(UroToday.com The 2025 ASTRO annual meeting featured a prostate cancer session and a presentation by Dr. Beth Neilsen discussing genomic and transcriptomic profiling of radiation-resistant, locally recurrent prostate cancer. Very little is known about the biological underpinnings of intraprostatic recurrences after definitive radiotherapy for prostate cancer. Understanding the etiology of radiation resistance in prostate cancer could lead to improved prognostic and predictive biomarkers and may have implications for the management of both recurrent and newly diagnosed prostate cancer. Dr. Neilsen and investigators hypothesized that there are conserved molecular profiles associated with local radioresistance.
Forty-one locally radiorecurrent prostate cancer tumors from 36 unique patients treated at two large academic centers were profiled using a targeted pan-cancer DNA sequencing panel as well as RNA expression (Veracyte). Genomic alteration frequencies within locally radiorecurrent prostate cancer were compared to alteration frequencies in treatment naïve prostate cancer from The Cancer Genome Atlas (TCGA). Transcriptomic data were compared to de-identified data from the Decipher Genomics Resource Information Database (GRID; NCT02609269, n = 146,865), which was accessed to create a subset (n = 22,320) of patients identified by matching Gleason grade group at the time of initial diagnosis with the locally radiorecurrent cohort. Standardized mean differences (SMDs) were used to assess for small (<0.4), moderate (0.4-0.7), and large (>0.7) differences between the cohorts.
The locally radiorecurrent cohort included patients with relatively aggressive disease, including 39% with Gleason grade 5, 25% with Gleason grade 4, and 17% Gleason grade 3: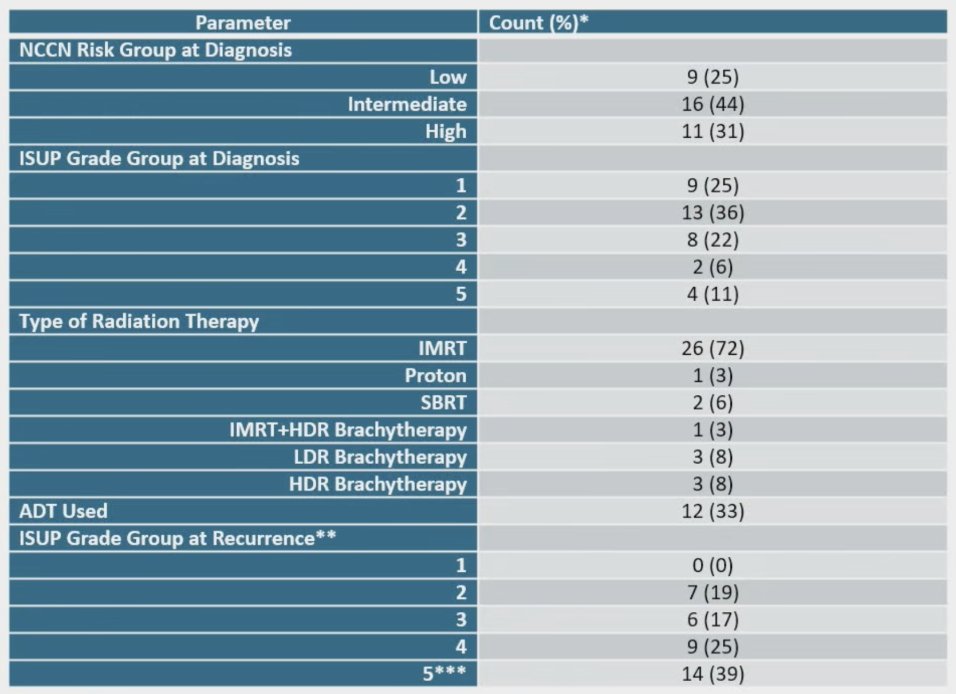
The locally radiorecurrent prostate cancer cohort demonstrated enrichment in PI3K pathway alterations compared to treatment naïve prostate cancer within TCGA, with alteration frequencies in PTEN of 12% (5/41) versus 3%, [p = 0.005] and PIK3CA of 12% (5/41) versus 2% [p < 0.001]. Other genetic alterations enriched in locally radiorecurrent prostate cancer include BRCA1 of 10% (4/41), PTCH1 of 22% (9/41), MSH3 of 12% (5/41), and STAG2 of 34% (14/41). However, no common genetic alteration was conserved across all samples:
![The locally radiorecurrent prostate cancer cohort demonstrated enrichment in PI3K pathway alterations compared to treatment naïve prostate cancer within TCGA with alteration frequencies in PTEN of 12% (5/41) versus 3%, [p = 0.005] and PIK3CA of 12% (5/41) versus 2% [p < 0.001]. Other genetic alterations enriched in locally radiorecurrent prostate cancer include BRCA1 of 10% (4/41), PTCH1 of 22% (9/41), MSH3 of 12% (5/41), and STAG2 of 34% (14/41). However, no common genetic alteration was conserved across all samples:](/images/com-doc-importer/229-astro-2025/astro-2025-genomic-and-transcriptomic-profiling-of-radiation-resistant-locally-recurrent-prostate-cancer/image-1.jpg)
![The locally radiorecurrent prostate cancer cohort demonstrated enrichment in PI3K pathway alterations compared to treatment naïve prostate cancer within TCGA with alteration frequencies in PTEN of 12% (5/41) versus 3%, [p = 0.005] and PIK3CA of 12% (5/41) versus 2% [p < 0.001]. Other genetic alterations enriched in locally radiorecurrent prostate cancer include BRCA1 of 10% (4/41), PTCH1 of 22% (9/41), MSH3 of 12% (5/41), and STAG2 of 34% (14/41). However, no common genetic alteration was conserved across all samples: 2](/images/com-doc-importer/229-astro-2025/astro-2025-genomic-and-transcriptomic-profiling-of-radiation-resistant-locally-recurrent-prostate-cancer/image-2.jpg)
The locally radiorecurrent cohort had proportionately greater patients with Decipher high or very high risk signatures (71% locally radiorecurrent versus 56% for Gleason grade-matched GRID [SMD 0.47] and versus 34% for the overall GRID cohort [SMD 1.0]). The locally radiorecurrent cohort demonstrated significantly higher basal phenotype (compared to luminal) based on multiple previously validated scores, including PAM50 [SMD 0.89] and PSC [SMD 0.76]. Lower androgen receptor activity was enriched in locally radiorecurrent (61% for locally radiorecurrent versus 9% for Gleason grade-matched GRID cohort [SMD 1.29]):
![The locally radiorecurrent cohort had proportionately greater patients with Decipher high or very high risk signatures (71% locally radiorecurrent versus 56% for Gleason grade-matched GRID [SMD 0.47] and versus 34% for the overall GRID cohort [SMD 1.0]). The locally radiorecurrent cohort demonstrated significantly higher basal phenotype (compared to luminal) based on multiple previously validated scores including PAM50 [SMD 0.89] and PSC [SMD 0.76]. Lower androgen receptor activity was enriched in locally radiorecurrent (61% for locally radiorecurrent versus 9% for Gleason grade-matched GRID cohort [SMD 1.29]):](/images/com-doc-importer/229-astro-2025/astro-2025-genomic-and-transcriptomic-profiling-of-radiation-resistant-locally-recurrent-prostate-cancer/image-3.jpg)
Dr. Neilsen concluded her presentation discussing genomic and transcriptomic profiling of radiation-resistant, locally recurrent prostate cancer with the following take-home points:
- A majority of patients had pathological upgrading at recurrence
- Genetic alterations in genes associated with increased prostate cancer aggressiveness and DNA repair were frequent in locally recurrent prostate cancer
- Locally radiorecurrent prostate cancer was more likely to have higher Decipher scores
- Locally radiorecurrent prostate cancer demonstrated basal subtype signatures (PAM50) and lower androgen receptor activity on transcriptomic profiling
- Future directions include:
- Further characterizing common molecular mechanisms and conserved pathways involved in locally radiorecurrent prostate cancer
- Validation of these results in other cohorts and with basic science approaches
- Ongoing efforts to obtain paired pre-radiotherapy and recurrent prostate cancer samples for comprehensive profiling
These results are being published as a brief report in the International Journal of Radiation Oncology, Biology, and Physics.
Presented by: Beth Neilsen, MD, PhD, Stanford Cancer Center South Bay, San Jose, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.