(UroToday.com) The 2025 ASTRO annual meeting featured a prostate cancer session and a presentation by Dr. T. Martin Ma discussing sequencing short term hormonal therapy with radiotherapy for prostate cancer. Dr. Ma started his presentation by asking several pre-session questions. The first question was “For a patient with unfavorable intermediate risk prostate cancer needing a 6-month course of ADT, when will you initiate ADT?”
- > 3 months before radiotherapy starts: 0%
- ~2-3 months before radiotherapy starts: 4%
- ~1-2 months before radiotherapy starts: 28%
- Around the same time as radiotherapy starts: 68%
- I do not have a defined timeline: 0%
The second question was “For a patient with high risk prostate cancer needing an 18 to 24-month course of ADT, when will you initiate ADT?”
- > 3 months before radiotherapy starts: 4%
- ~2-3 months before radiotherapy starts: 17%
- ~1-2 months before radiotherapy starts: 35%
- Around the same time as radiotherapy starts: 43%
- I do not have a defined timeline: 0%
Sequencing of systemic therapies with radiotherapy has been associated with differential survival benefits in multiple malignancies. Sequencing of ADT with radiotherapy (proportion of neoadjuvant versus adjuvant) has been variable across different trials, including:
- TROG and Canadian trials: favor prolonged neoadjuvant ADT
- NRG/RTOG trials: favor mixed neoadjuvant/concurrent ADT
- EORTC trials: favor concurrent/adjuvant ADT
To date, data are limited in directly comparing ADT sequencing strategies, with only two randomized trials ever comparing ADT sequencing:
- RTOG 9413:1 a 2x2 randomization of prostate-only radiotherapy versus whole pelvis radiotherapy, and neoadjuvant/concurrent versus adjuvant ADT (total of 4 months). This trial showed that there is a significant interaction between radiotherapy field size and ADT sequencing
- Ottawa 0101:2 neoadjuvant (4 months) + concurrent (2 months) versus concurrent (2 months) + adjuvant (4 months); with prostate-only radiotherapy. This trial showed no statistically significant difference in biochemical recurrence free survival between the two arms
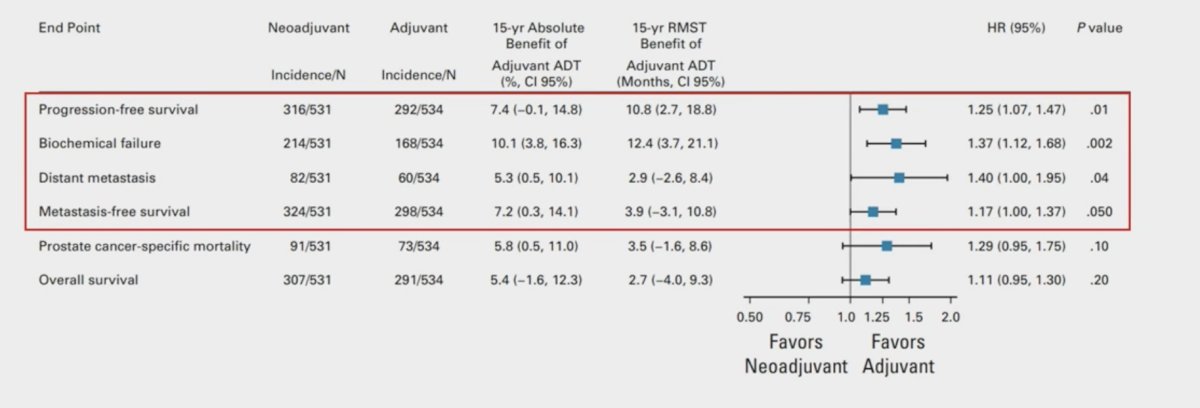
In a pooled individual patient data analysis of RTOG 9413 and Ottawa 0101 assessing prostate only radiotherapy,3 there was a significant benefit of utilizing adjuvant ADT:
Moreover, in the MARCAP Consortium meta-analysis4 (3 trials of neoadjuvant ADT extension and 4 trials of adjuvant ADT prolongation), there was no benefit in neoadjuvant ADT extension, but metastasis free survival and overall survival benefits with adjuvant ADT prolongation.
