(UroToday.com) The 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting held in San Francisco, CA between September 28th and 30th, 2025, was host to an advances in localized prostate cancer session. Dr. Tamim Niazi presented the 10-year outcomes of the Prostate Cancer Study-5 (PCS5), a non-inferiority, phase III trial of conventional versus hypofractionated radiotherapy for high-risk prostate cancer.
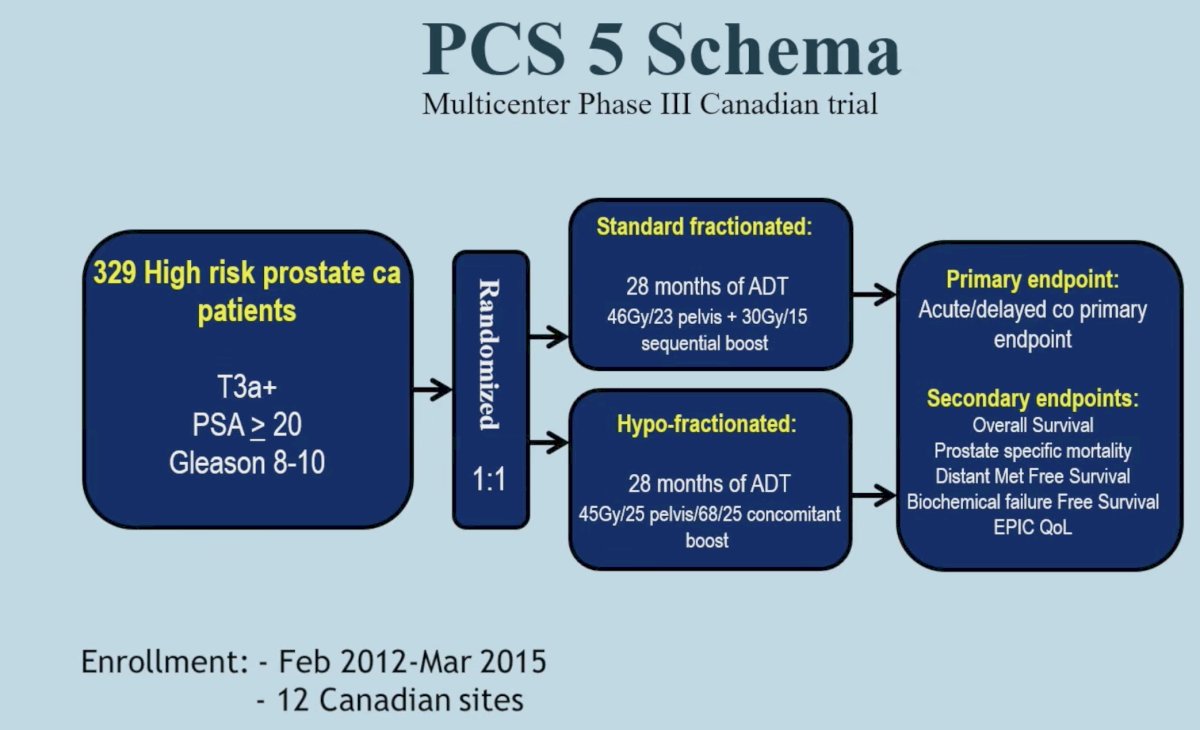
The PCS5 trial is a Canadian multicenter, open-label, phase III randomized trial that included men with histologically proven, clinically localized prostate cancer with ≥1 high-risk feature(s) (cT3/T4, Gleason score ≥8, and/or PSA >20). All eligible patients received 28 months of ADT and were randomized 1:1 to :
- Conventionally fractionated radiotherapy (76 Gy/38 Fx to the prostate plus 46 Gy/23 Fx to the pelvic lymph nodes)
- Hypofractionation (68 Gy/25 Fx to the prostate plus 45 Gy/25 Fx to the pelvic lymph nodes)
The 10-year survival outcomes from this study were published earlier this year in European Urology.1
The study cohort characteristics are summarized in the table below. The median patient age was 72 years, and the median serum PSA level was 11.6 ng/ml. 85% of patients had Gleason Score ≥8 disease (HFRT arm: 82%; CFRT arm: 85%). 61% of patients received intensity-modulated radiation therapy (IMRT) and 39% received 3-dimensional conformal radiation therapy (3D-CRT).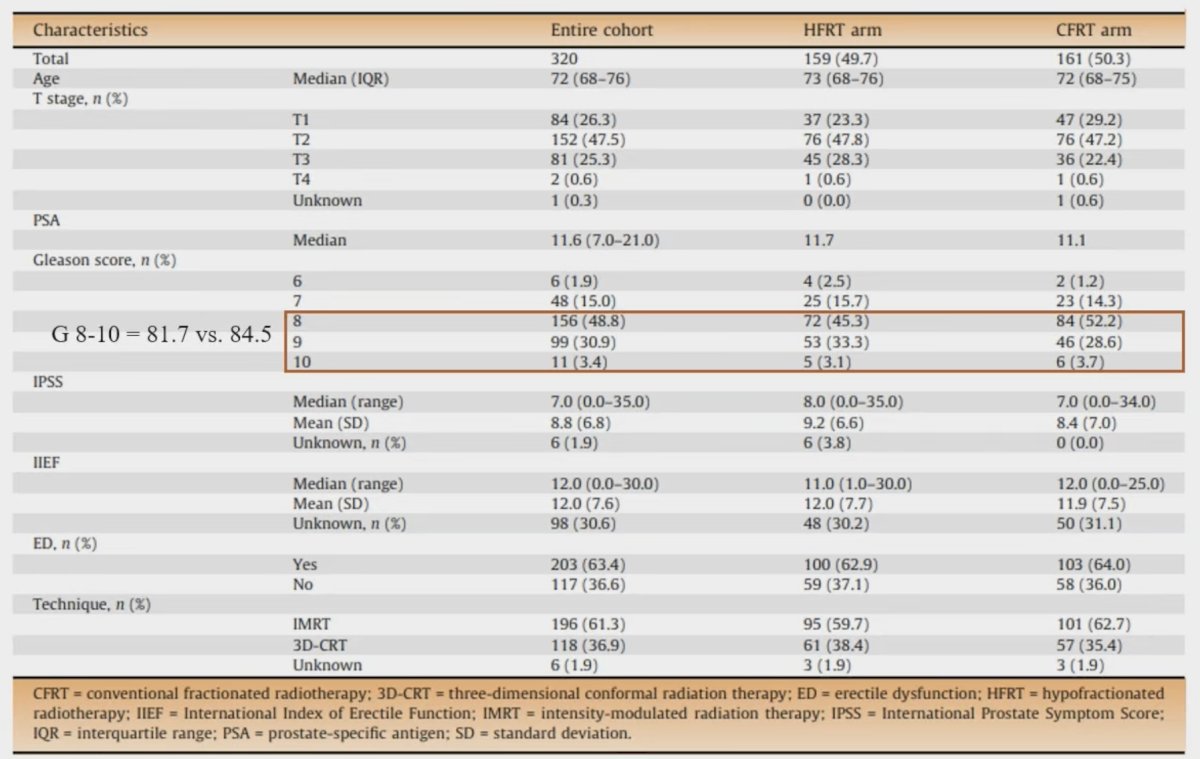
Patients in the hypofractionated arm had higher odds of acute Grade ≥1 (OR: 1.76, p=0.016) and Grade ≥2 (OR: 1.92, p=0.031) GI adverse events. There were no differences in the odds of acute GU events.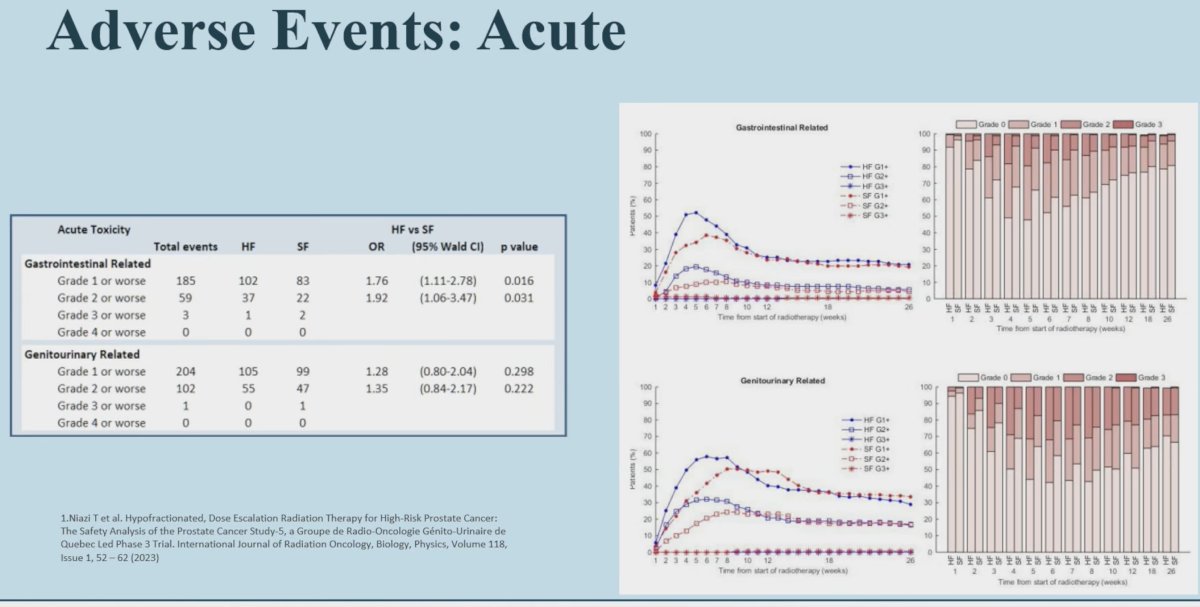
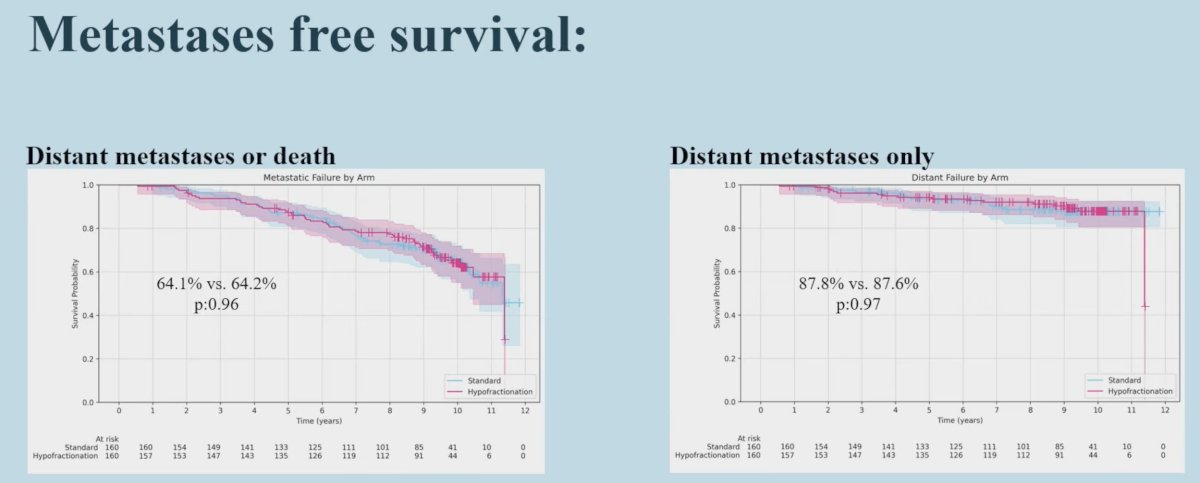
Late Grade ≥2 GU-related adverse events were more common in the standard fractionation arm (OR: 0.25, p=0.035). There were no differences in the odds of late GI-related adverse events.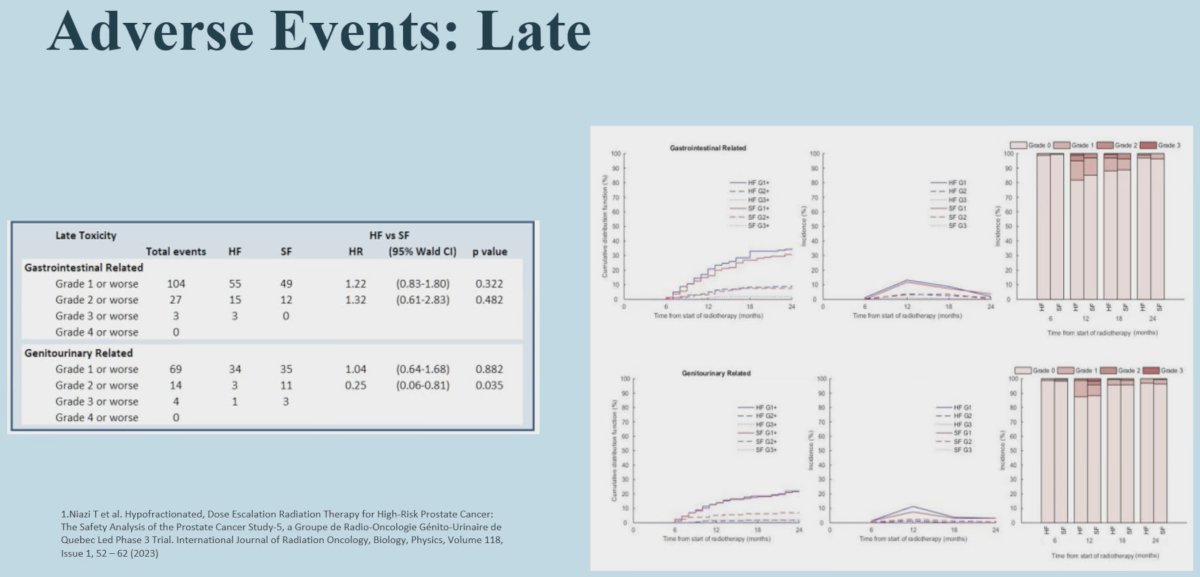 From a survival standpoint (10-year outcomes), no significant differences were observed in biochemical failure-free, metastases-free, prostate cancer-specific, and overall survivals between the two groups:
From a survival standpoint (10-year outcomes), no significant differences were observed in biochemical failure-free, metastases-free, prostate cancer-specific, and overall survivals between the two groups: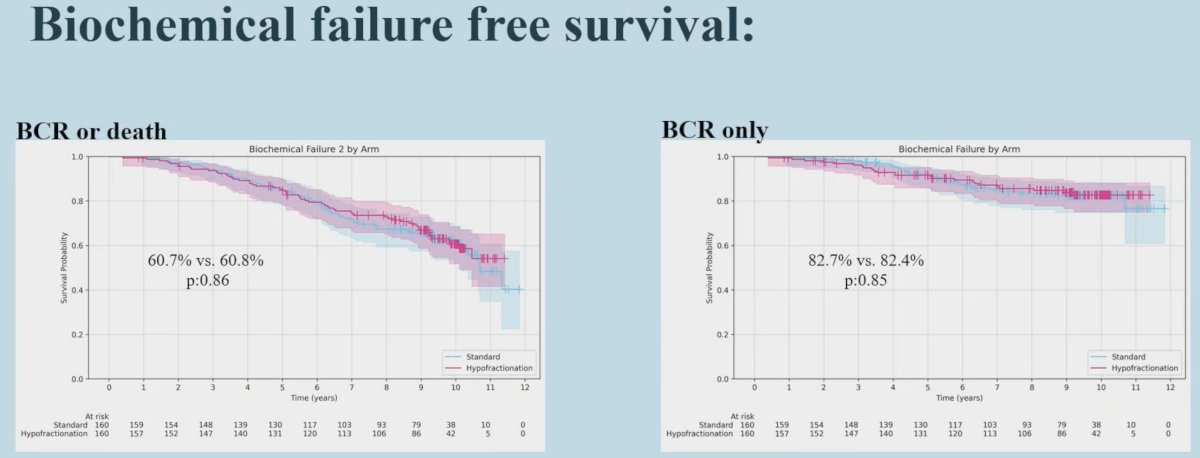
Dr. Niazi summarized the 10-year survival outcomes as follows:
- At 10 years follow-up, there were no significant differences in survival outcomes between hypo- and conventionally fractionated radiotherapy arms:
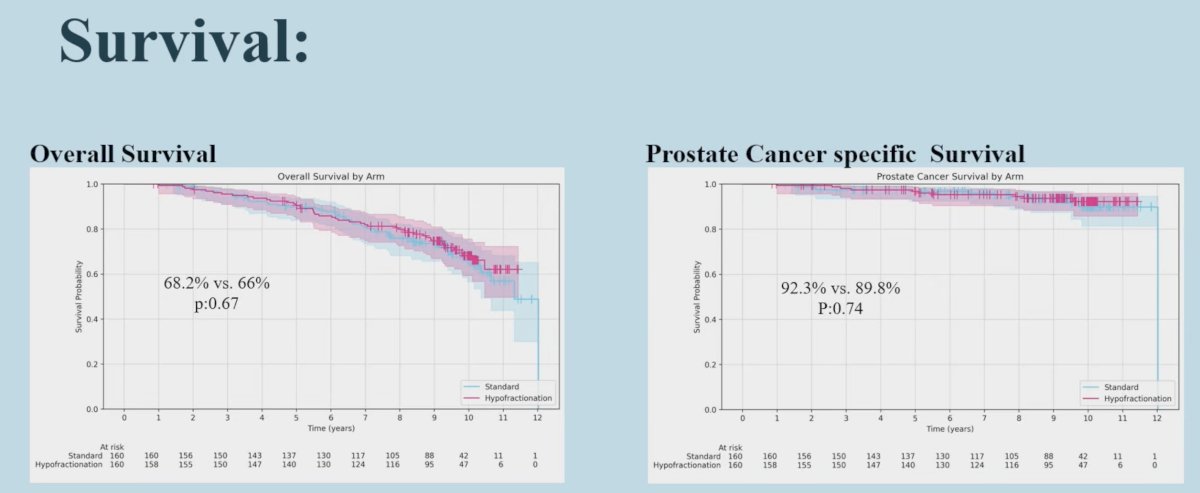
- Overall survival: 68% vs. 66% (HR: 1.04, p=0.67)
- Prostate cancer-specific survival: 92.3% vs. 90% (HR: 1.03, p=0.74)
- Biochemical failure-free survival: 60.7% vs. 60.8% (HR: 1.01, p=0.86)
- Metastasis-free survival: 64.1% vs. 64.2% (HR: 1.01, p=0.96)
- Hazard ratios for all outcomes: close to 1.00 at 3-, 5-, 7-, and 10 years after treatment.
Dr. Niazi concluded as follows:
- PCS5 is the 1st randomized study to evaluate moderate hypofractionated radiotherapy in high-risk prostate cancer patients treated with contemporary radiation plus androgen suppression
- These 10-year results confirm that hypofractionated radiotherapy (68 Gy in 25 fractions) is non-inferior to conventionally fractionated radiotherapy (76 Gy in 38 fractions) for high-risk prostate cancer patients treated with pelvic radiotherapy and long-term ADT
- Moderate hypofractionation should be considered as a standard of care option for high-risk prostate cancer patients planned for external beam radiotherapy plus long-term ADT.
Presented by: Tamim Niazi, MD, Associate Professor, Department of Oncology, Division of Radiation Oncology, McGill University, Montreal, QC
Written by: Rashid K. Sayyid, MD, MSc, Urologic Oncologist, Department of Urology, The University of Arizona, @rksayyid on X during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025
Related content: Ten-Year Outcomes of the PCS5 Trial for High-Risk Prostate Cancer Presented - Tamim Niazi
Reference:
- Niazi T, Nabid A, Malagon T, et al. Hypofractionated Dose Escalation Radiotherapy for High-Risk Prostate Cancer: the survival analysis of the Prostate Cancer Study-5 (PCS-5), a GROUQ-led phase III trial. Eur Urol. 2025; 87(3): 314-323.