(UroToday.com) The 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting held in San Francisco, CA, was host to an advances in localized prostate cancer session. Dr. Stefano Arcangeli presented the results of ABRUPT, a study evaluating the two-year clinical outcomes following ablative radiotherapy for unfavorable prostate tumors.
Dr. Arcangeli noted that the time is right to evaluate single-dose radiotherapy (SDRT) – one chance to make radiotherapy work while leveraging precision technology and radiobiology to achieve tumor control in ‘record time’.
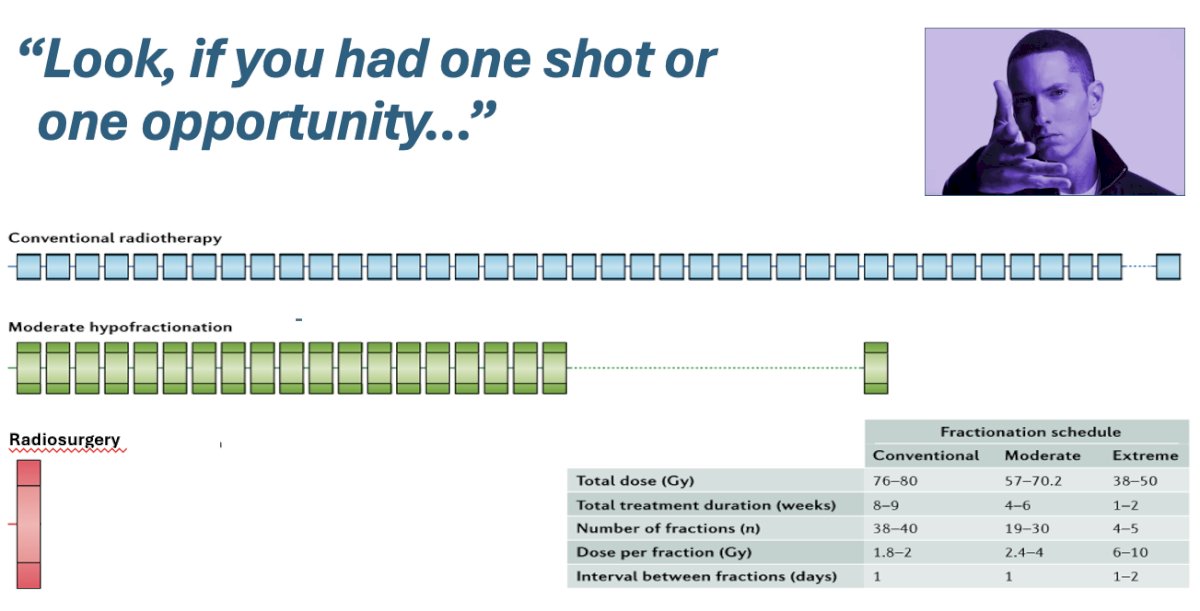
The objective of this study was to assess the gastrointestinal (GI) and genitourinary (GU) side effects of SDRT combined with androgen deprivation therapy (ADT) in patients with organ-confined unfavorable prostate cancer. The study hypotheses were as follows:
- Maximum allowable Grade 2 toxicity rates (H0), based on the results of PACE-B:
- GU: 31%
- GI: 11%
- Sample size: 30 patients to achieve 80% statistical power, assuming a type 1 error rate of 5%, with an alternate hypothesis (H1) of 10% for GU toxicity and 0% for GI toxicity
