(UroToday.com) The 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting held in San Francisco, CA, was host to an advances in localized prostate cancer session. Dr. Glen Gejerman presented the results of a randomized, placebo-controlled phase III trial of CAN-2409 + Prodrug in combination with standard of care external beam radiotherapy for newly diagnosed localized prostate cancer.
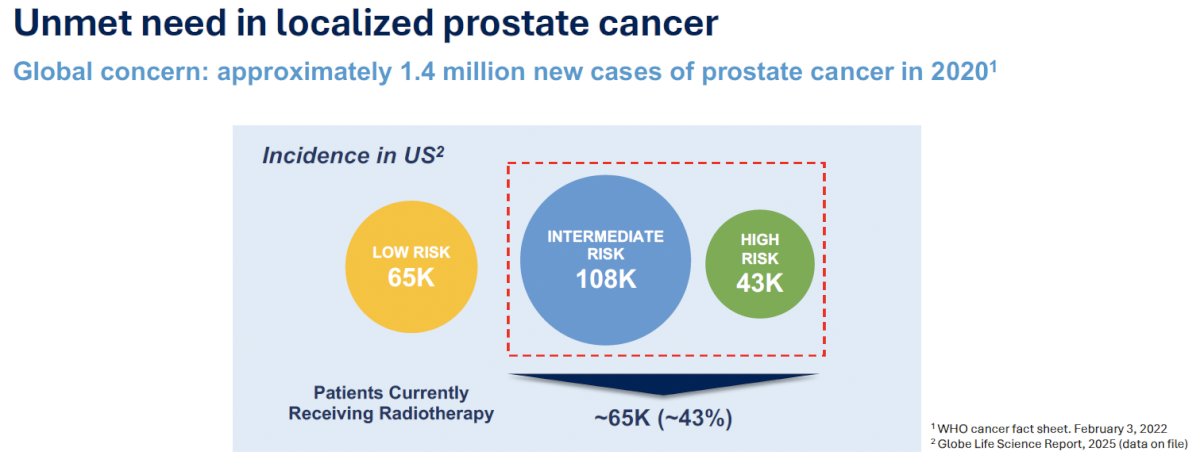
Dr. Gejerman highlighted that there are approximately 1.4 million incident cases of prostate cancer annually worldwide. Of the 216,000 annual cases in the United States, 151,000 are stratified as intermediate- or high-risk, with ~43% (65,000) receiving radiotherapy annually. As such, the treatment burden of prostate cancer becomes evident, and Dr. Gejerman emphasized that the goal of curative treatment is the prevention of cancer recurrence, while minimizing treatment-related side effects and maintaining quality of life.
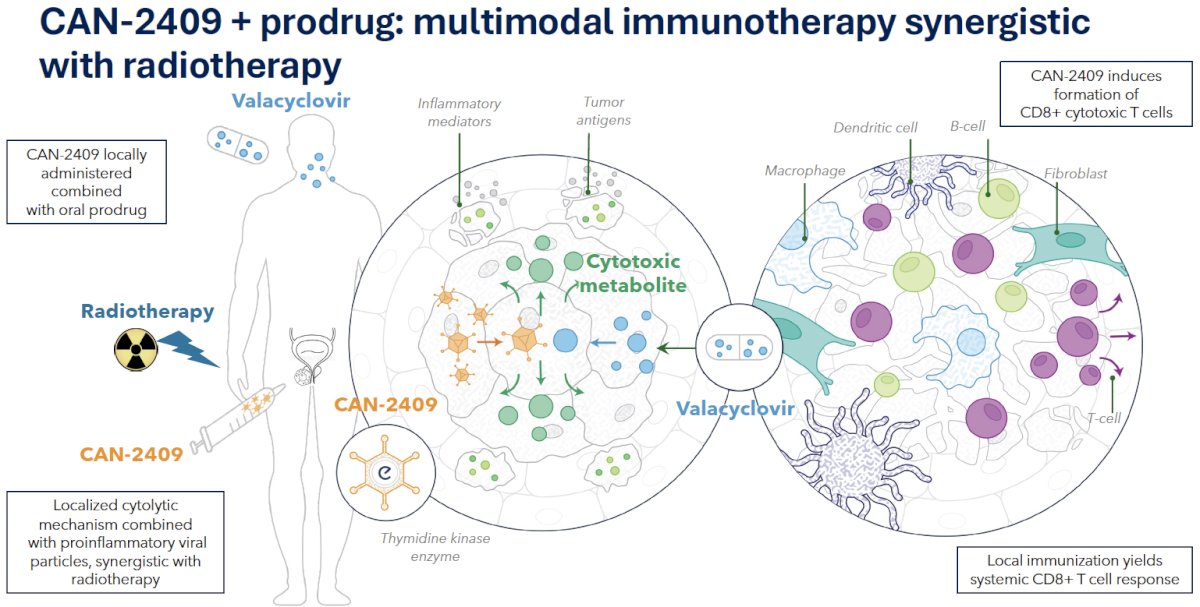
CAN-2409 is an investigational gene therapy for cancer that uses a virus to deliver the herpes simplex virus thymidine kinase (HSV-tk) gene into tumor cells, which then converts an oral prodrug (valacyclovir) into a toxic substance, causing cancer cells to die in an immunogenic way (CD8+ cytotoxic T cells).. This process acts as an in-situ vaccination, triggering a personalized immune response against the tumor and potentiating long-term tumor control. It induces a localized cytolytic mechanism that, combined with pro-inflammatory viral particles, induces a synergistic response with radiotherapy.
