(UroToday.com) The 2025 ASTRO annual meeting featured a clinical trials session and a presentation by Dr. Amar Kishan discussing the primary endpoint analysis of the phase II LUNAR randomized trial assessing neoadjuvant 177Lu-PSMA prior to ablative radiotherapy for oligorecurrent prostate cancer. Metastasis-directed stereotactic body radiotherapy in recurrent oligometastatic hormone-sensitive prostate cancer has emerged to improve progression-free survival. Moreover, highly sensitive PSMA PET/CT imaging has allowed optimal identification of patients for metastasis-directed stereotactic body radiotherapy.
Unfortunately, progression ultimately still occurs in a majority of patients, underscoring the existence of occult microscopic disease. PSMA-based radioligand therapy agents that combine 177Lu with ligands to PSMA have offered improved progression-free survival in men with advanced prostate cancer. These drugs were first studied in late-stage, post-chemotherapy metastatic castration resistant disease, and now have promising data, even in de novo metastatic hormone-sensitive disease. Thus far, the observed impact of PSMA-based radioligand therapy has been primarily in patients with macroscopic disease. Dr. Kishan and investigators hypothesized that adding PSMA-targeting radioligand therapy to metastasis-directed stereotactic body radiotherapy will improve progression-free survival in patients with oligometastatic hormone-sensitive prostate cancer by acting on occult, microscopic disease.
Patients with recurrent oligometastatic hormone sensitive prostate cancer, characterized by 1-5 lesions outside the prostate or prostate bed on PSMA PET/CT, were randomized in a 1:1 fashion to receive either stereotactic body radiotherapy to all metastatic lesions versus 2 cycles of neoadjuvant 177Lu-PSMA PNT2002 (6.8 GBq/cycles) 6-8 weeks apart followed by stereotactic body radiotherapy to all metastatic lesions. Stratification was based on the number of lesions (1 versus 2-3 versus 4-5) and PSMA-based stage (N1/M1a versus M1b versus M1c):
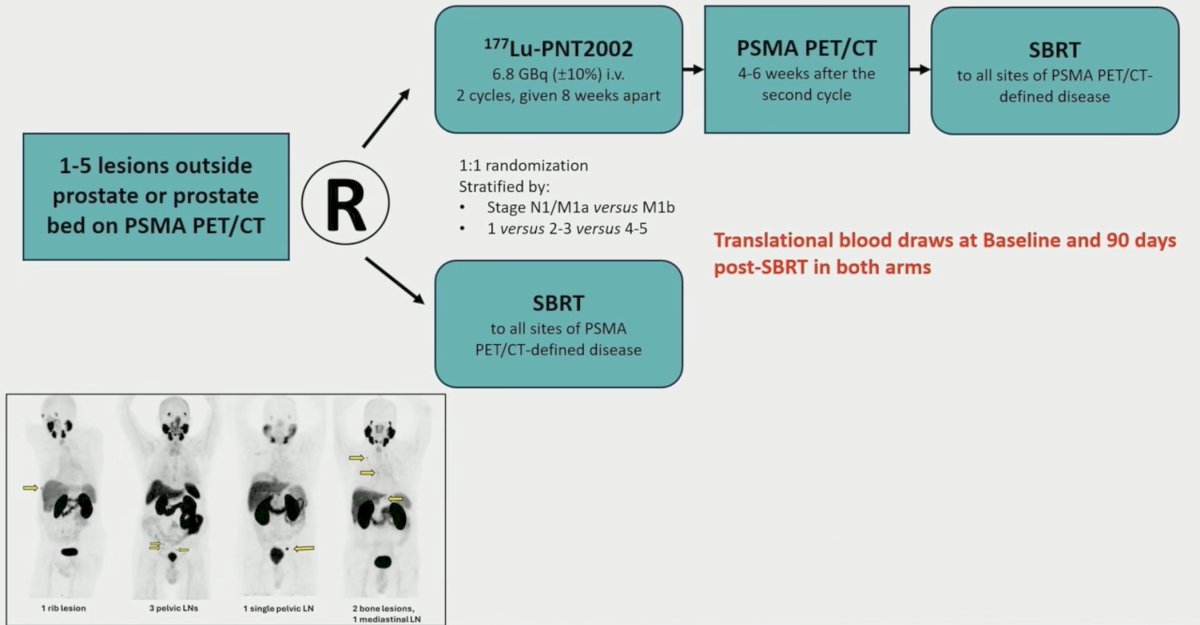
The primary endpoint was progression-free survival, with progression defined as PSMA-avid lesions seen at the time of biochemical progression or on a scheduled PSMA PET/CT performed 12 months after stereotactic body radiotherapy completion, initiation of salvage therapy, or death. This was a randomized phase II design with a one-sided alpha of 0.1 and a power of 0.80, yielding a target accrual of 90 patients. Progression-free survival was compared using a one-sided log-rank test based on Kaplan-Meier estimates. Exploratory analyses focused on associations between immunologic parameters and germline variants with progression-free survival.
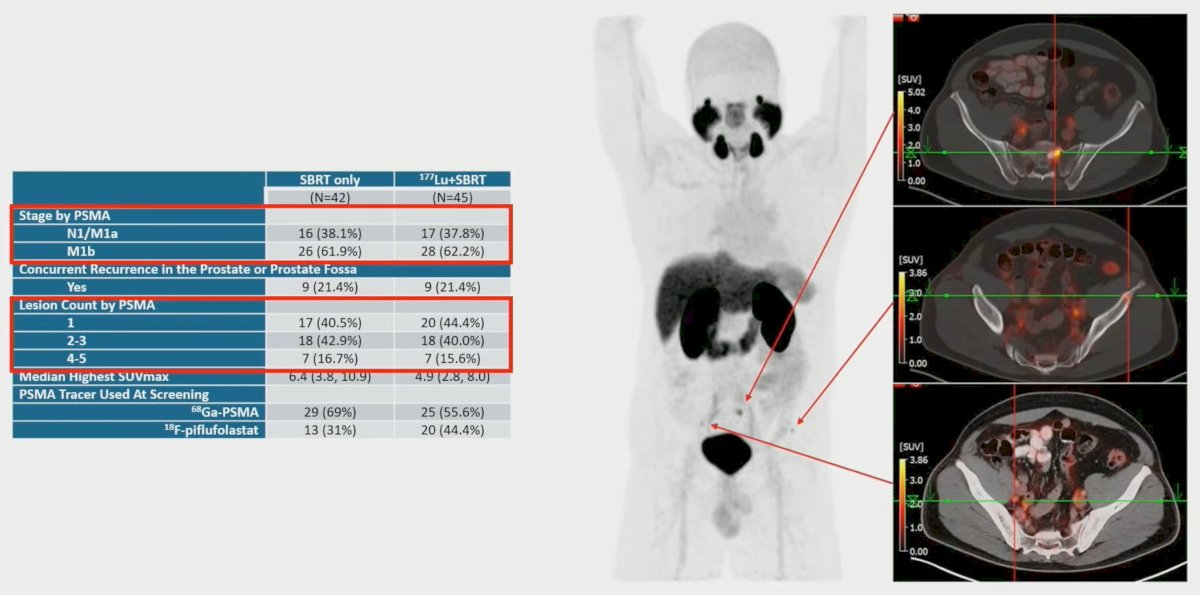
From September 2, 2022, to November 9, 2023, 92 patients were randomized (n = 47 stereotactic body radiotherapy alone, n = 45 177Lu-PSMA + stereotactic body radiotherapy); 5 patients randomized to stereotactic body radiotherapy alone dropped out prior to therapy. The median age was 69 years, and the median PSA was 1.1 ng/dL, with 38% of patients having M1b disease, and 43% of patients having solitary lesions: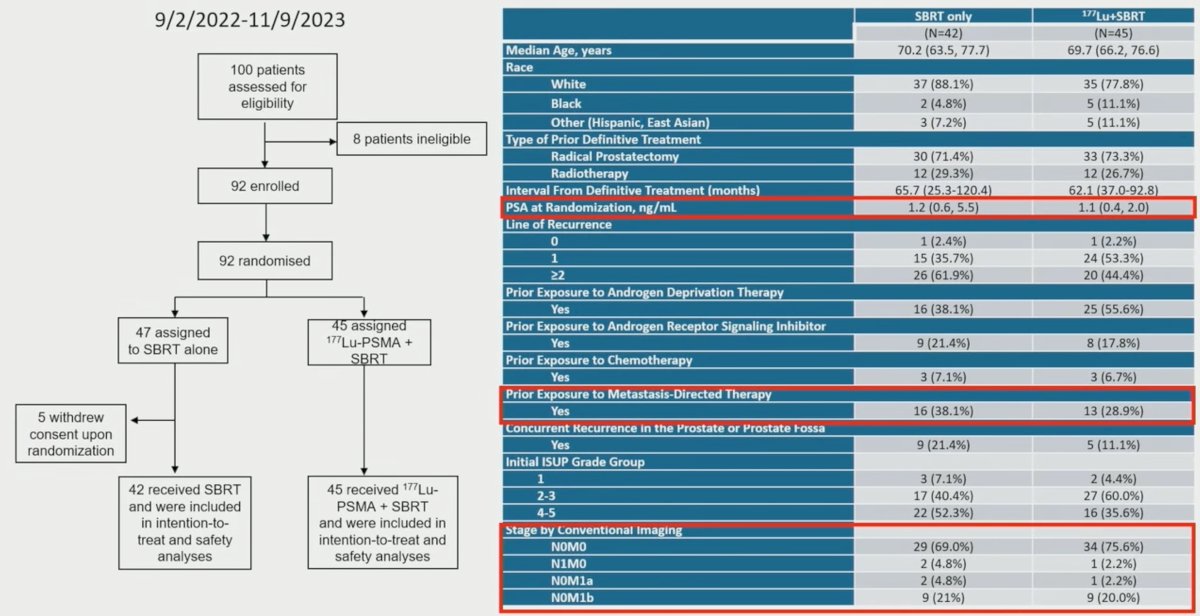
At a median follow-up of 20 months, the addition of 177Lu-PSMA to stereotactic body radiotherapy significantly improved median progression-free survival from 7.4 months (95% CI 