The inclusion and exclusion criteria were as follows:
- Inclusion:
- Histologically confirmed unfavorable intermediate or select high-risk prostate cancer
- PSA ≤20 ng/ml
- ≤cT3a
- N0M0 per PSMA PET
- WHO performance status 0–1
- IPSS ≤15
- Prostate gland volume <100 cc
- Exclusion:
- Prior pelvic radiotherapy
- Prior surgery for prostate cancer
- Prior TURP
- History of Crohn’s disease or ulcerative colitis
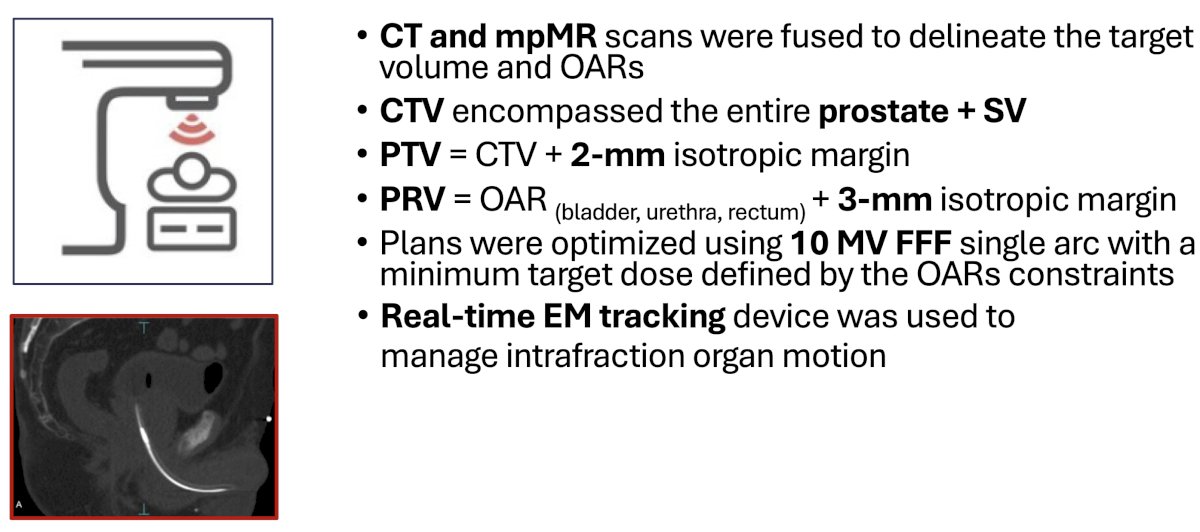
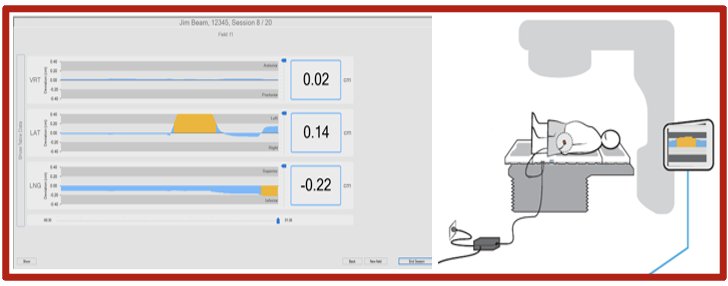
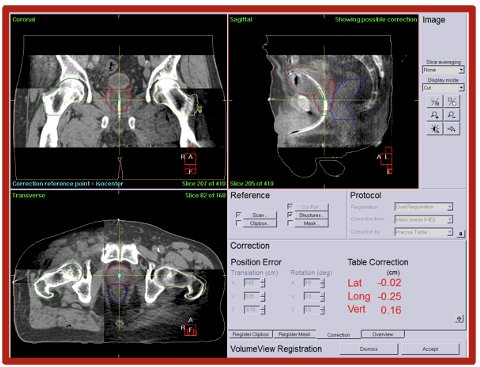
CT and multiparametric MRI scans were fused to delineate the target volume and organs at risk (OAR). The clinical target volume (CTV) included the entire prostate plus seminal vesicles. The planning target volume (PTV) included the CTV + 2 mm isotropic margin. The planning organ at risk volume (PRV) included the OAR (bladder, urethra, rectum) + a 3 mm isotropic margin. The plans were optimized using 10 MV flattening filter-free (FFF) single arc with a minimum target dose defined by the OARs constraints. Real-time electromagnetic tracking devices were used to manage intrafraction organ motion.
The study endpoints were:
- Acute and late toxicities, per CTCAE v.5
- Patient-reported outcomes: Minimal clinically important differences (MCID), defined as >0.5 standard deviations from the baseline EORTC QLQ-PR25/C30 scores
- IPSS score
- Serum PSA level
- mpMRI at 1-hour and 3, 6, and 24 months post-SDRT
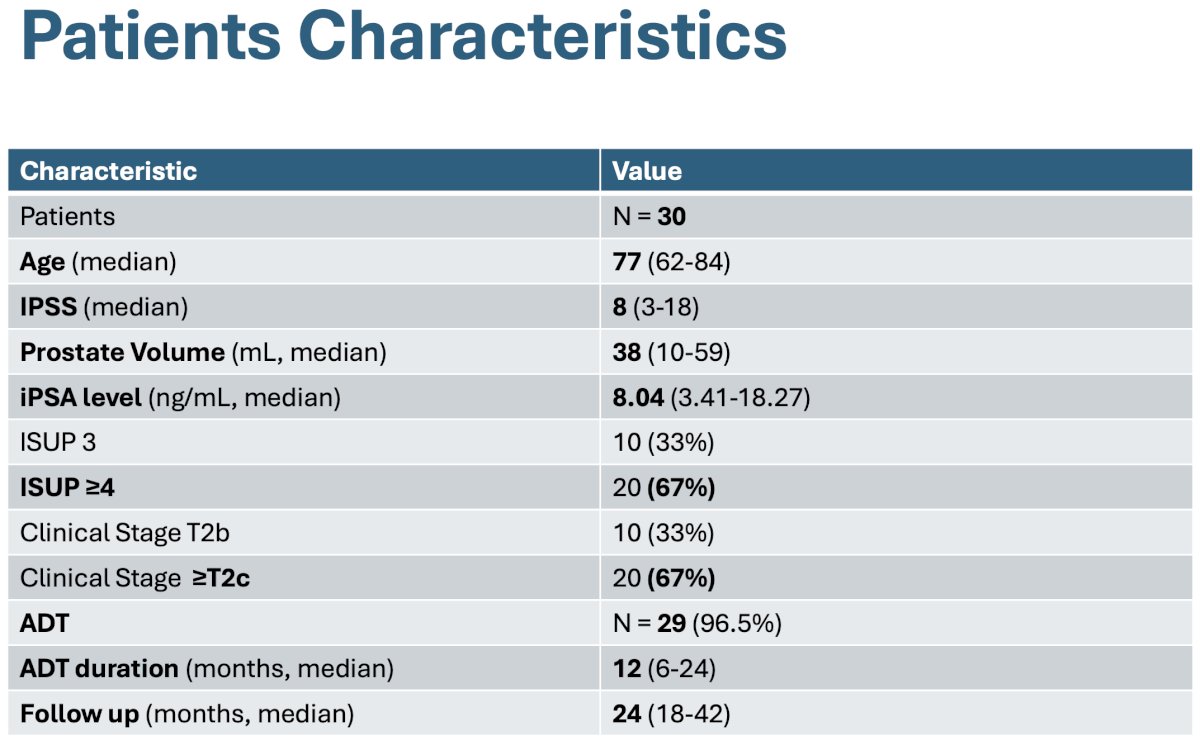
The study cohort included 30 patients, with the patient characteristics summarized in the table below. The median age was 77 years. The median serum PSA level 8 ng/ml, and the median prostate volume was 38 mL. Twenty (67%) patients had Grade Group ≥4 disease. 29/30 patients received ADT for a median duration of 12 months.
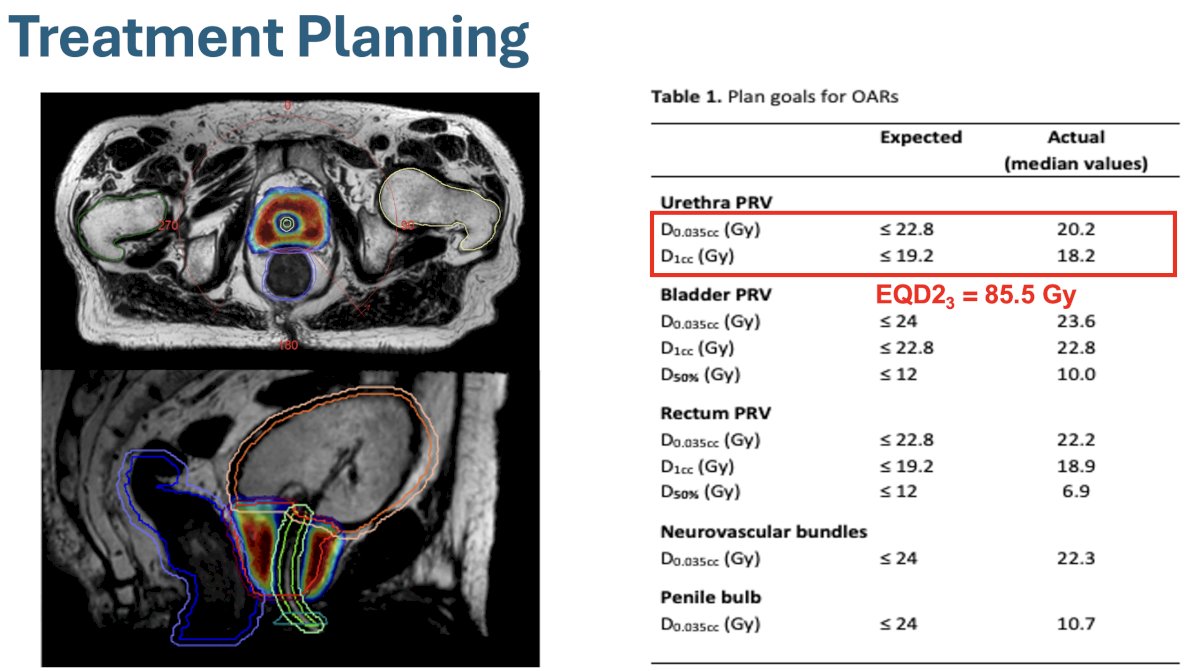
The treatment plan goals for OARs are summarized below:
The median treatment time was 14 minutes, with a median delivery time of 4.3 minutes. Treatment interruptions were required in 57% of the sessions due to ≥1 prostate displacement event >2 mm.
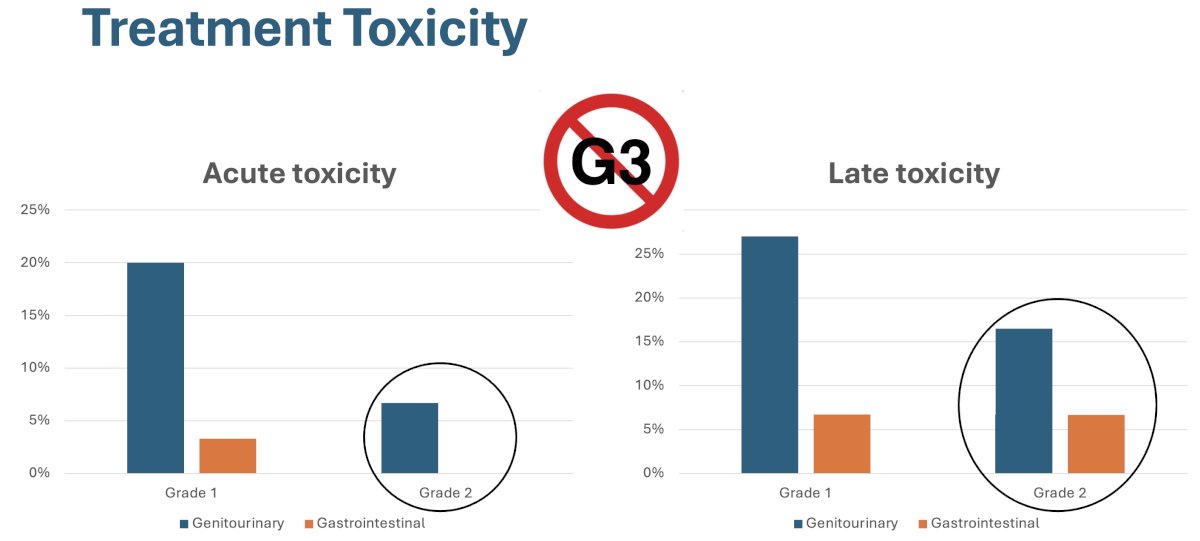
With regards to treatment toxicity, no grade ≥3 events were observed. In the acute setting, Grade 1 and 2 GU toxicity was observed in 20% and 7% of patients, respectively, with Grade 1 GI toxicity in 3% of cases. In the late setting, Grade 1 and 2 GU toxicities were observed in 27% and 16% of patients, respectively, with Grade 1 and 2 GI toxicities observed in 7% of patients.
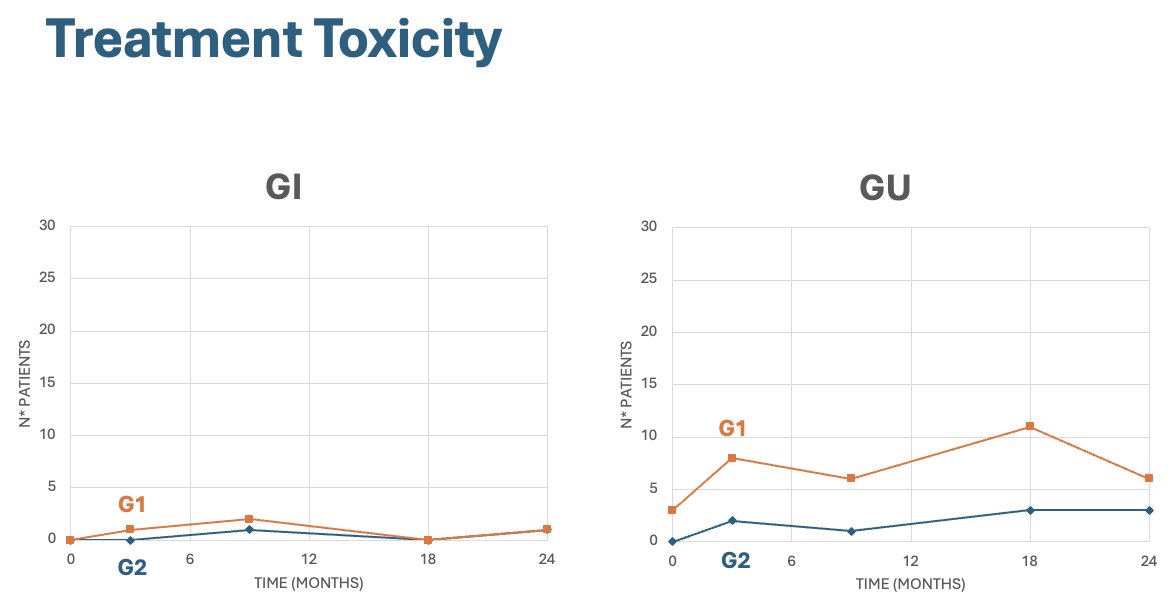
The rates of Grades 1-2 GI and GU toxicities over the 1st 24 months of follow-up are summarized in the plots below:
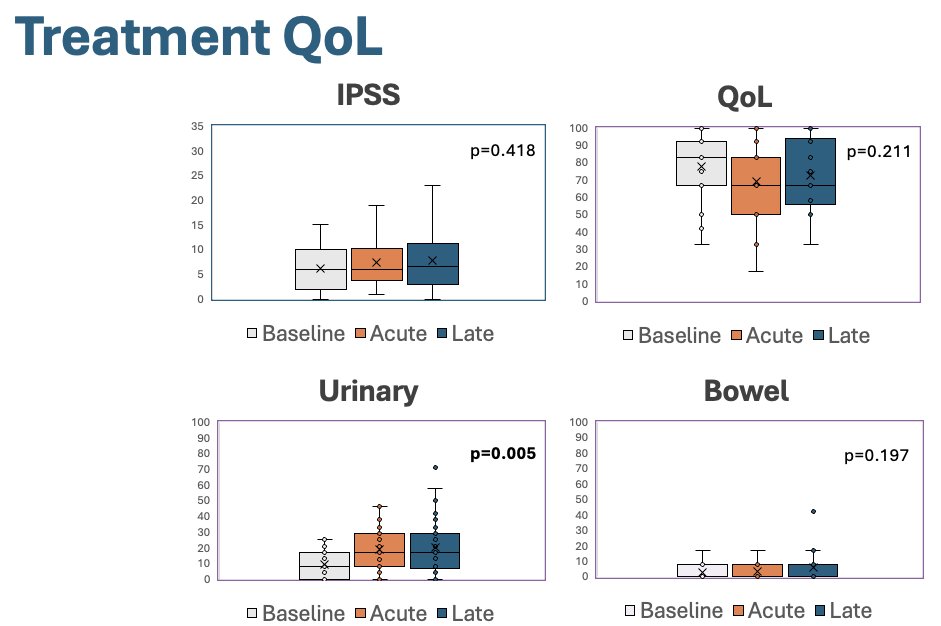
With regards to quality-of-life outcomes, there was a significant worsening in urinary symptoms in both the acute and late phases (p=0.005); however, there were no significant changes in IPSS, overall quality of life, and bowel symptom scores.
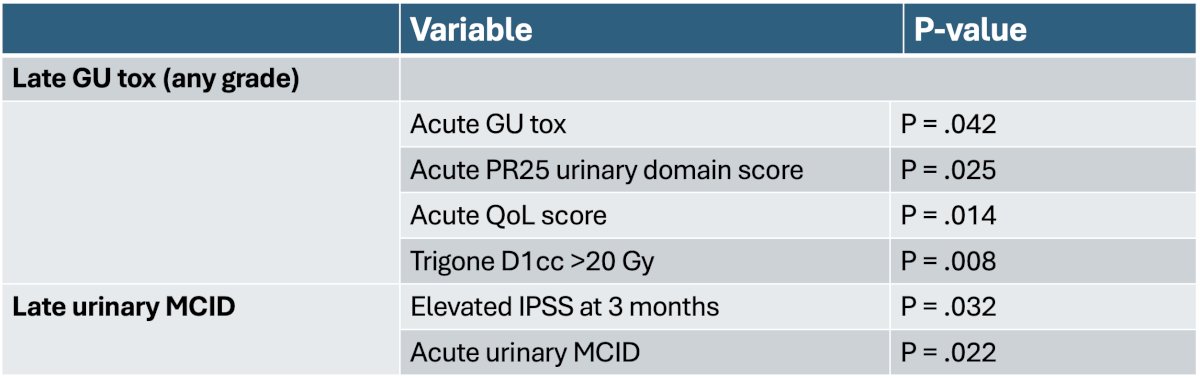
On multivariable analysis, predictors of late GU toxicity (any grade) and late urinary MCIDs were as follows:
At a median follow-up of 24 months, no patient experienced biochemical recurrence, and the median PSA was 0.16 ng/ml (range: 0.01–0.62). 83% of patients had recovered eugonadal testosterone levels.
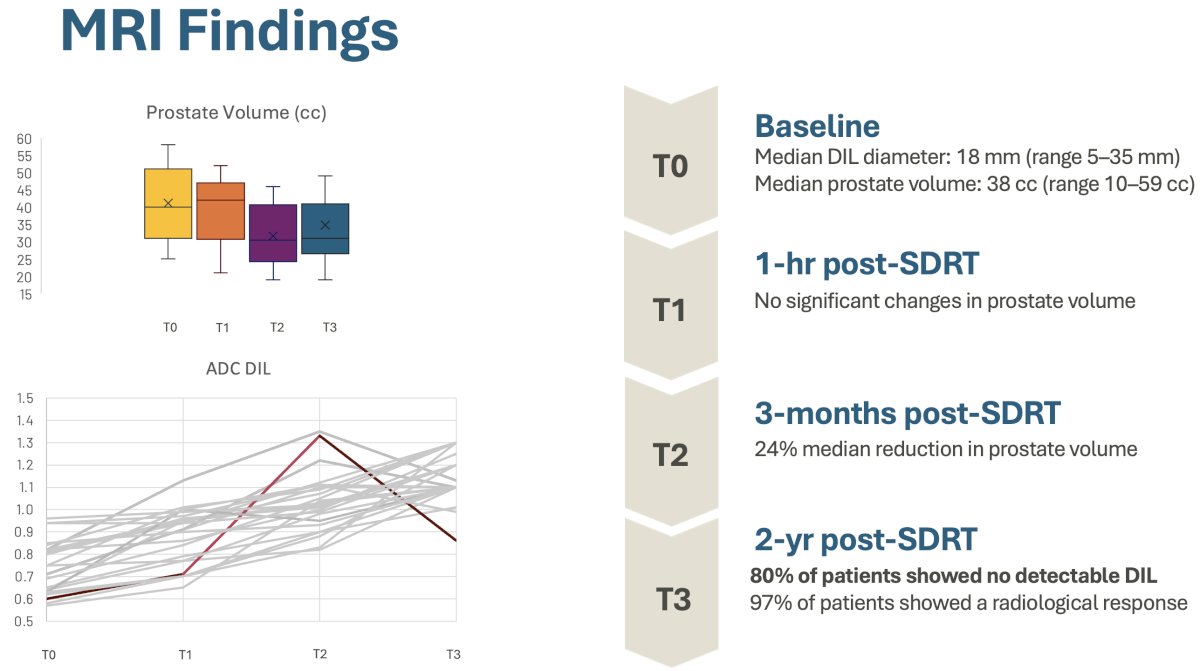
The MRI findings are summarized below. At baseline, the median diameter of the dominant intraprostatic lesion (DIL) was 18 mm. At 1-hour post-SDRT, there were no significant changes in prostate volume. At 3 months post-SDRT, there was a 24% median reduction in prostate volume. At 2 years post-SDRT, 80% of patients had no detectable DIL, and 97% demonstrated evidence of a radiological response.
Dr. Arcangeli concluded with the following take home messages:
- 24 Gy SDRT with urethra sparing and organ motion control, in association with ADT, is feasible and safe in organ confined unfavorable risk prostate cancer with a small prostate volume and good urinary function at baseline
- Late GU toxicity is linked to acute GU toxicity, quality of life, and trigone D1cc >20 Gy
- Could diffusion-weighted (DW) MRI be used as an early biomarker of treatment response?
- Long-term results are awaited to confirm these findings
Presented by: Stefano Arcangeli, MD, Associate Professor, Department of Medicine and Surgery, University of Milan Bicocca, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025