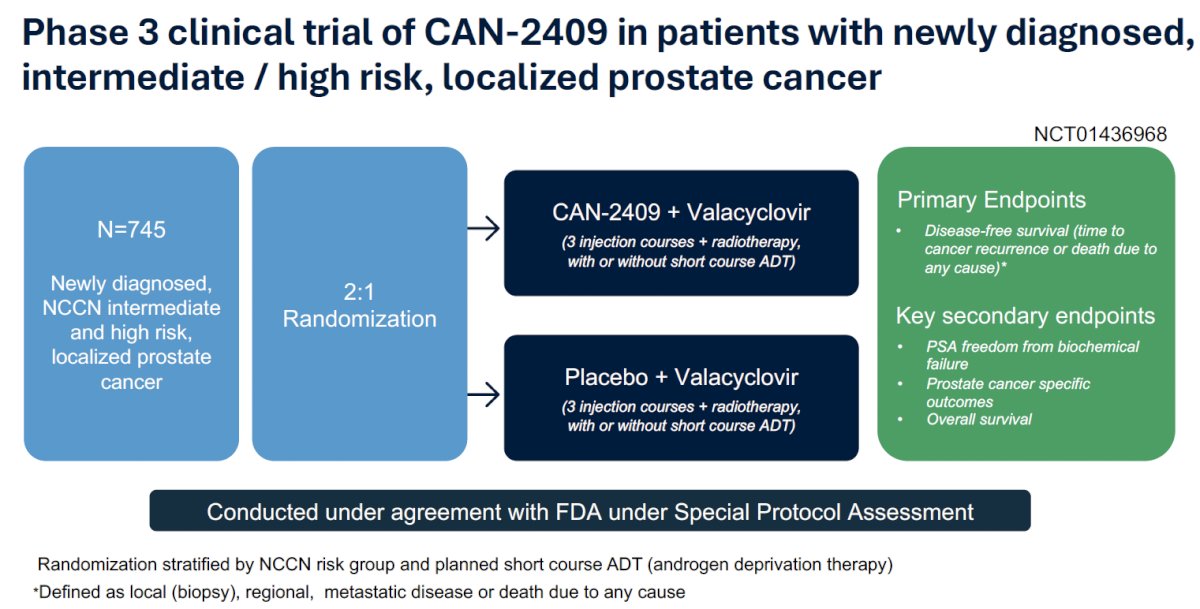
This was a phase III clinical trial of CAN-2409 in patients with newly diagnosed clinically localized, intermediate- or high-risk prostate cancer. A total of 745 eligible participants were randomized 2:1 to:
- CAN-2409 + valacyclovir
- 3 injection courses + radiotherapy +/- short-term ADT
- Placebo + valacyclovir
- 3 injection courses + radiotherapy +/- short-term ADT
The primary study endpoint was disease-free survival. The key secondary endpoints were:
- PSA freedom from biochemical failure
- Prostate cancer-specific outcomes
- Overall survival
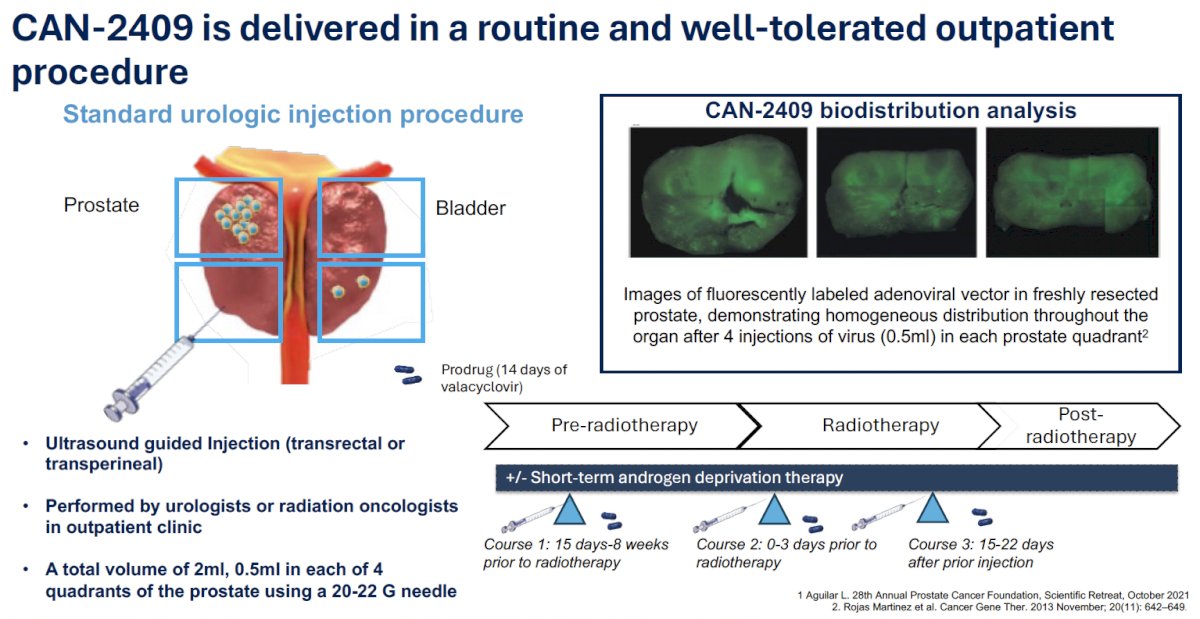
