(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting, held in San Francisco, was host to the Quality of Life Outcomes after Prostate Radiotherapy session. Dr. Brian Davis presented abstract 196 - A Randomized, Parallel Phase II Trial of Hypofractionated Proton Therapy or IMRT for Recurrent, Oligometastatic Prostate Cancer with Pelvic and/or Para-aortic Lymph Node Involvement Following Primary Localized Treatment with Radiotherapy.
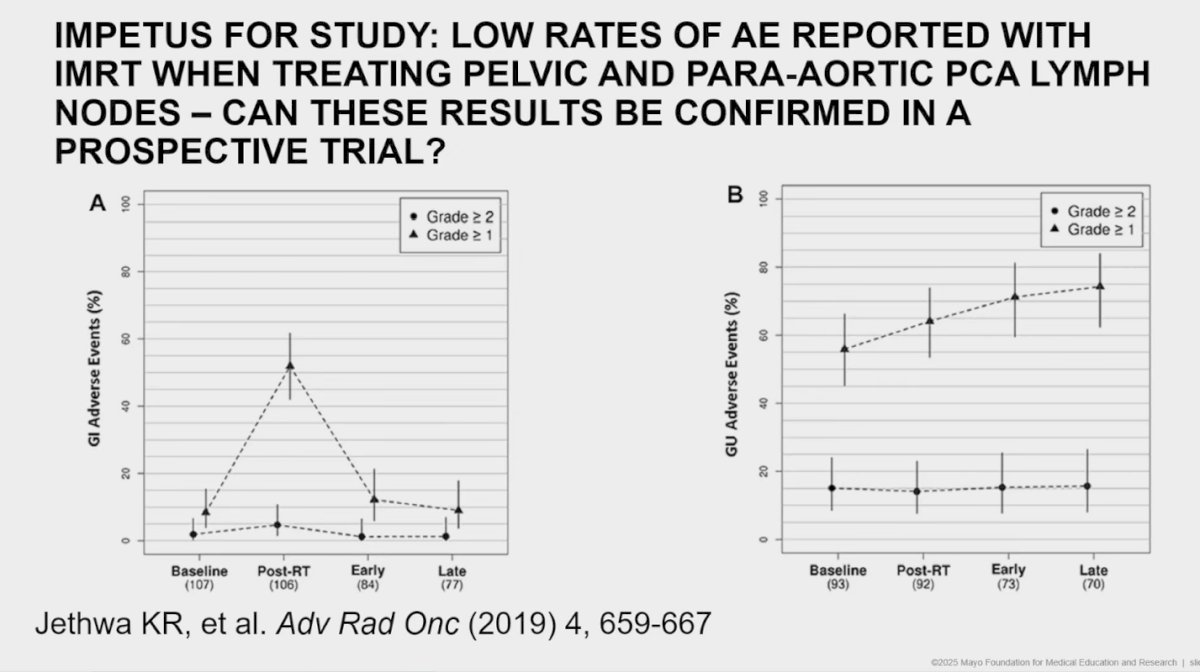
Dr. Davis began by highlighting the impetus for the study, noting that prior retrospective data that they published six years ago suggested low rates of gastrointestinal (GI) and genitourinary (GU) adverse events with IMRT when treating pelvic and para-aortic prostate cancer lymph nodes. However, whether these encouraging findings could be replicated in a prospective trial remained an open question.
He further emphasized a recently published study (PEACE V-STORM), which compared metastasis-directed therapy (MDT) using SBRT to PET-avid lymph nodes versus elective nodal radiotherapy (ENRT). The trial demonstrated that ENRT improved both biochemical relapse-free survival (BRFS, HR 0.62; 95% CI 0.48–0.80; p=0.014) and metastasis-free survival (MFS, HR 0.62; 80% CI 0.44–0.86; p=0.063) compared with MDT alone, suggesting a strong rationale for ENRT in patients with para-aortic nodal involvement.1

Dr. Davis highlighted that the study aimed to determine whether moderate hypofractionated (MHF) pelvic and/or para-aortic radiotherapy (RT) for recurrent prostate cancer with pelvic (N1) or para-aortic (M1a) nodal involvement increases patient-reported genitourinary (GU) or gastrointestinal (GI) toxicity compared to conventionally fractionated RT.
This was a randomized, parallel phase II trial evaluating both proton therapy and IMRT. Patients were randomized 2:1 to moderate hypofractionation (39 Gy in 15 fractions) versus conventional fractionation (45 Gy in 25 fractions), with a simultaneous integrated boost to PET-avid nodal recurrences (48 Gy in 15 fractions or 56.25 Gy in 25 fractions). Pelvic nodal fields were treated according to 2021 NRG guidelines, and all patients received concomitant androgen deprivation therapy (ADT) for 12–18 months.
Eligibility criteria for patient enrollment were:
- Prior prostate or post-radical prostatectomy bed RT, with or without pelvic nodal RT, for local/regional prostate cancer
- Detectable PSA with pelvic and/or para-aortic nodal recurrence only, diagnosed by prostate-specific PET scan (biopsy confirmation recommended)
- Biopsy of clinically involved lymph node for confirmation (recommended).
- ECOG PS ≤ 1
The primary endpoints of the study were early and late GI and GU toxicities greater than grade 3, assessed at 3 and 24 months. Secondary endpoints included the incidence of late grade ≥2 GI and/or GU toxicities following completion of radiotherapy, acute grade >3 toxicities within 3 months, and a direct comparison of late grade ≥3 GI and GU toxicity rates between the two treatment schedules. The study schema is presented below.
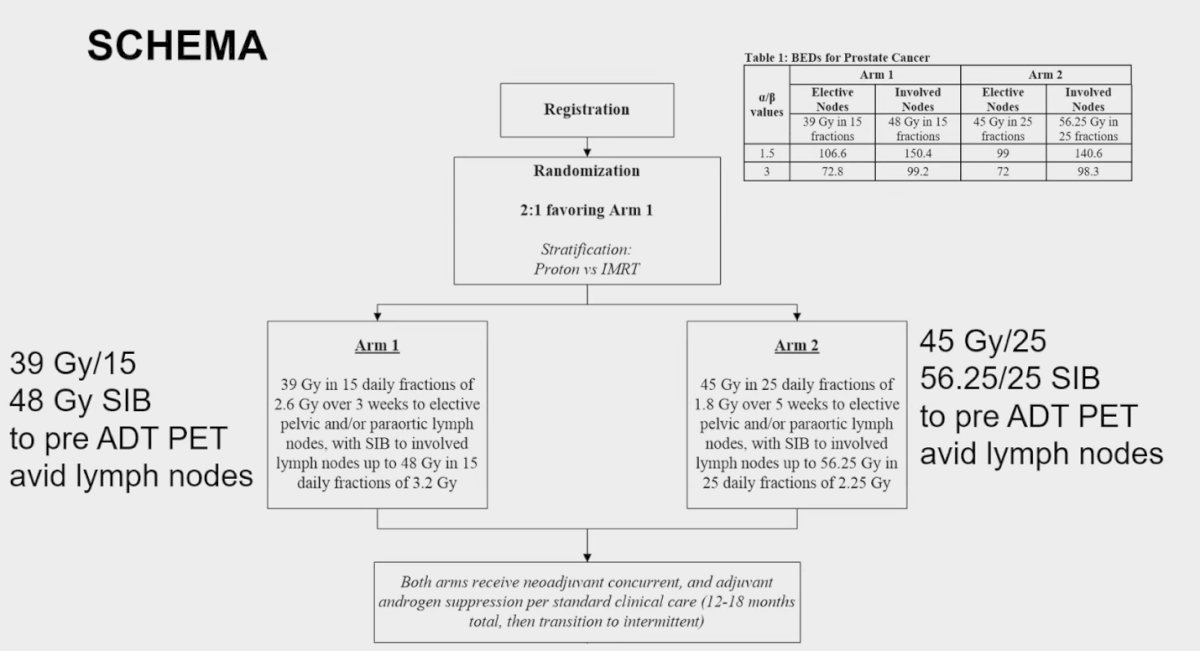
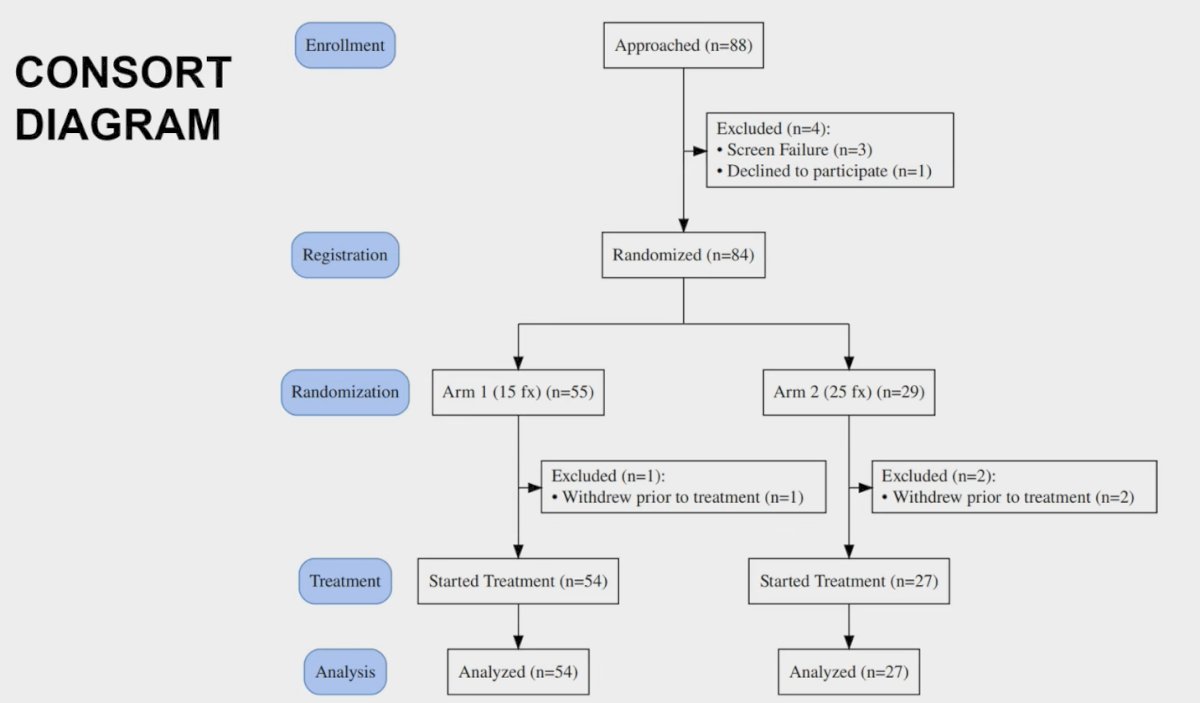
Dr. Davis highlighted that the study was designed using an α/β ratio of 3, consistent with prostate cancer radiobiology. The study was powered at 89% to detect a ≥5% toxicity rate in Arm 1 and had 92% power to identify a ≥2% toxicity rate in the same arm. The study randomized 84 patients and three ended up being excluded from the analysis, the CONSORT diagram is presented below.
