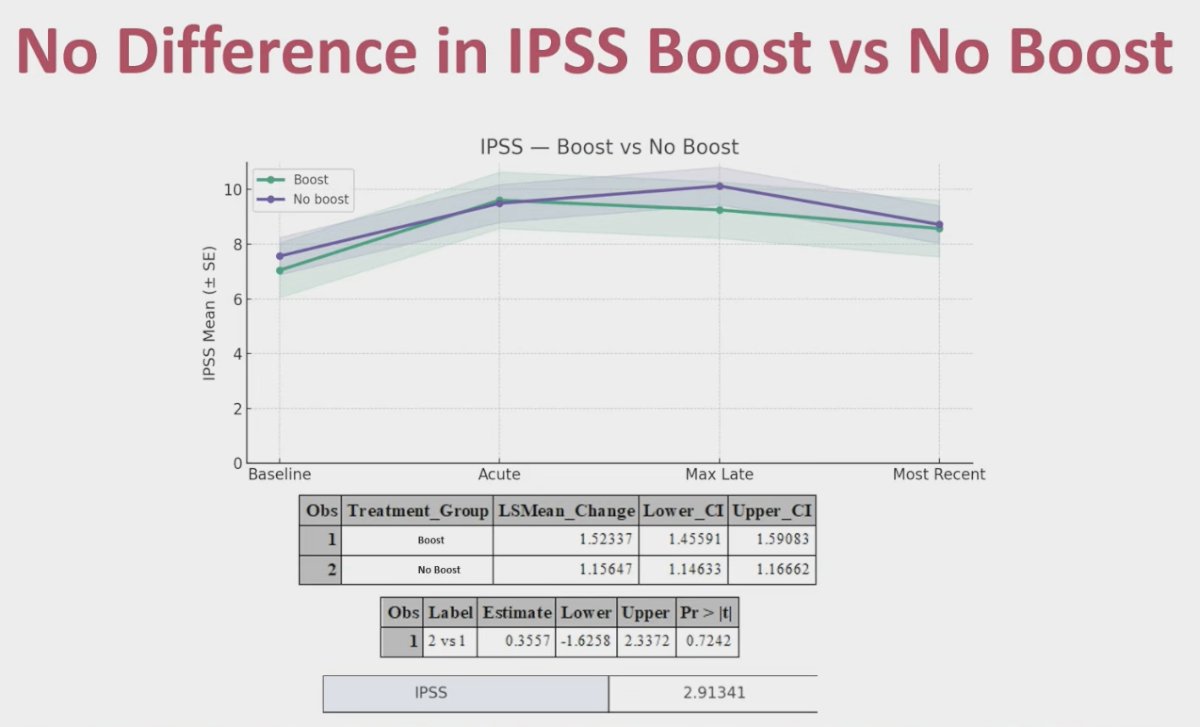
Dr. Jani’s concluding remarks were:
- In the EMPIRE-2 study, there were no significant differences between the fluciclovine and PSMA arms in IPSS or EPIC-CP patient-reported outcomes, despite a higher proportion of patients in the fluciclovine group receiving prostate or nodal boosts.
- Receipt of a radiation boost (vs. no boost) was not associated with worse patient-reported outcomes, including urinary, bowel, sexual, or vitality domains.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.
Reference: