(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco, between September 28 and September 30 was host to the Session 28 - GU 6: Revelations in Renal Radiotherapy. Dr. Shankar Siva presented abstract 264 - Ultra-Hypofractionated Stereotactic Ablative Body Radiotherapy (SABR) for Primary Renal Cell Carcinoma: Pooled Outcomes from the FASTRACK and FASTRACK II Clinical Trials.
Dr. Siva began by highlighting national trends in the surgical management of kidney cancer, referencing NCDB data, which demonstrated that despite growing interest in nephron-sparing approaches, radical nephrectomy remained the predominant surgical treatment for renal masses between 2004 and 2015. While the number of partial nephrectomies steadily increased over the years from 3,568 in 2004 to 4,303 in 2015, radical nephrectomy volumes remained significantly higher, consistently exceeding 14,000 cases annually. These findings underscore an ongoing gap between guideline recommendations favoring nephron-sparing surgery when feasible and real-world practice patterns across the U.S.1

In the evolving landscape of nephron-sparing strategies for renal cell carcinoma (RCC), options include partial nephrectomy, thermal ablation (cryotherapy or radiofrequency ablation), and, more recently, stereotactic ablative body radiotherapy (SABR). While partial nephrectomy remains the gold standard, it is invasive and requires general anesthesia. Thermal ablation offers a less invasive alternative but has limitations in treating peri-hilar or large tumors. SABR stands out as a fully non-invasive, outpatient option that does not require anesthesia and can effectively target large or centrally located tumors, positioning it as a promising tool in the nephron-sparing space.

Dr. Siva highlighted that stereotactic ablative body radiotherapy (SABR), particularly in a 5-fraction regimen, is a commonly used nephron-sparing approach for patients with renal cell carcinoma (RCC). She emphasized findings from an individual patient data meta-analysis from IROCK, which demonstrated favorable 5-year outcomes. Importantly, the majority of patients included (91.3%) were either inoperable or declined surgery, supporting SABR as a viable non-invasive alternative in select cases.2
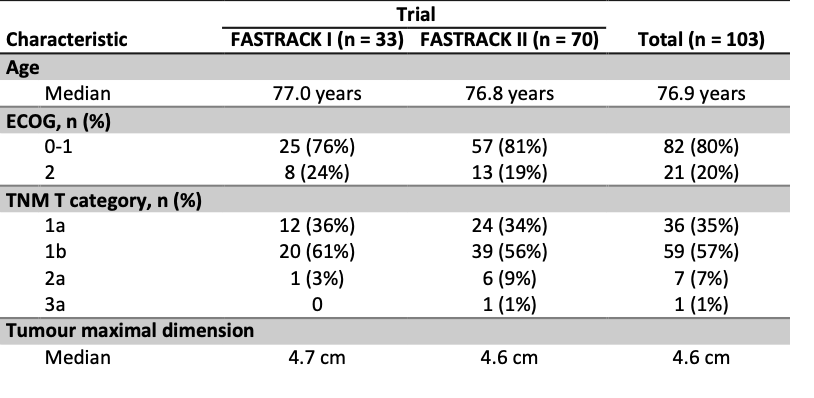
Dr. Siva highlighted the evolution of ultra-hypofractionated SABR for primary RCC through two pivotal trials. The FASTRACK trial (2012–2014), a single-institution proof-of-concept study, enrolled 33 patients and treated 34 primary RCCs, laying the groundwork for broader investigation. This was followed by FASTRACK II (2016–2020), a multi-institutional, international trial that treated 70 patients, aiming to build more robust evidence. Today, she presented a pooled analysis of both trials, further supporting the role of SABR as a nephron-sparing approach in patients who are inoperable or decline surgery.
The intervention included 26 Gy in a single fraction for tumors <4–5 cm and 42 Gy in 3 fractions for tumors ≥4–5 cm. She highlighted that, based on RCC-specific α/β ratios (either 2.6 Gy or 6.9 Gy), both regimens achieve comparable biological effective doses ranging from 123–286 Gy, suggesting a strong radiobiologic rationale for high-dose hypofractionation in this setting. The ITV was defined as the GTV on 4DCT plus an internal margin, with a uniform 5 mm isotropic expansion applied to generate the PTV. In FASTRACK I, treatment was predominantly delivered using 3DCRT, IMRT was also utilized in select cases.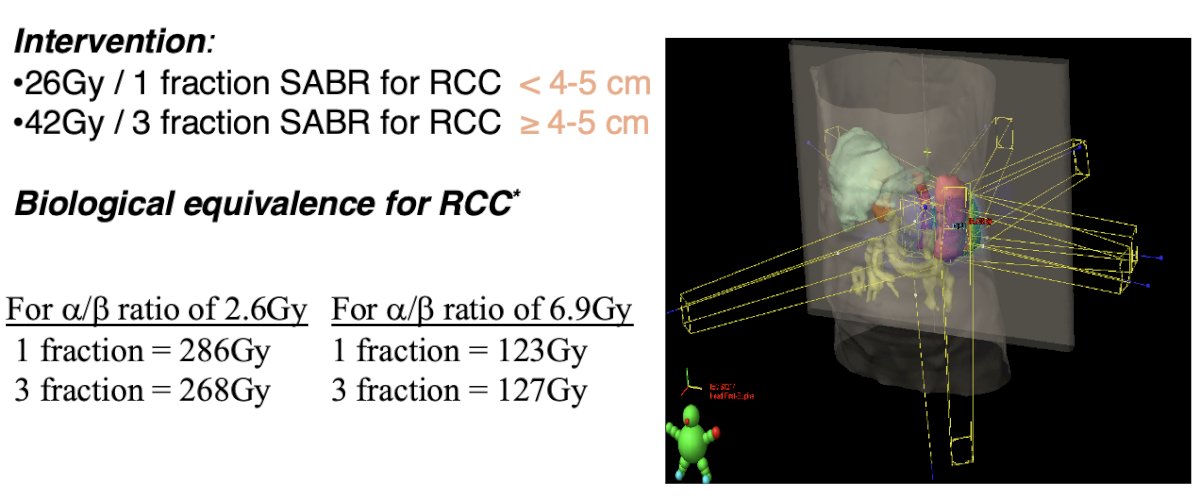
Patient characteristics from the pooled FASTRACK I and II trials (n=103) showed a median tumor maximal dimension of 4.6 cm, with similar measurements across both cohorts. The majority of patients had clear cell RCC (76%) and preserved renal function, with a mean eGFR of 59.3 mL/min.
The treatment was well tolerated, with no grade 4 or 5 adverse events reported. Grade 3 toxicity occurred in 7.7% of patients, and the overall adverse event rate was 87%. The most common treatment-related toxicities were fatigue (64%) and abdominal/flank pain (49%), followed by nausea/vomiting (29%) as shown below.

In terms of efficacy, with a median follow-up of 3.5 years (IQR: 2.3–4.3), the pooled analysis demonstrated excellent local control rates of 100% at 1 year and 98% at both 3 and 5 years.

Similarly, freedom from distant failure remained high, with rates of 97% at 1, 93% at 3 years, and 83% at 5 years.

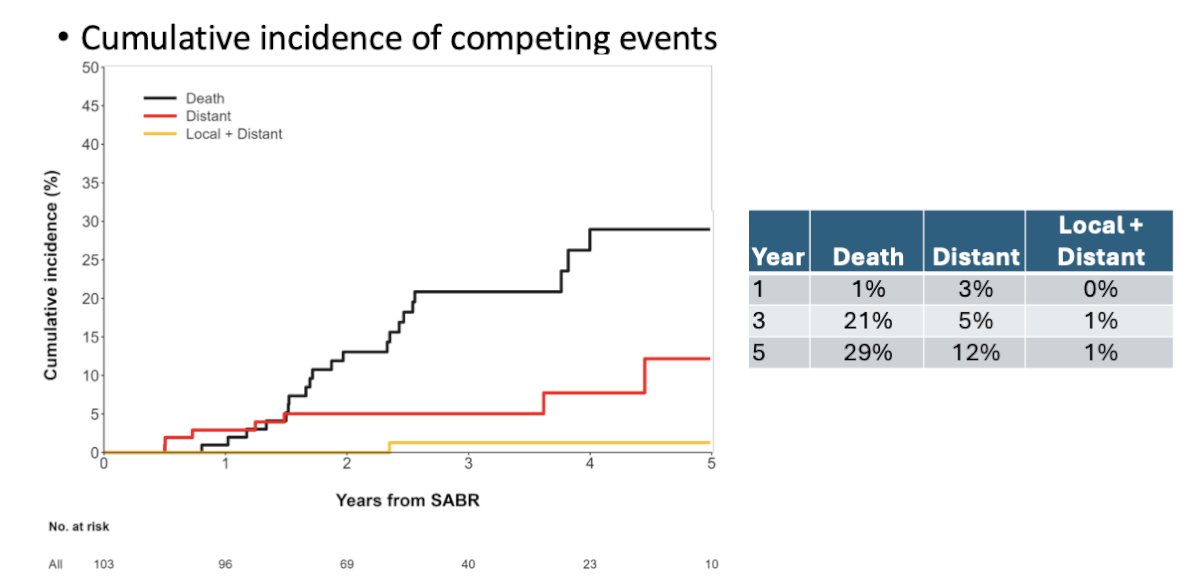
Cumulative incidence analysis showed that by 5 years, 12% of patients experienced distant failure, 1% had both local and distant failure, and 29% had died highlighting that while local control was excellent, competing risks from death and distant progression remain relevant in this population. Dr. Siva emphasized that the observed 5-year death rate (29%) likely reflects the advanced age of the study population, with a median age of 77 years and some patients as old as 91.
Regarding renal function, there was a gradual decline in eGFR from a baseline of 59 mL/min to 43 mL/min at 5 years, accompanied by a corresponding increase in creatinine from 109 to 145 µmol/L, though changes appeared to stabilize after year 2.

Dr. Siva concluded by highlighting that this cohort had larger tumors (median 4.6 cm) compared to those typically seen in trials of radical versus partial nephrectomy or thermal ablation. Despite this, outcomes were favorable, with only one local failure and one cancer-related death. The renal function decline 12 mL/min at 3 years and 16 mL/min at 5 years was comparable to what is expected with thermal ablation or partial nephrectomy in patients with underlying CKD. The safety profile was excellent, with only 7.7% experiencing grade 3 adverse events and no grade 4 or 5 events, potentially aided by routine use of steroids and antiemetics. Techniques used were relatively basic, suggesting that future optimization could further improve nephron-sparing and reduce toxicity.
Dr Siva wrapped up the presentation with the following conclusions:
- To our knowledge, this is the largest analysed prospective trial cohort(s) of a non-surgical curative treatment for primary RCC.
- Pooled results of high-dose single and three fraction SABR show the approach is highly effective, nephron sparing, and safe.
- Findings support the use of ultra-hypofractionated SABR schedules for primary RCC.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.
References:
- Tan WS, Berg S, Cole AP, Krimphove M, Marchese M, Lipsitz SR, Nabi J, Sammon JD, Choueiri TK, Kibel AS, Sun M, Chang S, Trinh QD. Comparing Long-Term Outcomes Following Radical and Partial Nephrectomy for cT1 Renal Cell Carcinoma in Young and Healthy Individuals. JNCI Cancer Spectr. 2019 Feb 1;3(1):pkz003. doi: 10.1093/jncics/pkz003. Retraction in: JNCI Cancer Spectr. 2020 Oct 17;4(4):pkaa056. doi: 10.1093/jncics/pkaa056. PMID: 31360891; PMCID: PMC6649692. – Retracted Article
- Siva S, Ali M, Correa RJM, Muacevic A, Ponsky L, Ellis RJ, Lo SS, Onishi H, Swaminath A, McLaughlin M, Morgan SC, Cury FL, Teh BS, Mahadevan A, Kaplan ID, Chu W, Grubb W, Hannan R, Staehler M, Warner A, Louie AV. 5-year outcomes after stereotactic ablative body radiotherapy for primary renal cell carcinoma: an individual patient data meta-analysis from IROCK (the International Radiosurgery Consortium of the Kidney). Lancet Oncol. 2022 Dec;23(12):1508-1516. doi: 10.1016/S1470-2045(22)00656-8. Epub 2022 Nov 16. PMID: 36400098.