(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session 28 - GU 6: Revelations in Renal Radiotherapy. Dr. Chad Tang discussed the four presentations from the Revelations in Renal Radiotherapy session.
Dr. Tang structured his discussion into two categories: i.) localized RCC, highlighting trials by Siva, Onishi, and Ali, and ii.) oligometastatic RCC, focusing on the phase IIb trial reported by Assadi.
Localized Renal Cell CarcinomaDr. Onishi presented the long-term follow-up results of a multicenter, prospective phase 2 trial of Stereotactic Body Radiotherapy (SBRT) for primary RCC, which Dr. Tang noted was a very well-conducted analysis with an impressive median follow-up of 76 months. The study enrolled 49 patients between 2007 and 2017, with a median age of 73 years and ECOG performance status 0–2. Most patients were treated as initial therapy (n=40), while nine had prior contralateral nephrectomy. Median tumor diameter was 27 mm, and SBRT was delivered in 10 fractions at total doses of 50, 60, or 70 Gy.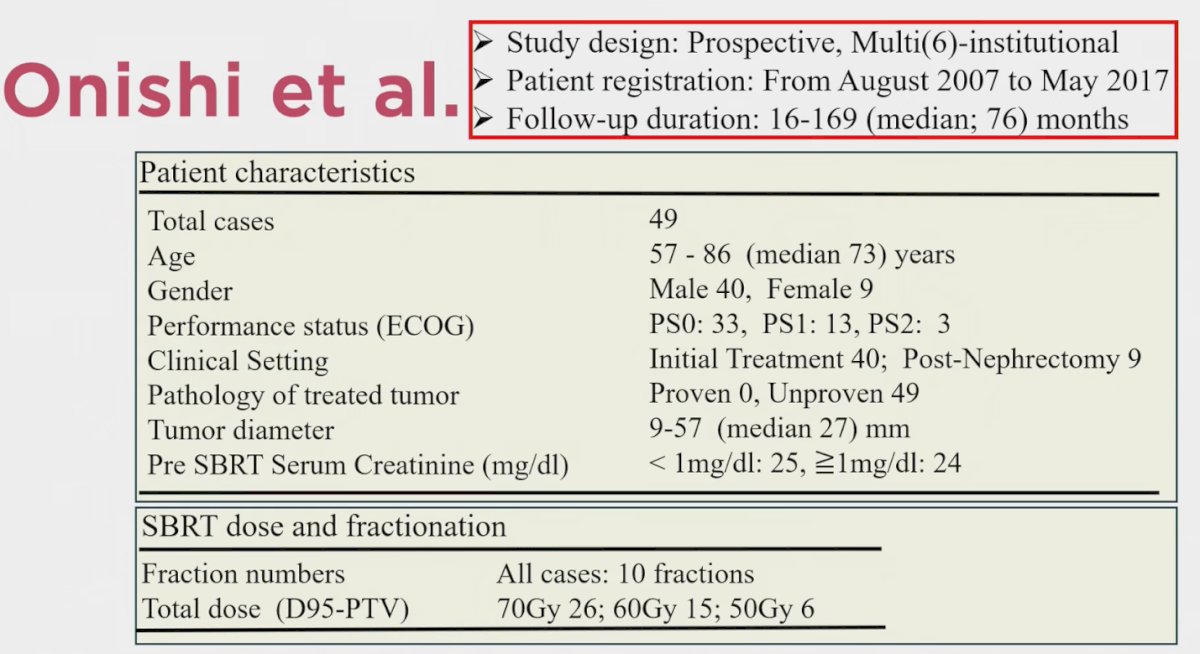