6.0-13.5 months) to 17.6 months (95% CI 15 months – not reached; HR 0.37, 95% CI 0.22-61):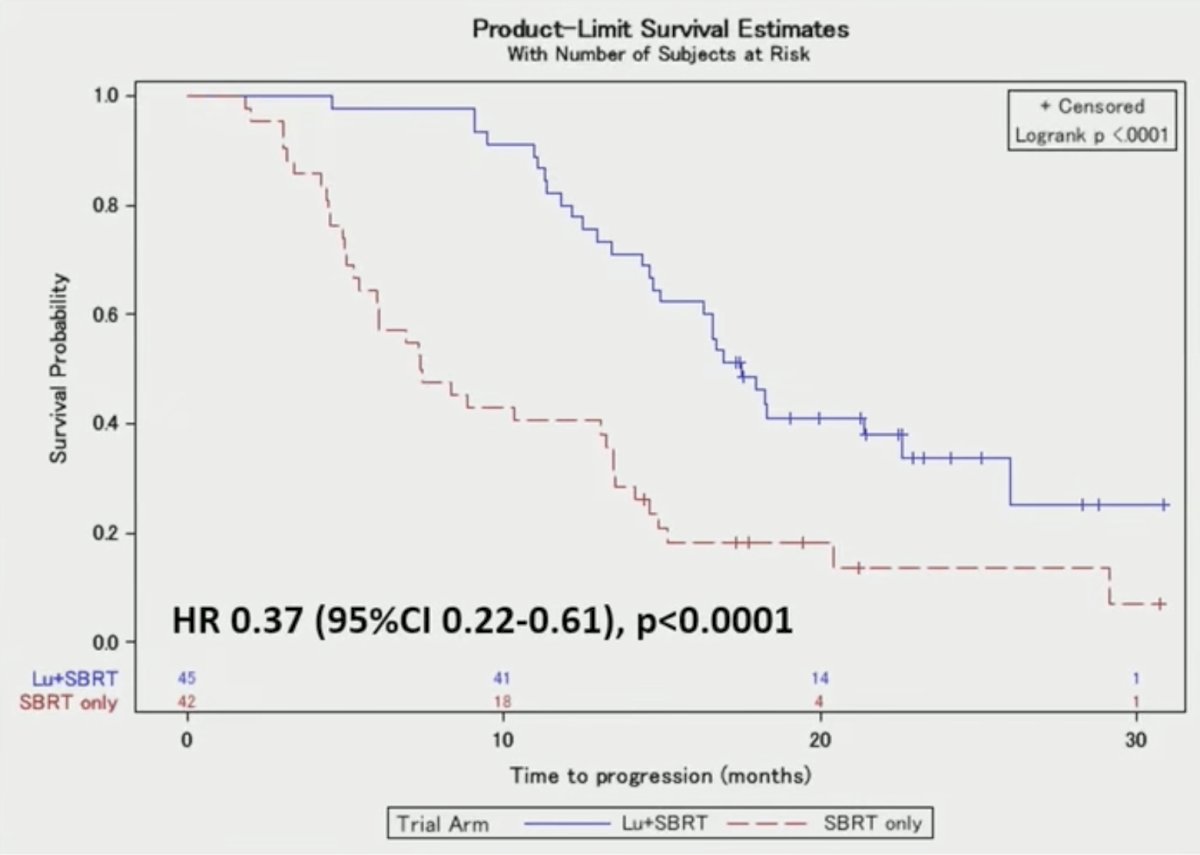
Of note, 64/65 progression events (98%) corresponded to new lesions, and on a per-lesion basis, 2/91 lesions (2%) on the stereotactic body radiotherapy arm and 0/96 (0%) on the 177Lu-PSMA + stereotactic body radiotherapy arm showed in-field progression. Median hormone therapy-free survival increased from 14.1 months (95% CI 10.1 months – not reached) to 24.3 months (95% CI 18 months – not reached; HR 0.40, 95% CI 0.22-0.71):

Of note, 46/47 patients (98%) who received salvage hormone therapy had new lesions on PSMA PET/CT. Repeat metastasis-directed therapy without hormone therapy was delivered in 17/64 (27%) patients with new lesions.
Grade 3 lymphopenia was seen in 7% and 5% of patients receiving 177Lu-PSMA + stereotactic body radiotherapy and stereotactic body radiotherapy, respectively, with no other grade 3 toxicities attributable to treatment: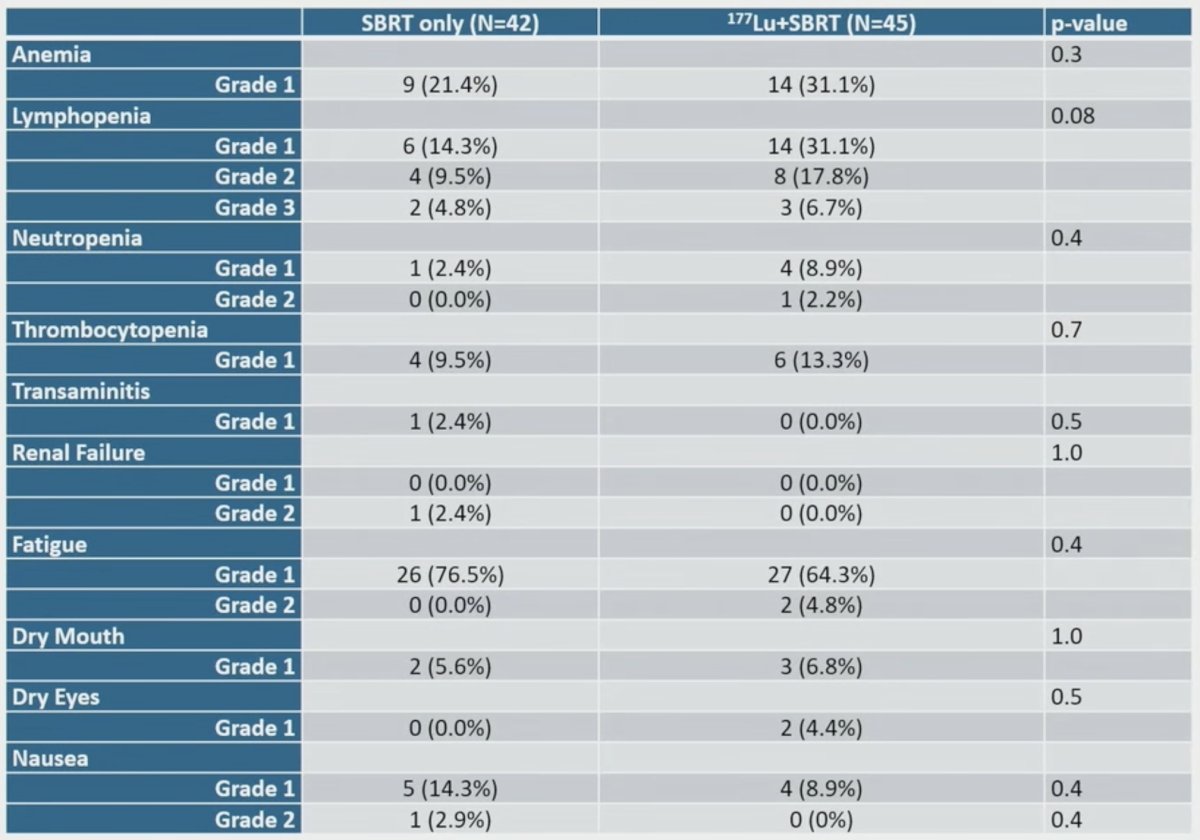
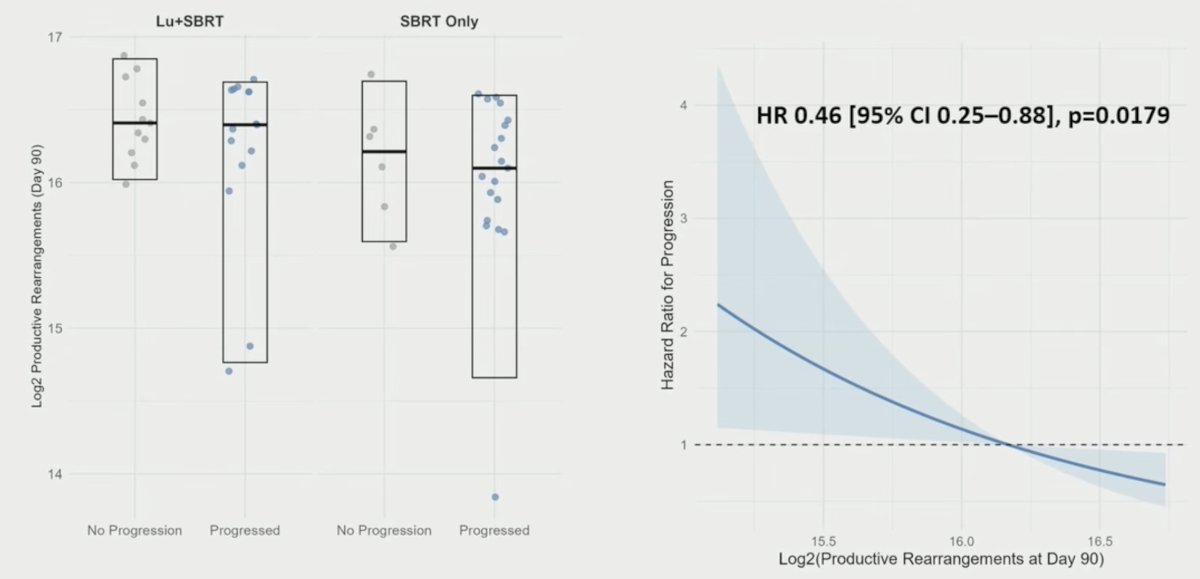
There was a significant between-arm differences in productive T-cell receptor rearrangements at 90 days (p = 0.02) and a significant association between productive rearrangements at 90 days and progression (HR 0.46, 95% CI 0.25-0.88):
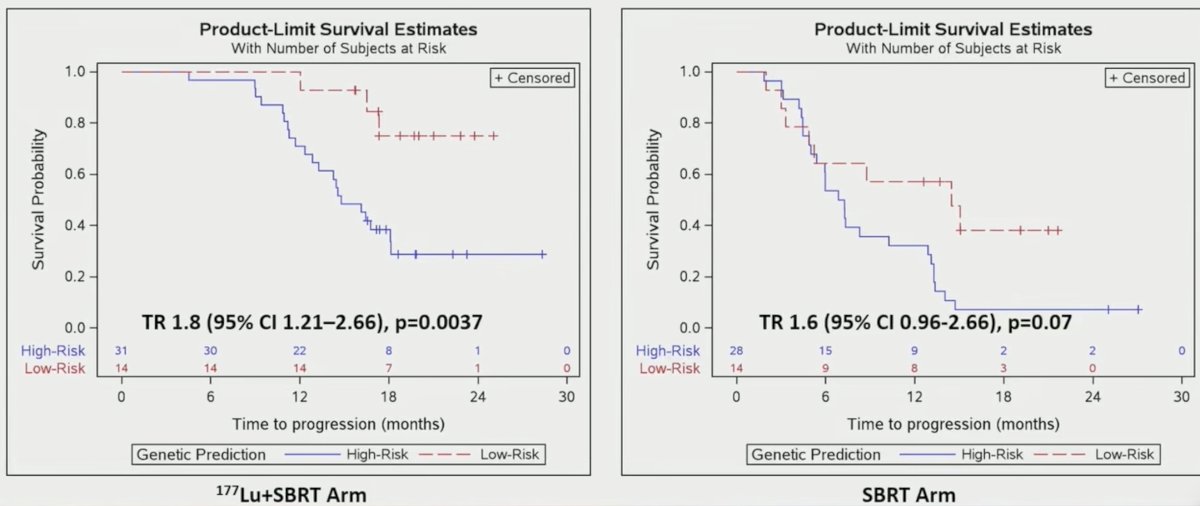
Predictive models based on germline SNPs in 22 genes predicted progression in both arms, but were only statistically significant in the experimental arm:
Dr. Kishan concluded his presentation discussing the primary endpoint analysis of the phase II LUNAR randomized trial with the following take-home points:
- Adding two cycles of 177Lu-PSMA PNT2002 to stereotactic body radiotherapy significantly improved progression-free survival in men with oligorecurrent prostate cancer, presumably by action against occult metastatic disease, without attendant increase in toxicity
- Progression-free survival was defined based on PSMA PET/CT-based progression, which may not carry prognostic impact of progression on conventional imaging, but is a highly pragmatic endpoint
- Increased T-cell receptor productive rearrangements at 90 days were prognostic, and a biomarker based on germline variants in genes largely related to immune response and DNA repair was identified
- 64% of patients on the 177Lu-PSMA PNT2002 + stereotactic body radiotherapy arm still progressed, suggesting that further optimization is possible
Presented by: Amar U. Kishan, MD, Professor, Executive Vice Chair of Clinical and Translational Research, Department of Radiation Oncology, University of California, Los Angeles (UCLA), Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.