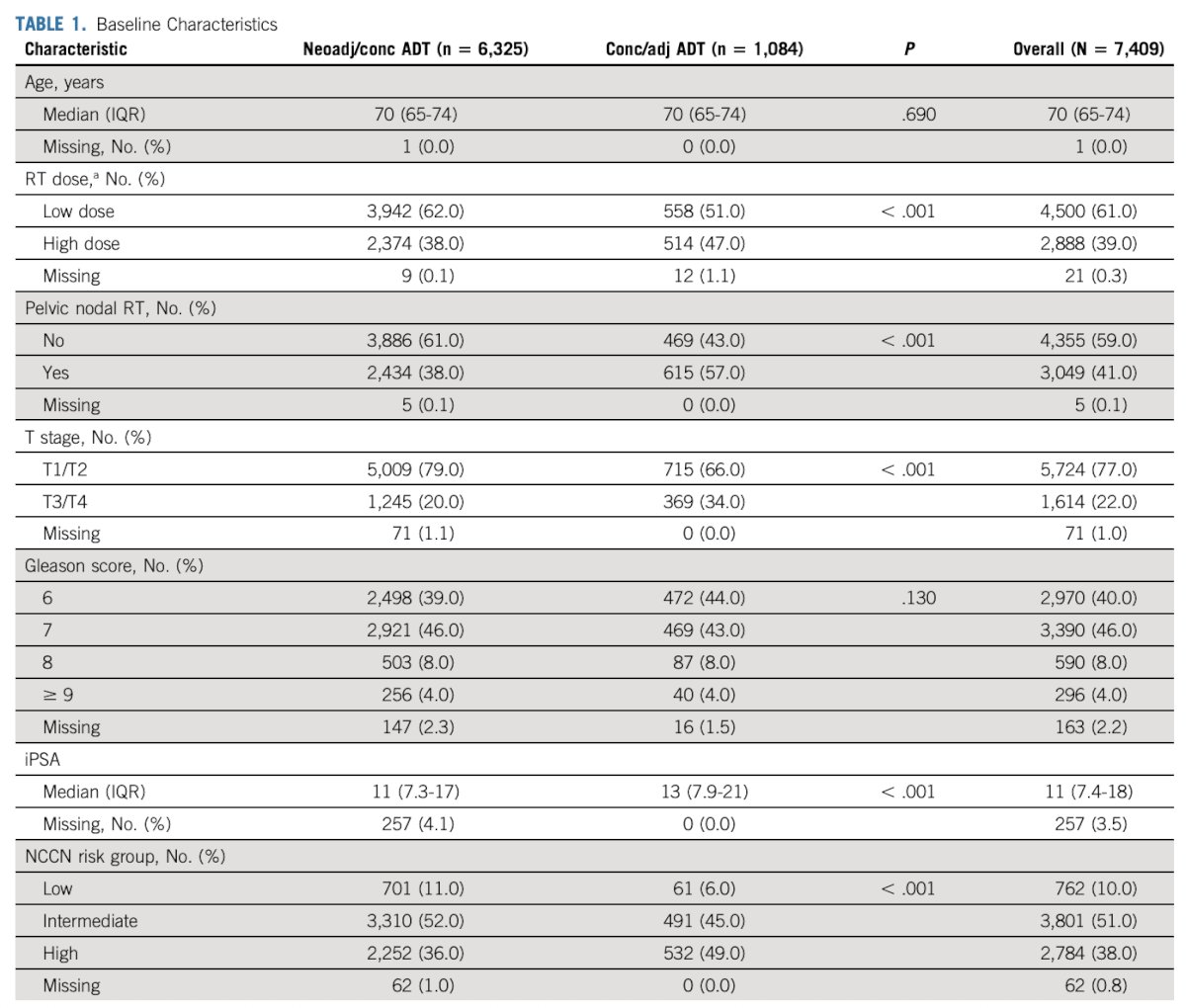
In the SANDTORM meta-analysis,5 Dr. Ma notes that the objective was to investigate the impact of ADT sequencing for men receiving ADT for localized prostate cancer with prostate only radiotherapy or whole pelvis radiotherapy. The primary endpoint was metastasis free survival. This was an individual patient data analysis from 12 randomized trials in the MARCAP Consortium that included patients receiving neoadjuvant/concurrent or concurrent/adjuvant short term ADT (4-6 months) with radiotherapy. There were 7,409 patients in the study, including 6,325 neoadjuvant/concurrent and 1,084 concurrent/adjuvant ADT, with a median follow-up of 10.2 years. Inverse probability of treatment weighting (IPTW) with propensity scores derived from age, initial PSA, Gleason score, T stage, radiotherapy dose, and mid-trial enrollment year. IPTW-adjusted Cox regression models and IPTW-adjusted Fine and Gray competing risk models were used. Restricted mean time lost (RMTL, for competing risk data) was used as an alternative measure of the treatment effect. Baseline characteristics for the meta-analysis are highlighted in the following table:
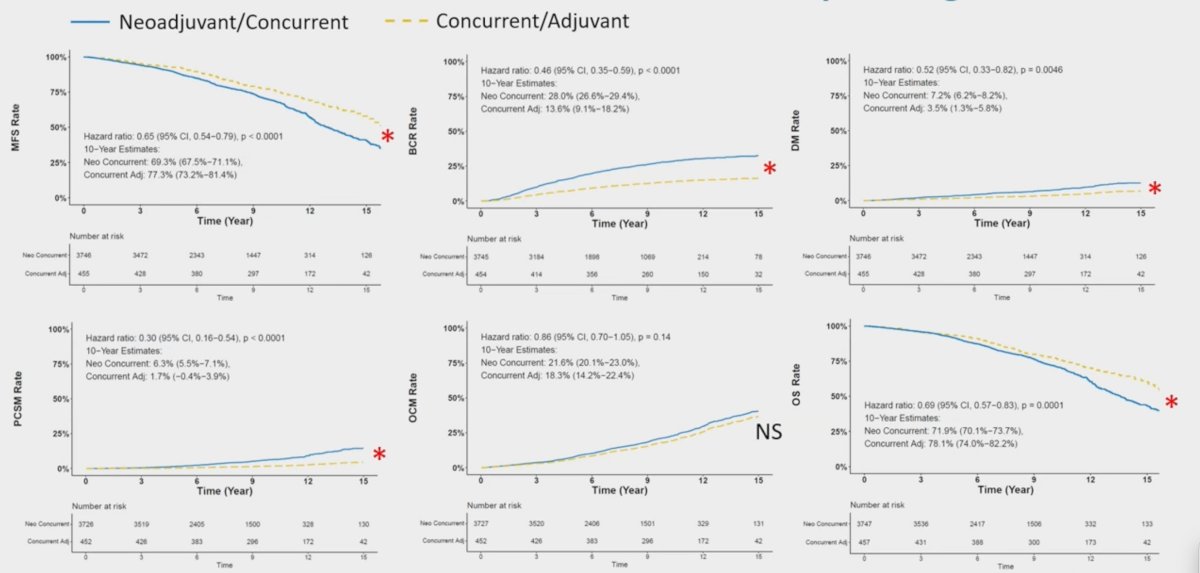
Dr. Ma notes that they found that there was a significant interaction between ADT sequencing and radiotherapy field size (pelvic only versus whole pelvis radiotherapy) for biochemical recurrence, distant metastasis, prostate cancer specific mortality, other cause mortality, metastasis free survival, but not overall survival after IPTW adjustment (p-interaction < 0.02 for all except p = 0.20 for overall survival). Subsequent analyses were dichotomized into cohorts receiving prostate only radiotherapy or whole pelvis radiotherapy and performed independent analyses in each cohort per an a prior analysis plan. The following Kaplan Meier and cumulative function curves depict the associations between outcomes and ADT sequencing in prostate only radiotherapy:
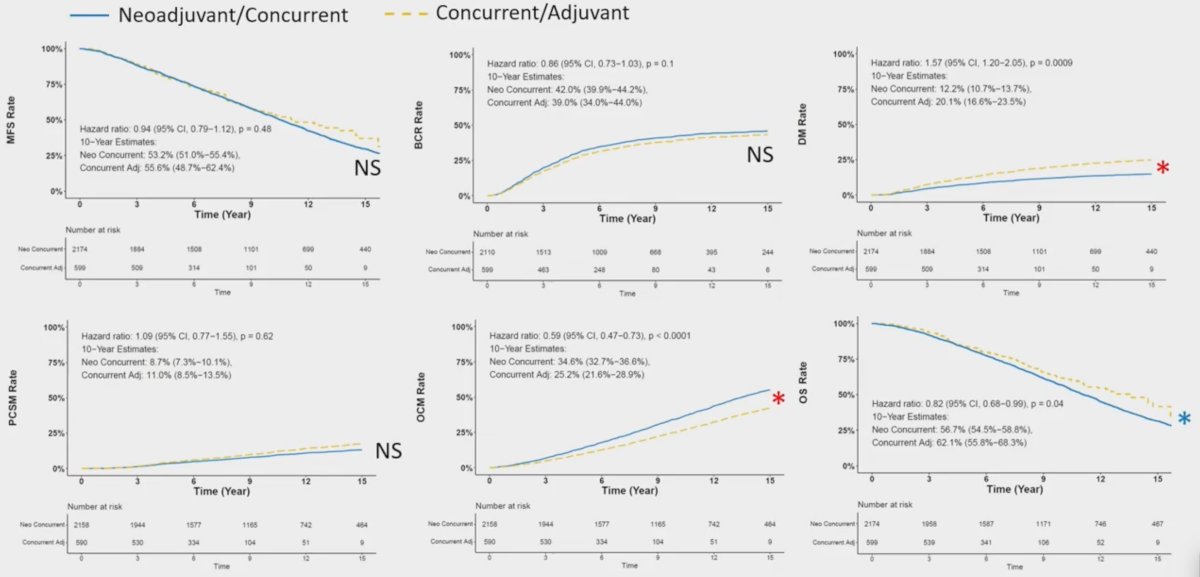
Similarly, the following Kaplan Meier and cumulative function curves depict the associations between outcomes and ADT sequencing in whole pelvis radiotherapy:
Dr. Ma notes that the adjuvant component of ADT may be beneficial regardless of radiation field size. The benefit of adjuvant ADT could be related to protracted radiotherapy-induced tumor cell death, and the continued blockade of androgen receptor-regulated DNA repair genes and radiotherapy induced neoangiogenesis may be beneficial. For whole pelvis radiotherapy, the immunologic effects of ADT may be important. ADT can increase INF-gamma production, decrease regulatory T-cell activation, and increase naïve T cell infiltration into the prostate. Whole pelvis radiotherapy may eliminate proinflammatory lymphocytes in the pelvic nodal system and periphery, and ADT immunological benefit would only occur if the ADT is given neoadjuvantly.
Dr. Ma concluded his presentation discussing sequencing short-term hormonal therapy with radiotherapy for prostate cancer with the following take home points:
- The impact of ADT sequencing on outcomes is dependent on the radiotherapy field size (pelvic only versus whole pelvis radiotherapy)
- When pelvic only radiotherapy is delivered, concurrent/adjuvant short term ADT sequencing is associated with optimal outcomes, including overall survival
- These data strongly suggest that concurrent/adjuvant ADT should be the standard of care when short term ADT and pelvic only radiotherapy are indicated
- The effects are not as clear for patients receiving whole pelvis radiotherapy, though neoadjuvant/concurrent short term ADT may be preferred given its distant metastasis benefit
- This data is most applicable to intermediate risk disease when short term ADT is indicated
Presented by: T. Martin Ma, MD, PhD, University of Washington, Seattle, WA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025
References:
- Roach M, Moughan J, Lawton CA, et al. Sequence of hormonal therapy and radiotherapy field size in unfavourable, localised prostate cancer (NRG/RTOG 9413): long-term results of a randomised, phase 3 trial. Lancet Oncol. 2018;19(11):1504-1515.
- Malone S, Roy S, Eapen L, et al. Sequencing of androgen-deprivation therapy with external-beam radiotherapy in localized prostate cancer: A phase III randomized controlled trial. J Clin Oncol. 2019;38(6):593-601.
- Spratt DE, Malone S, Roy S, et al. Prostate Radiotherapy with Adjuvant Androgen Deprivation Therapy (ADT) Improves Metastasis-Free Survival Compared to Neoadjuvant ADT: An Individual Patient Meta-Analysis. J Clin Oncol. 2021 Jan 10;39(2):136-144.
- Kishan AU, Sun Y, Hartman H, et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localized prostate cancer: An individual patient data meta-analysis. Lancet Oncol. 2022 Feb;23(2):304-316.
- Ma TM, Sun Y, Malone S, et al. Sequencing of Androgen-Deprivation Therapy of Short Duration with Radiotherapy for Nonmetastatic Prostate Cancer (SANDSTORM): A Pooled Analysis of 12 Randomized Trials. J Clin Oncol. 2023 Feb 1;41(4):881-892.