CAN-2409 is delivered via ultrasound-guided injections (transrectal or transperineal) by a urologist or radiation oncologist in an outpatient clinic setting. A total volume of 2 cc is injected (0.5 ml in each of the 4 prostate quadrants using a 20-22 G needle). CAN-2409 is injected in 3 courses:
- Course 1: 15 days to 8 weeks prior to radiotherapy
- Course 2: 0–3 days prior to radiotherapy
- Course 3: 15–22 days after the prior injection
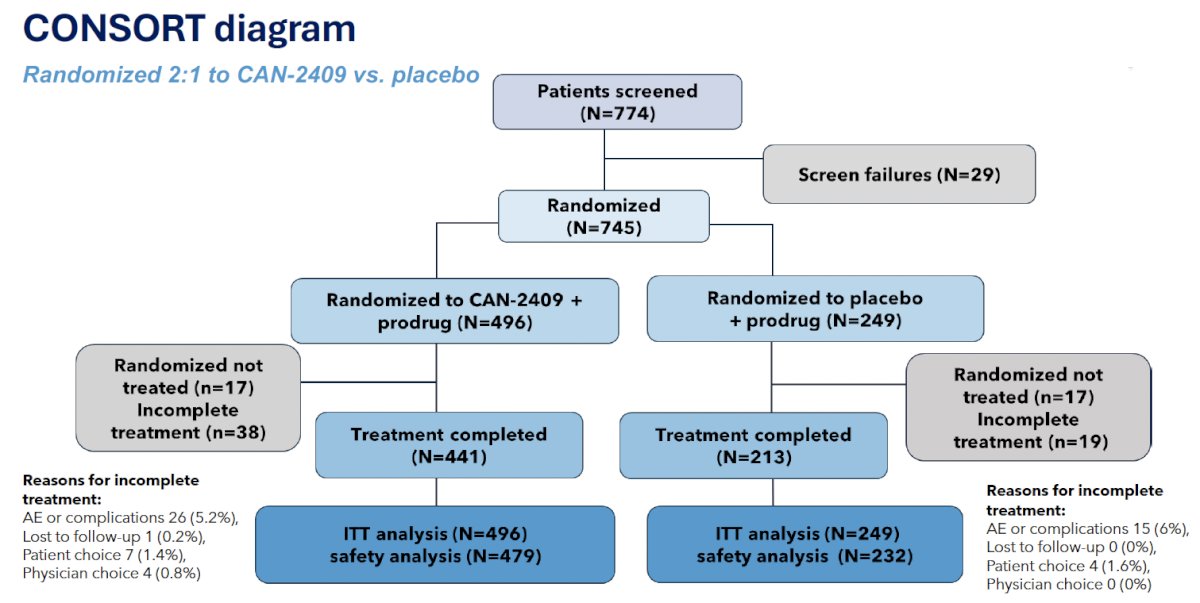
The study CONSORT diagram is illustrated below. 38/496 patients did not complete treatment in the CAN-2409 investigational arm
The baseline patient characteristics are summarized below. The median age was 69 years. 85% of patients had intermediate-risk disease and Gleason 7 disease. The median PSA was 6.7 ng/ml. Nearly 50% of patients were planned for concurrent ADT.

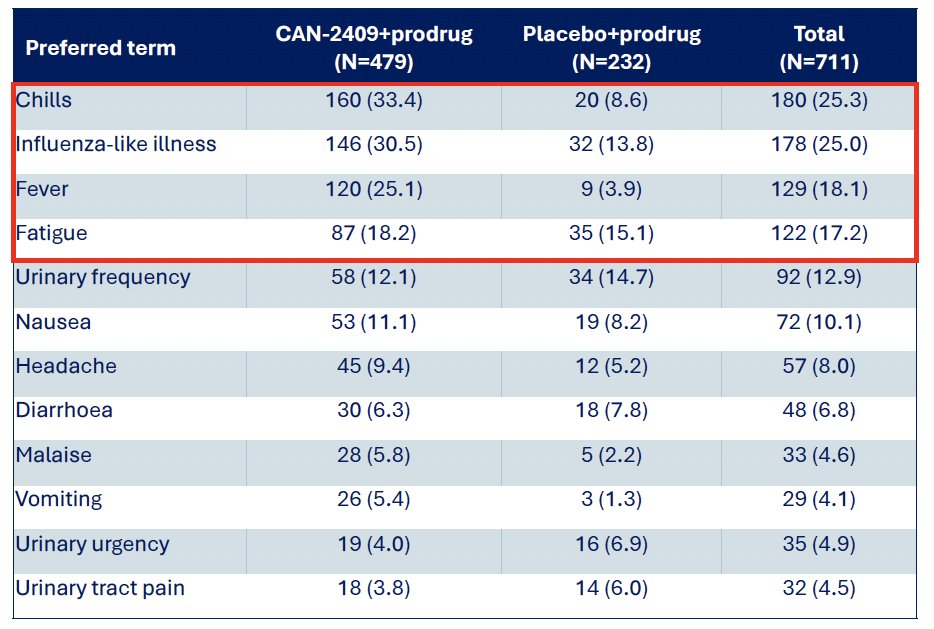
CAN-2409 in combination with standard of care radiotherapy +/- ADT was generally well-tolerated. The most frequent treatment-related adverse events (TRAEs) are summarized in the table below:
- Chills, fever, flu-like symptoms were commonly mild to moderate and self-limited.
- >90% of fever, flu-like symptoms, chills and fatigue resolved within 24–72 hours.
- The incidence of treatment-related serious adverse events (SAEs) was lower in the CAN-2409 arm (1.7% vs 2.2%).
- The overall incidence of SAEs (both treatment and non-treatment related) was lower in the CAN-2409 arm (5.8% vs 7.3%).
- The incidence of treatment discontinuation secondary to AEs was lower in the CAN-2409 arm (5.4% vs 6%)
The radiation therapy regimens received are summarized below:
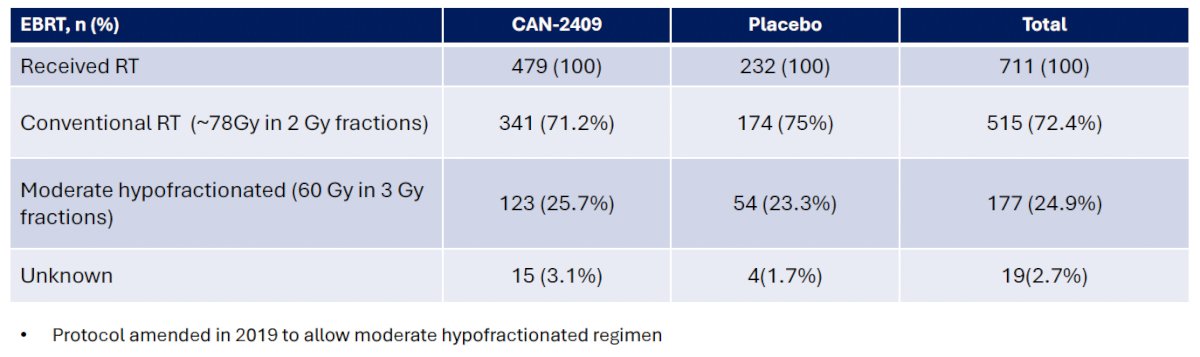
Approximately 25% of patients received moderate hypofractionated radiotherapy, with the protocol amended in 2019 to allow for moderate hypofractionation. Both conventional and moderate hypofractionated regimens were well-tolerated with no significant differences in the safety profiles. Grade ≥3 TRAEs were similar in the CAN-2409 and placebo arms with both
hypofractionated (1.6% vs 1.9%) and standard EBRT (1.8% vs. 1.1%), respectively.
At a median follow-up of 50.3 months, patients in the CAN-2409 arm had a 30% improved disease-free survival rate (HR: 0.70, 95% CI: 0.52–0.94, p=0.0155).

Similarly, patients in the CAN-2409 arm had a 38% reduction in prostate cancer recurrences or prostate cancer-related deaths (HR: 0.62, 95% CI: 0.44-0.87, p=0.0046).

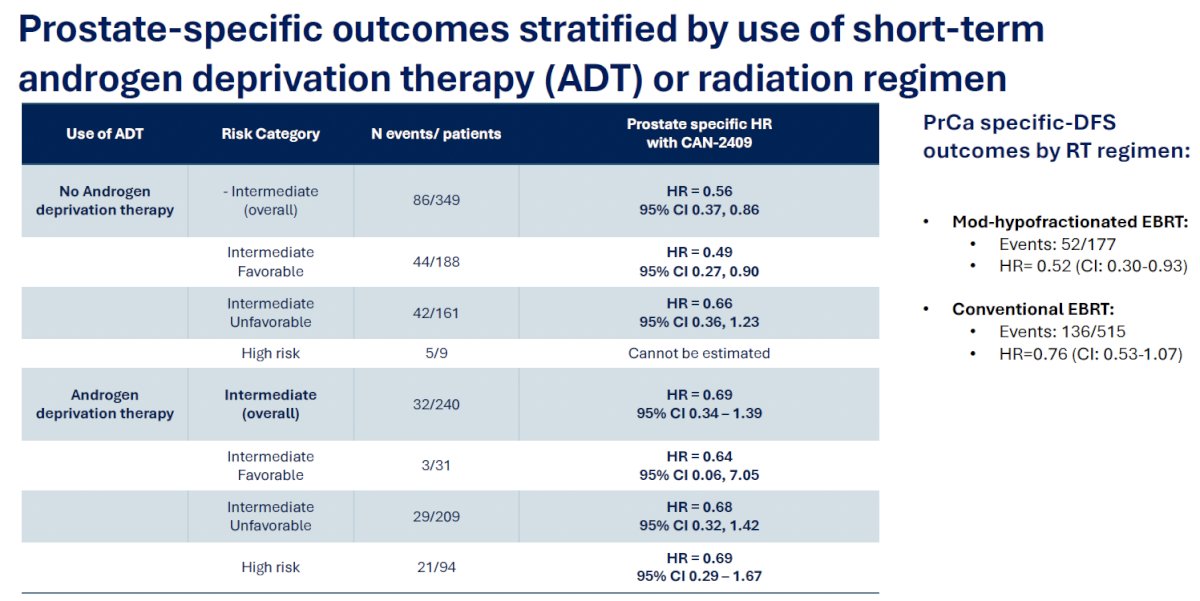
When stratified by the use of short-term ADT and the radiation regimen administered, the study investigators found consistent results in favor of CAN-2409:
- ADT
- No concurrent ADT: HR=0.56, 95% CI 0.37–0.86
- Concurrent ADT: HR=0.69, 95% CI 0.34–1.39
- Radiotherapy regimen
- Moderate hypofractionation: HR=0.52, 95% CI 0.30–0.93
- Conventional fractionation: HR=0.76, 95% CI 0.53–1.07
With regards to other key secondary endpoints:
- There was a significant increase in the proportion of patients achieving a PSA nadir of <0.2 ng/ml in the treatment arm
- 67% vs. 58.6%, respectively (p=0.016)
- Overall survival was similar by treatment arm during study follow-up (median follow up 50 months)
- Only 2 deaths due to prostate cancer (one CAN-2409, one placebo)
- 50 patients died due to other causes, unrelated to treatment
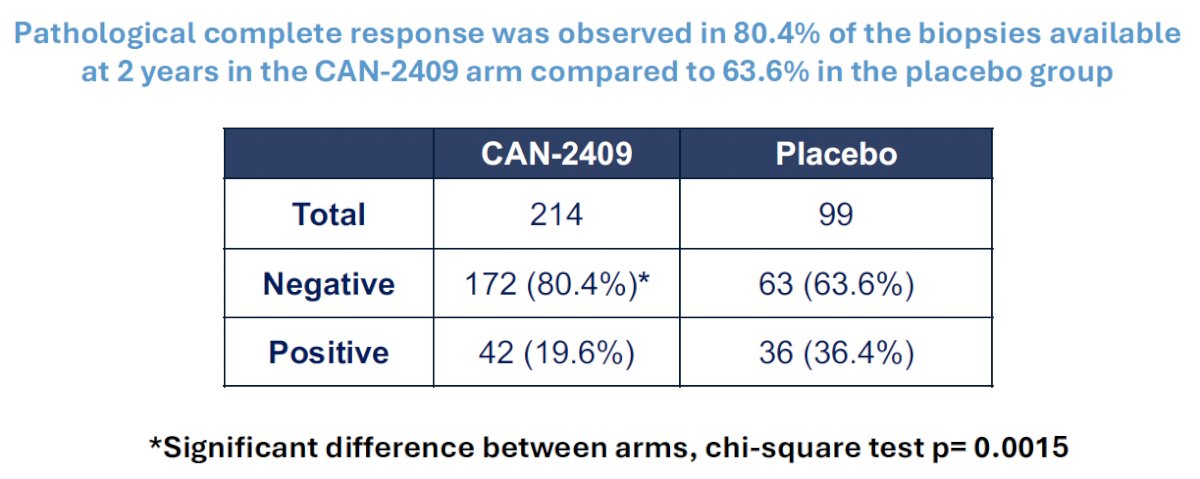
CAN-2409 significantly improved the rate of pathological complete response in the 2-year biopsies (80.4% vs 63.6%, p=0.0015), which is particularly significant given the known associations between positive biopsies ≥2 years after radiotherapy and prostate cancer metastases and mortality rates.
Dr. Gejerman concluded as follows:
- CAN-2409 significantly improved disease-free survival in patients with localized, intermediate- or high-risk prostate cancer treated with standard-of-care EBRT with curative intent (HR: 0.70; p=0.0155)
- CAN-2409 significantly improved prostate cancer-specific outcomes (HR: 0.62; p=0.0046)
- CAN-2409 significantly increased the proportion of patients achieving a PSA nadir of < 0.2 ng/ml compared to placebo (67.1% vs. 58.6%; p=0.0164)
- CAN-2409 significantly improved the rate of pathological complete response in 2-year biopsies, compared to the placebo control arm (80.4% vs. 63.6%; p=0.0015)
- CAN-2409 was safe and well-tolerated
- CAN-2409 immunotherapy could represent the first new therapy in >20 years for men with localized prostate cancer who seek cure
Presented by: Glen Gejerman, MD, MBA, Co-chief of Urologic Oncology and the Medical Director of TomoTherapy® at Hackensack University Medical Center, Bloomfield, NJ
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025