(UroToday.com) The 2025 ASTRO annual meeting featured a prostate cancer radiation toxicity session and a presentation by Dr. Jonathan Massachi discussing a secondary analysis of the MIRAGE trial1 assessing dosimetric data of post-radiotherapy sexual dysfunction in patients receiving definitive stereotactic body radiotherapy for prostate cancer. Preservation of sexual function following radiation therapy for prostate cancer remains a significant goal for many men choosing this treatment pathway. Aggressive margin reduction with MRI-guided radiotherapy has been shown to reduce toxicity in patients receiving stereotactic body radiotherapy, but nearly 45% of men still experienced a significant decline in sexual function in the 2 years of treatment. Dr. Massachi and colleagues performed a secondary analysis of the MIRAGE phase III randomized trial,1 which compared CT-guided stereotactic body radiotherapy with MRI-guided stereotactic body radiotherapy, to evaluate potential predictors of sexual dysfunction.
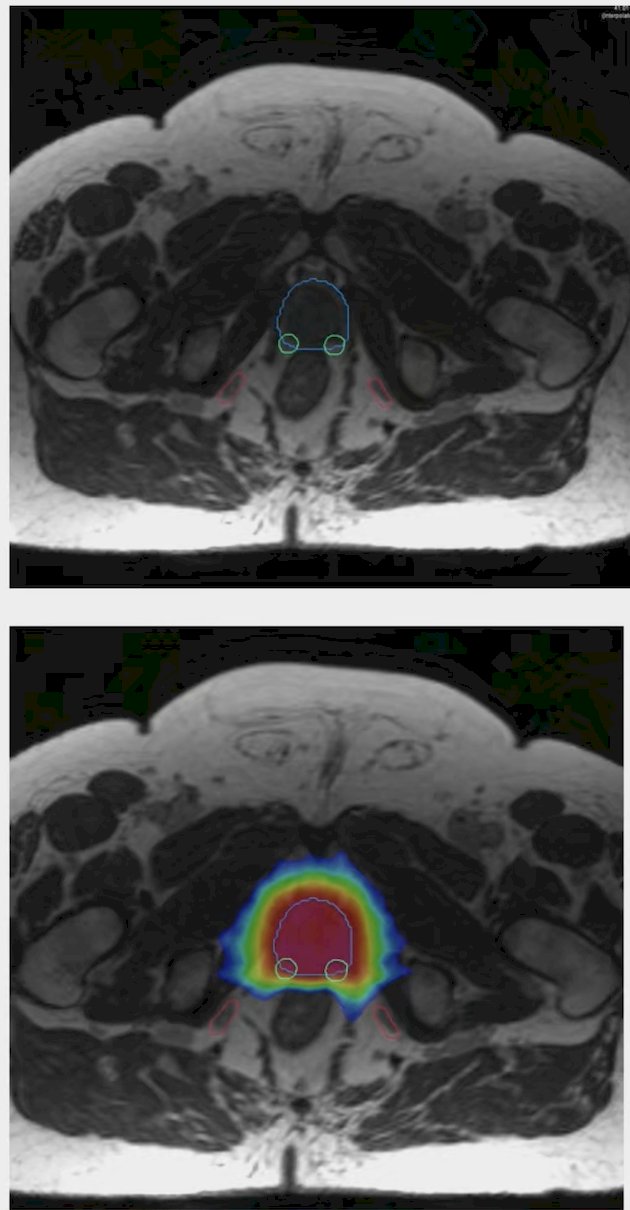
Sexual function was scored based on Expanded Prostate Cancer Index sexual function (EPIC-26 SF) domain, with a 24 point decline being considered clinically significant. The internal pudendal artery and neurovascular bundle were contoured on radiotherapy planning CT or low-field MRI scans using a rigid registration to a diagnostic MRI:
Dosimetric profiles were then extracted and statistical analysis was performed using non-parametric rank-sum and Chi square test of proportions to assess for differences between groups where appropriate.
