(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session16 - GU 4: Quality of Life Outcomes after Prostate Radiotherapy. Dr. James Yu discussed quality of life results from NRG-GU005: A Phase III Trial of Stereotactic Body Radiotherapy (SBRT) vs. Hypofractionated Intensity-Modulated Radiation Therapy (IMRT) for Localized Intermediate Risk Prostate Cancer.
Dr. Yu began by highlighting that moderately hypofractionated IMRT (MH-IMRT) has been the standard of care for prostate cancer since RTOG 0415 and other landmark studies.1 At the time this trial was designed, ultrahypofractionated SBRT had not yet been directly compared to MH-IMRT, and concerns remained regarding potential toxicity. For men with intermediate-risk prostate cancer, quality of life is considered just as important as traditional oncologic outcomes. Prior patient-level meta-analyses suggested that SBRT may result in less clinically significant decline in patient-reported bowel and urinary irritative/obstructive function two years post-treatment.2
The NRG-GU005 trial is a randomized, non-blinded phase III study comparing image-guided SBRT with MH-IMRT in patients with localized intermediate-risk PCa. While the primary endpoint focused on oncologic outcomes, the investigators emphasized that QOL is equally important in this setting. This analysis reported secondary endpoints, specifically evaluating HRQOL in patients treated with SBRT.1
Patients were randomized 1:1 to receive either SBRT (36.25 Gy in 5 fractions) or MH-IMRT (70 Gy in 28 fractions or 60 Gy in 20 fractions), with stratification by Gleason score, PSA, and use of rectal balloons or hydrogel rectal spacers (rectal manipulation). HRQOL was assessed using the Expanded Prostate Cancer Index Composite (EPIC-26) at baseline, 12, and 24 months post-treatment.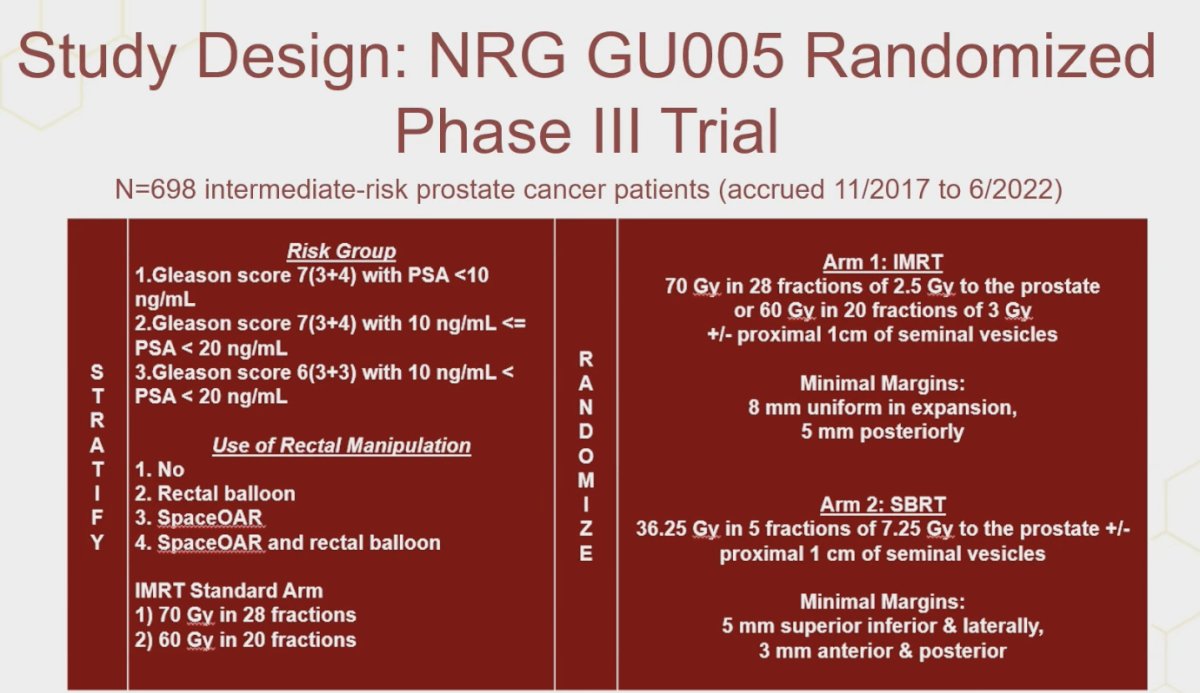
Secondary patient-reported outcomes included the incidence of a minimal clinically important decline (MCID) in urinary irritative/obstructive (UIO) and bowel domains at 1 year, and urinary incontinence, sexual, and hormonal domains at 1 and 2 years post-treatment. MCID thresholds were predefined as >5 points for UIO, >6 for urinary incontinence, >10 for sexual, and >4 points for bowel and hormonal domains. The investigators employed a repeated measures mixed-effects model for each EPIC-26 domain, adjusting for baseline score, treatment arm, stratification factors, T-stage, age, and race.
In NRG-GU005, radiotherapy details included CTV defined as the prostate ±1 cm of proximal seminal vesicles. MH-IMRT was delivered as 70 Gy in 28 fractions or 60 Gy in 20 fractions, with CTV to PTV expansion of 8 mm except 5 mm posteriorly. SBRT was delivered as 36.25 Gy in 5 fractions (2–3 per week), with a 5 mm expansion except 3 mm posteriorly and anteriorly. Importantly, the maximum dose to PTV without urethral visualization was capped at 38.78 Gy, with urethral visualization and contouring required if exceeded, and acceptable variation defined as 43.5 Gy.
Patient characteristics were well balanced between the two arms, with no significant differences observed in baseline demographics. The median age was 68 years, and rectal manipulations such as rectal balloon or SpaceOAR were used in a similar proportion of patients across groups. Overall, the trial randomized 698 patients, of whom 345 were assigned to MH-IMRT and 353 to SBRT as illustrated below.
The statistical plan focused on patient-reported outcomes, specifically assessing the frequency of an MCID at 1 and 2 years compared to baseline. Individual MCID, being more sensitive to treatment-related differences than group mean scores, was used to evaluate post-treatment quality of life relative to baseline, as shown below.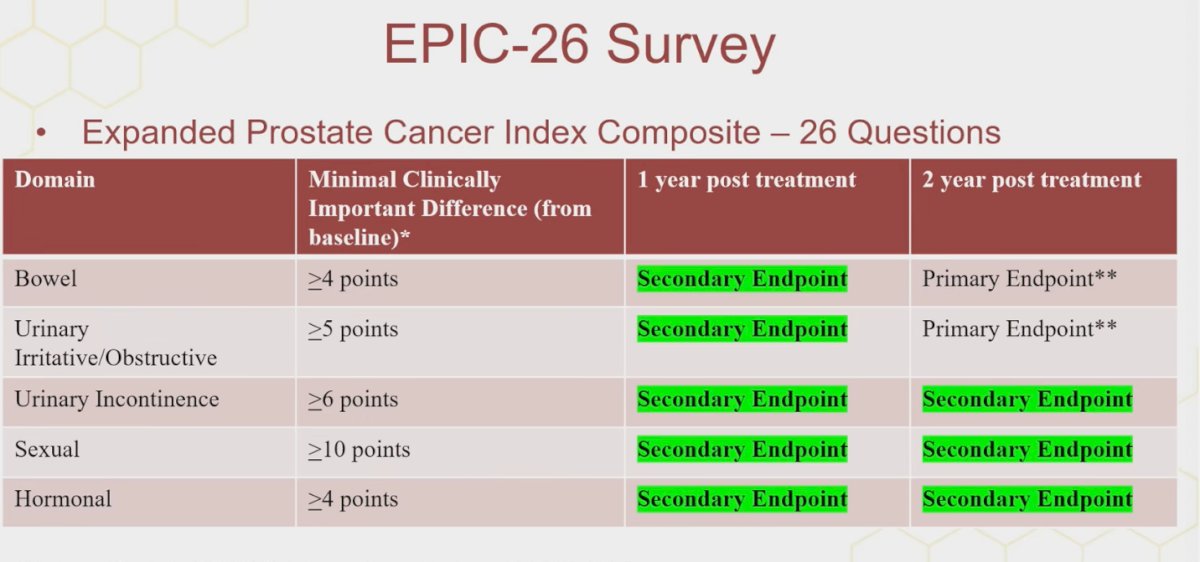
An exploratory longitudinal analysis was also performed, conducted separately for each domain score using longitudinal linear modeling. Models were adjusted for baseline domain score, treatment arm, stratification factors (risk group using Gleason score and PSA, rectal manipulation), T-stage, age, and race.
Dr. Yu highlighted that compliance with EPIC questionnaires was excellent, with over 80% completion at both year 1 and year 2. Importantly, baseline EPIC scores were well balanced between treatment arms across bowel, urinary irritation, urinary incontinence, sexual, and hormonal domains, ensuring a fair comparison for subsequent PRO analyses.

At one year post-treatment, significantly fewer patients in the SBRT arm experienced a minimal clinically important decline compared to those in the MH-IMRT arm in both the bowel (33% vs 46%, p=0.002) and sexual (34% vs 44%, p=0.026) domains, as shown below.
At two years, significantly fewer patients in the SBRT arm experienced a minimal clinically important decline in the urinary incontinence domain compared with those in the MH-IMRT arm (26% vs 35%, p=0.023).
Moreover, longitudinal analysis of the urinary incontinence domain demonstrated a significant treatment effect favoring SBRT, with a least square mean difference of 2.91 (95% CI: 0.85–4.97; p=0.0058). By contrast, no significant treatment effect was observed in the sexual or hormonal domains.
Dr. Yu presented the investigator-reported toxicity data, which overall favored SBRT. Treatment-related grade ≥3 genitourinary toxicities occurred more frequently in the MH-IMRT arm (2.5% vs. 0.6%, p=0.04). Rectal hemorrhage of any grade was also higher in the MH-IMRT arm (17.3% vs. 10.5%, p=0.01).
Additionally, investigator-reported fatigue of any grade was significantly more common with MH-IMRT compared to SBRT (50.8% vs. 39.2%, p=0.0025) as illustrated below.
Lastly, Dr. Yu compared these results with findings from the PACE-B trial, the other large study directly comparing SBRT to MH-IMRT. He highlighted that while both studies assessed patient-reported outcomes, there were slight differences in the definitions of MCID. Despite these methodological differences, both trials consistently demonstrated lower rates of urinary incontinence-related decline with SBRT compared to MH-IMRT, underscoring the potential quality-of-life benefit of SBRT in this setting.3

Dr. Yu concluded the presentation with the following take-home messages:
- Significantly fewer SBRT patients experienced minimally clinically important declines in sexual and bowel HRQOL at 1 year compared to MH-IMRT.
- At 2 years, fewer SBRT patients experienced declines in urinary incontinence HRQOL, favoring SBRT over MH-IMRT.
- Longitudinal analysis also favored SBRT over MH-IMRT in terms of patient-reported urinary incontinence-related quality of life
- These findings suggest improved HRQOL with SBRT compared to IMRT in localized intermediate-risk prostate cancer.
- SBRT is very safe for the treatment of intermediate-risk prostate cancer and is associated with low rates of investigator-reported toxicity
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September
Related content: Patient-Reported Outcomes in the NRG-GU005 Prostate Cancer Trial - James Yu
Reference:
- Lee WR, Dignam JJ, Amin MB, Bruner DW, Low D, Swanson GP, Shah AB, D'Souza D, Michalski JM, Dayes IS, Seaward SA, Hall WA, Nguyen PL, Pisansky TM, Faria SL, Chen Y, Rodgers JP, Sandler HM. Long-Term Analysis of NRG Oncology RTOG 0415: A Randomized Phase III Noninferiority Study Comparing Two Fractionation Schedules in Patients With Low-Risk Prostate Cancer. J Clin Oncol. 2024 Jul 10;42(20):2377-2381. doi: 10.1200/JCO.23.02445. Epub 2024 May 17. PMID: 38759121; PMCID: PMC11377096.
- Yu JB, Cramer LD, Herrin J, Soulos PR, Potosky AL, Gross CP. Stereotactic body radiation therapy versus intensity-modulated radiation therapy for prostate cancer: comparison of toxicity. J Clin Oncol. 2014 Apr 20;32(12):1195-201. doi: 10.1200/JCO.2013.53.8652. Epub 2014 Mar 10. PMID: 24616315; PMCID: PMC3986382.
- Van As NJ, Tree AC, Brand DH, et al. Hypofractionated stereotactic body radiotherapy versus conventionally fractionated or moderately hypofractionated radiotherapy for prostate cancer (PACE-B): 2-year urinary and bowel patient-reported outcomes from a randomized, controlled, phase 3 trial. N Engl J Med. 2024;391(15):1413-1425. doi:10.1056/NEJMoa2400483