Patients underwent staging with PET and MRI pelvis (≤180 days before ADT) and PSA/testosterone (≤90 days). Protocol required ADT for 12–18 months, with RT starting within 6 months of consent. Patients were randomized to 25 fractions (5 weeks) or 15 fractions (3 weeks) with concomitant ADT, and study follow-up extended to 5 years.
Toxicities were assessed using CTCAE v4.0 and QoL with EPIC-26. Monitoring included weekly assessments during treatment, active follow-up at the end of RT and at 3, 6, 12, 18, and 24 months, and extended event monitoring every 6 months through year 5.
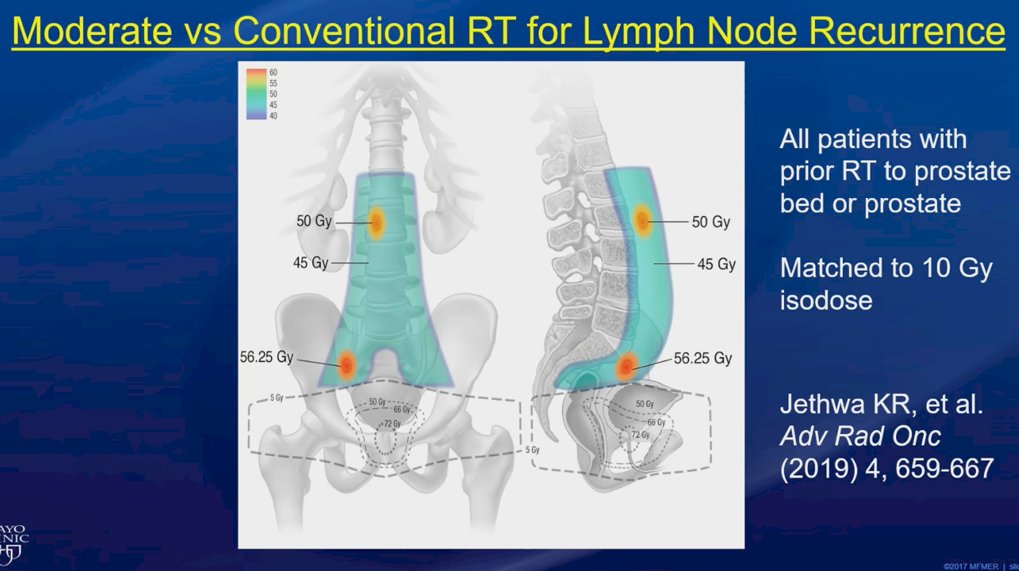
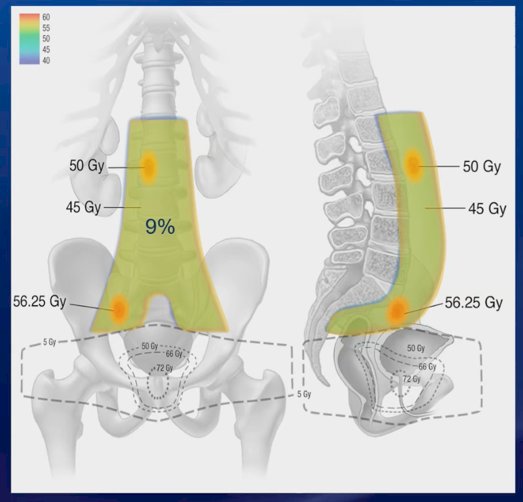
An example treatment plan was shown for patients with nodal recurrence following prior prostate or prostate bed radiotherapy. The isodose distribution illustrates elective nodal coverage to 45–50 Gy, with a simultaneous integrated boost up to 56.25 Gy to PET-avid nodal recurrences. The lower isodose lines (figure below) correspond to the original post-prostatectomy field, demonstrating how nodal recurrences are encompassed within the extended para-aortic fields while respecting prior treatment volumes.
Dr. Davis noted that patient selection for proton therapy was influenced by several factors, including institutional availability and patient preference. Proton therapy offers the advantage of reduced radiation exposure to surrounding organs compared to IMRT, highlighting its potential role in minimizing treatment-related toxicity.

A total of 81 patients were enrolled between January 2020 and August 2023, including 74 post-radical prostatectomy and 7 post-primary radiotherapy cases, with a median follow-up of 38.5 months (IQR 30.3–48.4) when the abstract was submitted, but over 2 years now. Of these, 54 patients (22 proton, 32 IMRT) were randomized to the moderate hypofractionated (MHF) arm and 27 patients (12 proton, 15 IMRT) to the conventional fractionation (CF) arm. Baseline PSA levels had a median of 2.2 ng/mL (IQR 0.9–4.6; range 0.19–19.5) and a mean of 3.9 ng/mL (SD 4.4). In terms of treatment fields, 62 patients received pelvic irradiation only, 18 received both pelvic and para-aortic fields, and 1 patient was treated to the para-aortic region alone.
In terms of PET imaging, the majority of patients underwent choline PET (65.4%), followed by PSMA (17.3%), combined PSMA and choline (16.0%), and fluciclovine (1.2%). Pathologic confirmation of nodal involvement was obtained in 43% of cases, most commonly via CT-guided biopsy (33%) or prior pN1 disease (10%).
Dr. Davis reported that no patients in either treatment arm experienced grade 3 genitourinary or gastrointestinal acute toxicities. Overall, grade 1+ and grade 2+ acute GI/GU toxicities occurred in 43.2% and 4.9% of patients, respectively. Within the moderate hypofractionation (MHF) arm, there was a significant difference in the occurrence of grade 1+ acute toxicities between proton therapy and IMRT (p=0.04). However, no significant differences were observed between modalities in the conventional fractionation (CF) arm (p=0.34) or for grade 2+ acute toxicities in either the MHF (p=0.14) or CF (p=0.36) arms.

Notably, cause-specific survival at 4 years was 97%, while relapse-free survival was 52%. In terms of dosimetric outcomes within the MHF arm, the mean small bowel dose was substantially lower with protons at 4.45 Gy (SD = 3.2 Gy) compared to 14.3 Gy (SD = 4.9 Gy) with IMRT, underscoring the potential advantage of proton therapy in reducing off-target radiation exposure.
Dr. Davis concluded his presentation with the following key remarks:
- Moderate hypofractionation (39 Gy/15 fractions with SIB to 48+ Gy) for nodal prostate cancer recurrence showed acceptably low acute toxicity, comparable to conventional fractionation.
- Both IMRT and proton therapy were safe options, with no major differences in clinically meaningful GU/GI toxicity observed.
- MHF with SIB appears promising as an approach for elective nodal radiation therapy (ENRT), including treatment of para-aortic lymph nodes.
- Proton therapy reduced radiation dose to abdominal structures compared to IMRT, though without translating into significant clinical toxicity differences in this trial.
- Findings support the role of ENRT in select patients with recurrent nodal prostate cancer and provide a basis for future evaluation of hypofractionated regimens
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC) Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
- Ost P, Siva S, Brabrand S, Dirix P, Liefhooghe N, Otte FX, Gomez-Iturriaga A, Everaerts W, Shelan M, Conde-Moreno A, López Campos F, Papachristofilou A, Guckenberger M, Scorsetti M, Zapatero A, Villafranca Iturre AE, Eito C, Couñago F, Muto P, Duthoy W, Mach N, Fonteyne V, Moon D, Thon K, Mercier C, Achard V, Stellamans K, Goetghebeur E, Reynders D, Zilli T. Salvage metastasis-directed therapy versus elective nodal radiotherapy for oligorecurrent nodal prostate cancer metastases (PEACE V-STORM): a phase 2, open-label, randomised controlled trial. Lancet Oncol. 2025 Jun;26(6):695-706. doi: 10.1016/S1470-2045(25)00197-4. Epub 2025 May 5. PMID: 40339593.