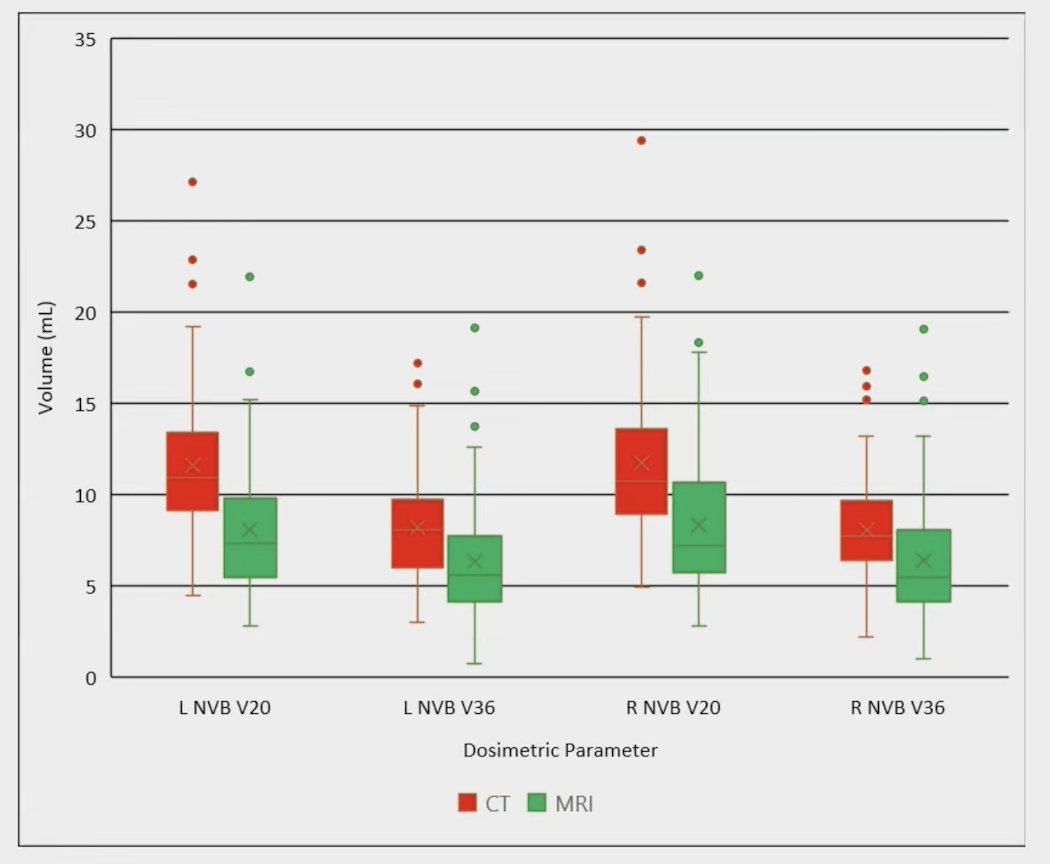
A total of 127 patients had both EPIC-26 sexual function scores and analyzable dosimetry (CT n = 61; MRI n = 66). Overall, 65% of participants received ADT and 66% had recovered to a normal testosterone level by 24 months. There were 31% and 29% of patients in the CT and MRI groups, respectively, that experienced a significant decline in EPIC-26 SF at 2 years. In the CT group, bilateral neurovascular bundle V20Gy and V36Gy were significantly higher than the MRI group, but internal pudendal artery doses were not significantly different between study arms:
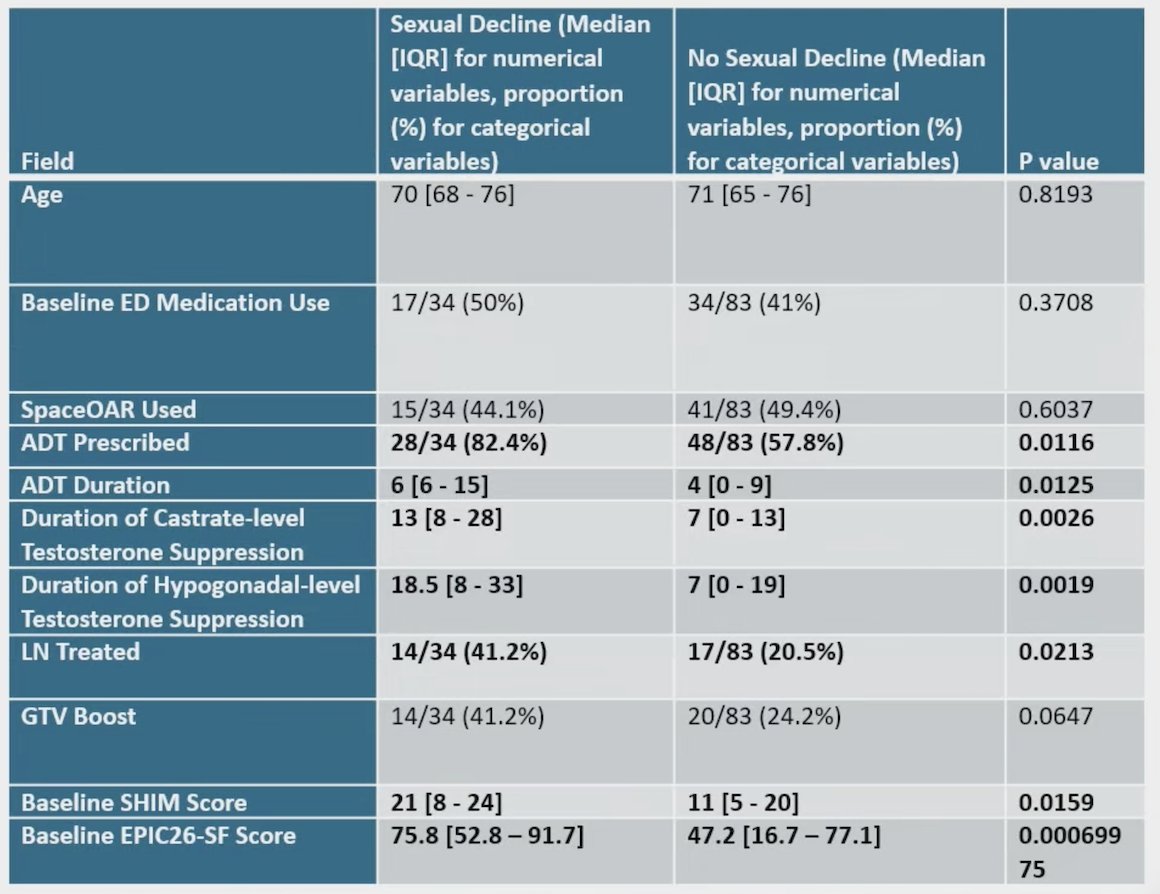
ADT use and duration, pelvic nodal radiation, and baseline EPIC-26 SF were significantly associated with a large decline in EPIC-26 SF by two years. However, there were no significant differences across multiple dosimetric measures (D0.035, V20Gy, V36Gy, Dmean) when comparing patients with significant versus non-significant declines in EPIC-26:
Dr. Massachi concluded his presentation discussing a secondary analysis of the MIRAGE trial assessing dosimetric data of post-radiotherapy sexual dysfunction in patients receiving definitive stereotactic body radiotherapy with the following take home points:
- MRI-guided stereotactic body radiotherapy without explicit sexual structure sparing resulted in lower doses to the neurovascular bundles than CT-guided treatment, but no significant difference in internal pudendal arteries
- Despite this decreased dose between study arms, patients who experienced significant sexual function decline had no significant dosimetric differences for these structures
- Explicit sparing of sexual function-associated structures may be needed to avoid exceeding the threshold for causing injury
Presented by: Jonathan Massachi, MD, UCLA, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025
References: