(UroToday.com) The 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting held in San Francisco, CA, was host to an advances in localized prostate cancer session. Dr. Abhishek Kumar presented the results of a study evaluating the outcomes following radiation therapy and radical prostatectomy in patients with high-risk prostate cancer within the context of a similar access system.
Dr. Kumar noted that high-risk prostate cancer remains a heterogeneous disease and is associated with a high risk of metastasis. The NCCN Guidelines currently recommend radiation therapy plus long-term androgen deprivation therapy as a category 1 treatment option and radical prostatectomy with lymphadenectomy and personalized use of postoperative therapy as a category 2A option. To date, no randomized data have compared these treatment strategies in high-risk prostate cancer.
The objective of this study was to compare oncologic outcomes among patients undergoing a radiotherapy versus radical prostatectomy-based approach in a ‘modern’ US cohort using the United States Department of Veterans Affairs Corporate Data Warehouse dataset. Patients with localized, high-risk prostate cancer were included, defined as having ≥1 of the following:
- PSA > 20 ng/mL
- Clinical stage cT3-T4 or presence of MRI-detected extraprostatic extension
- Gleason score 8-10
All patients had a pre-treatment MRI prostate study report available for review. The clinical notes were reviewed to assess if radiotherapy patients were surgical candidates and vice versa.
The primary outcome was the cumulative incidence of distant metastases modeled using Fine-Gray regression modeling, with death treated as the competing event. The secondary outcome was overall survival, evaluated using a Cox proportional hazards regression model with outcomes reported using hazard ratios (HRs) and 95% confidence intervals (95% CI).
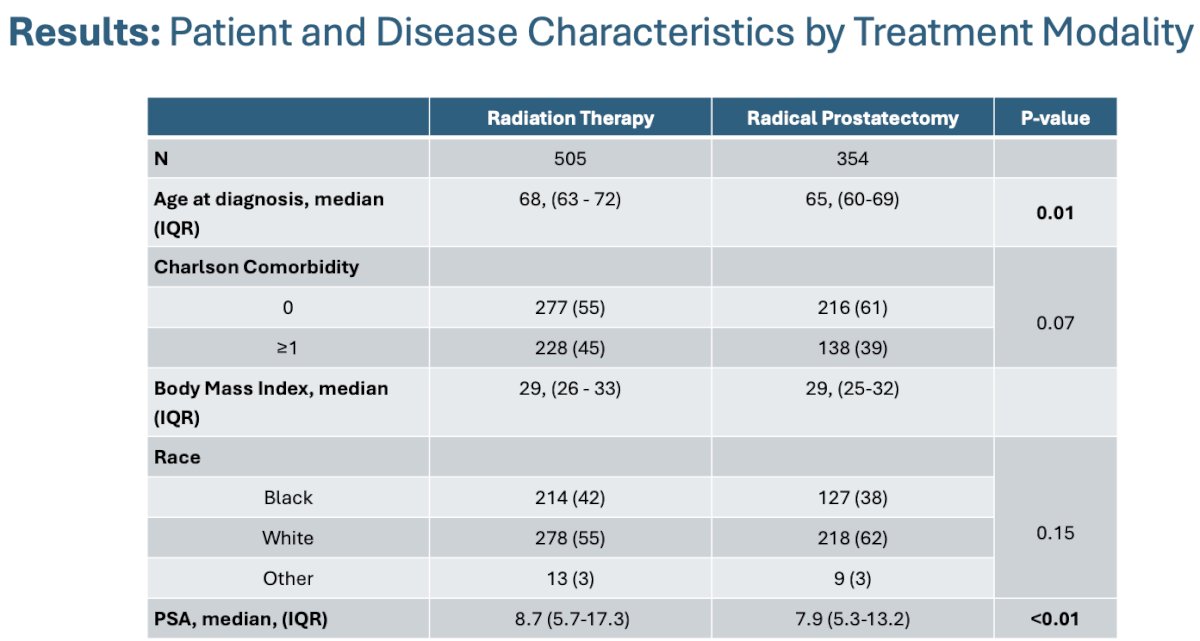
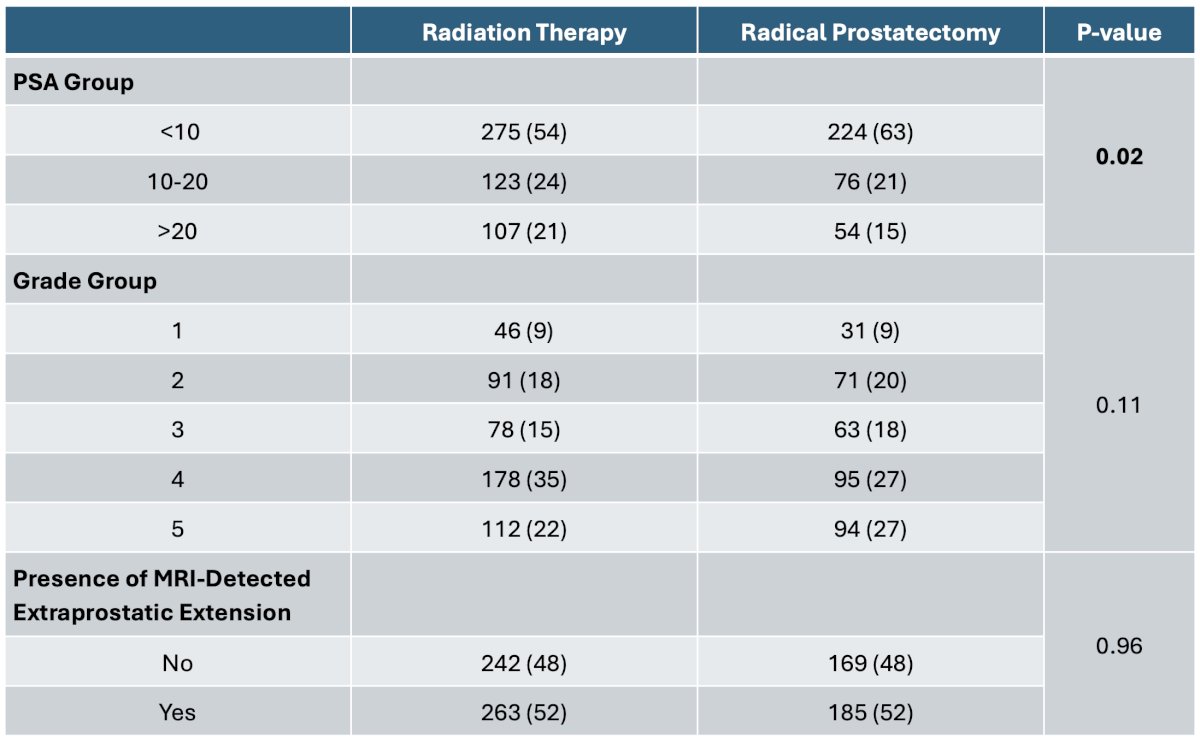
The study cohort included 859 patients (radiation therapy: 505; radical prostatectomy: 354). Radiation therapy-treated patients were older (68 vs 65 years, p<0.01) and had a significantly higher serum PSA level (8.7 vs 7.9 ng/ml; p<0.01), with 46% having a serum PSA level >10 ng/ml (RP: 37%, p=0.02). There were no significant differences in Grade Group patterns or presence/absence of extraprostatic extension on MRI.
58% of patients in the radiation therapy arm received concurrent ADT for ≥18 months. 77% of radiation therapy patients were considered potential radical prostatectomy candidates.
The median follow-up for the cohort was 4.8 years. The five-year overall survival for the entire cohort was 92%. The 5-year cumulative incidence of metastases in the cohort was 9%. In the radical prostatectomy subgroup, the 5-year cumulative incidence of receiving post-operative radiotherapy was 32%, with an additional 5% declining post-prostatectomy radiotherapy. Of the 110 patients who received post-prostatectomy radiotherapy, 76% received concurrent ADT.
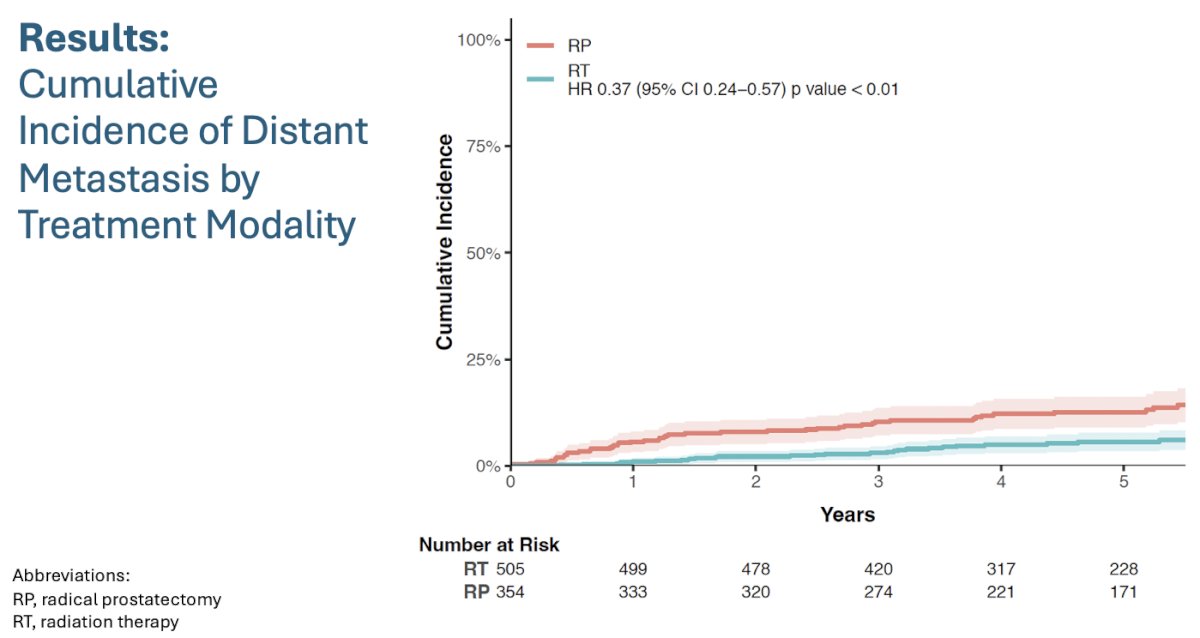
As seen in the cumulative incidence function curves below, patients in the radiotherapy arm had 63% lower rate of distant metastases (HR: 0.37, 95% CI: 0.24–0.57, p<0.01).
When the outcomes were stratified by surgical candidacy (i.e., dividing the radiotherapy group into surgical [SC] and non-surgical candidates [NSC]), the authors found consistent results in favor of radiotherapy, compared to radical prostatectomy (HRs: 0.34-0.45, p<0.025 for both comparisons):

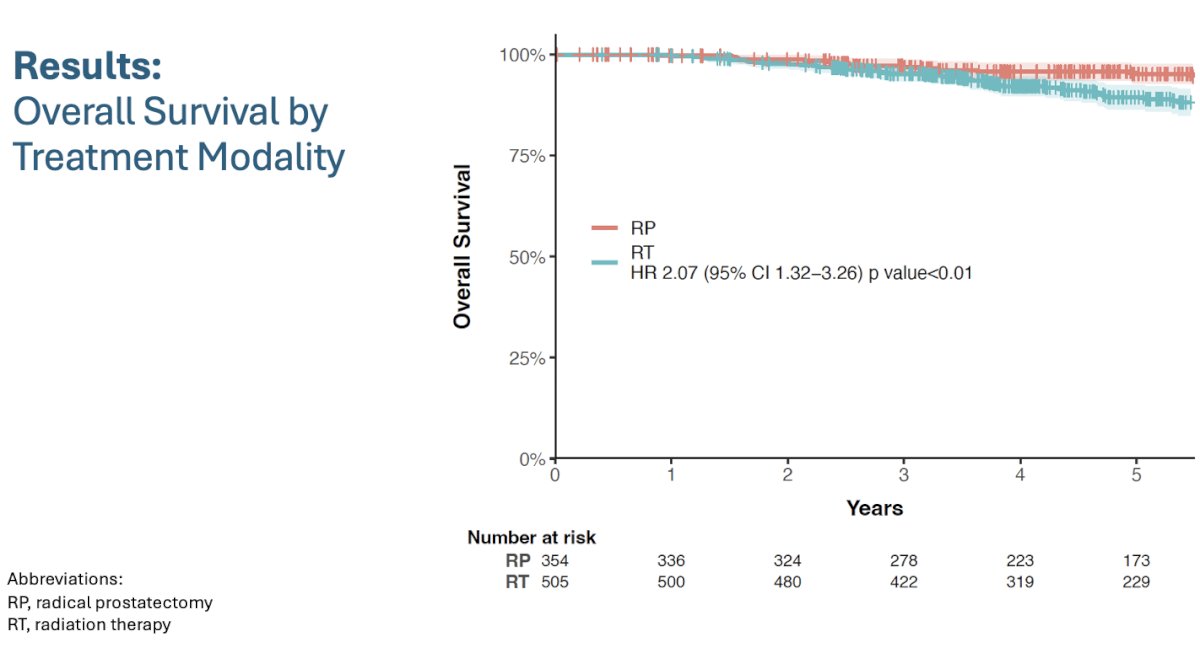
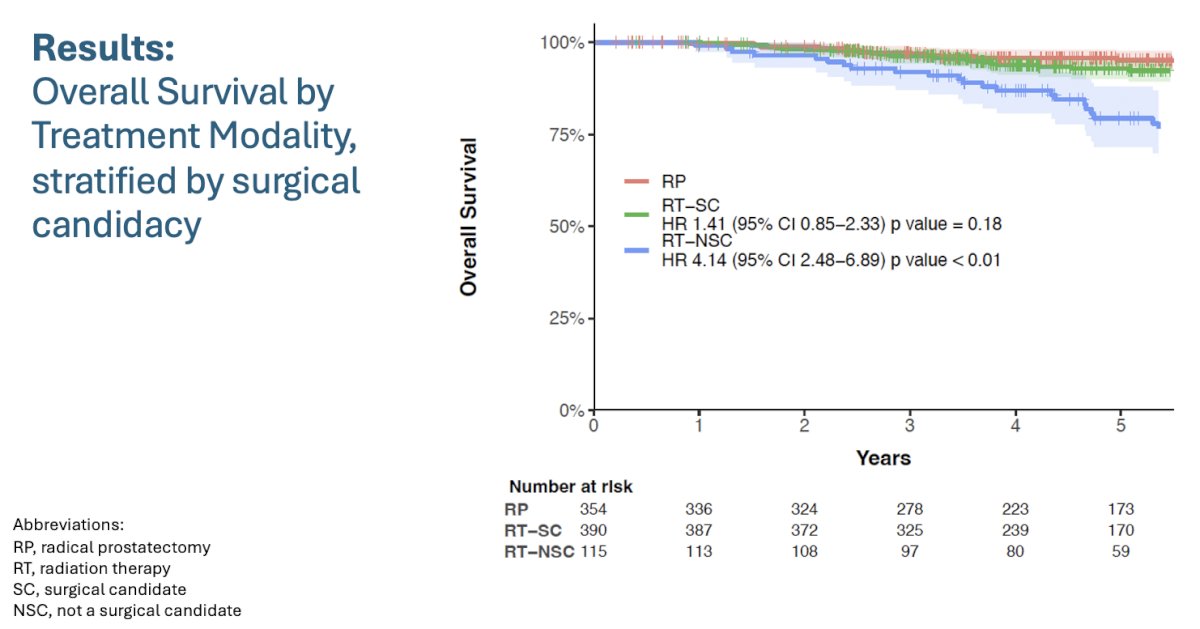
Overall, patients in the radiotherapy arm had worse overall survival outcomes (HR: 2.07, p<0.01):
However, when stratified by surgical candidacy, the authors noted that only NSC radiotherapy patients had worse overall survival outcomes (HR: 4.14, p<0.01), whereas those who were potential surgical candidates (i.e., RT-SC) had non-significantly different overall survival outcomes to radical prostatectomy patients (HR: 1.41, p=0.18).
After multivariable adjustment, patients receiving radiotherapy had lower risk of distant metastases compared to patients receiving radical prostatectomy, irrespective of whether they were surgical candidates (HR: 0.34, 95% CI: 0.21–0.56, p<0.01) or not (HR: 0.38, 95% CI: 0.19–0.75, p<0.01).
Compared to patients receiving radical prostatectomy, patients receiving radiotherapy who were surgical candidates had similar overall survival (HR: 1.04, 95% CI: 0.61–1.77, p=0.88) while those who were not had worse overall survival rates (HR: 2.86, 95% CI: 1.65–4.93, p<0.01).
Dr. Kumar noted that the strengths and limitations of this study include the following:
- Strengths
- Inclusion of MRI prostate findings
- Diverse cohort: 40% of patients were Black
- Approximately 90% treated after 2016
- Could account for surgical candidacy in radiotherapy patients
- Limitations
- Retrospective, no standardized approach to radiation therapy or radical prostatectomy, ADT duration, salvage/adjuvant radiotherapy
- Limited follow-up time (4.8 years)
- Lack of PSMA-PET data
Dr. Kumar concluded as follows:
- In a national, ‘modern’ cohort, patients receiving a radiotherapy-based treatment approach, including ADT, had a nearly three-fold lower rate of distant metastases compared to patients receiving an radical prostatectomy-based approach (abiraterone may further increase relative benefit)
- Nearly 40% of radical prostatectomy patients received or were recommended post-operative radiotherapy, most of whom received ADT
- Overall survival was similar between radical prostatectomy- and radiotherapy-based approaches if patients receiving radiotherapy were also surgical candidates, but worse if not surgical candidates
- SPCG-15 is an open randomized trial comparing radical prostatectomy to radiotherapy in high-risk prostate cancer patient
- In the meantime, there will be additional advancements in imaging, biomarkers (genomic and multimodal AI), and enhanced systemic agents to consider when evaluating treatment options in the high-risk prostate cancer setting
Presented by: Abhishek Kumar, MD, MAS, The Oncology Institute of Hope and Innovation, Cerritos, CA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025