Dr. Tang also highlighted the combined analysis of FASTRACK I and II presented by Dr. Siva, which included 103 patients with primary RCC treated across single- and multi-institutional settings. The median follow-up was 3.5 years, with patients having a median age of 77 years and mostly ECOG 0–1. Tumor maximal dimension was approximately 4.6–4.7 cm, and the majority were stage T1b. He emphasized that this pooled dataset provided excellent outcomes with SBRT and further strengthened the evidence base for non-surgical management of localized RCC.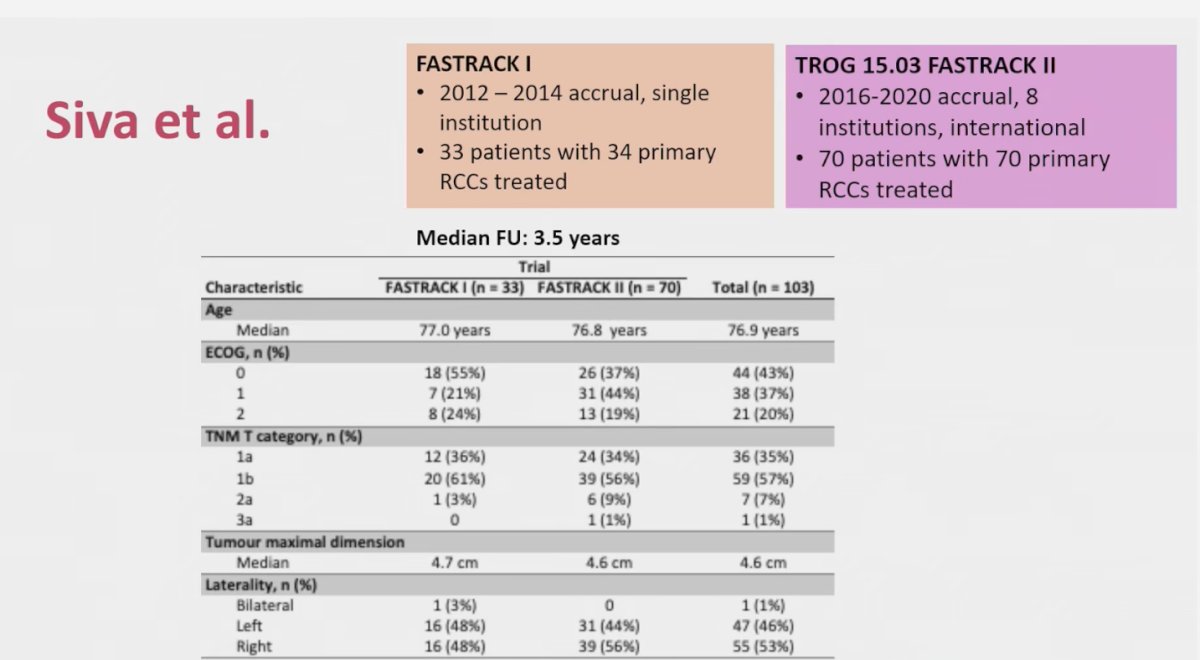
Notably, both studies demonstrated excellent long-term local control, with Dr. Onishi reporting 100% at 5 years and Dr. Siva’s pooled FASTRACK analysis showing 98% at 5 years, with only two documented failures to date.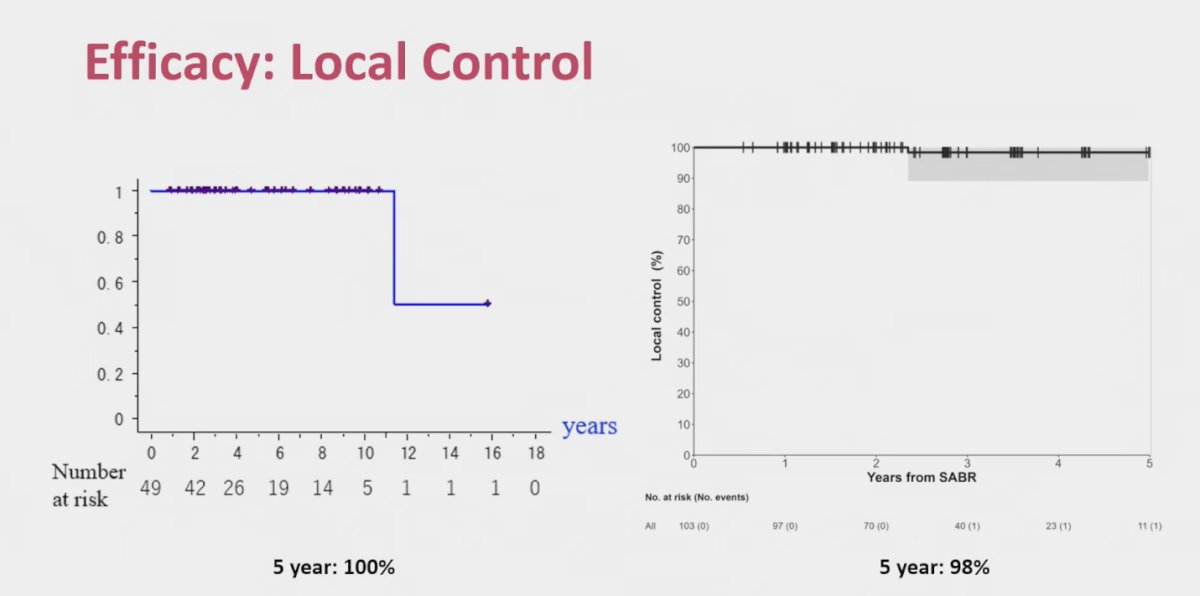
Dr. Tang further contextualized these findings with a recent meta-analysis by Huang et al., which compared ablative therapies in localized RCC across more than 9,000 patients. Among 612 patients treated with SBRT, 5-year local control was 95%, comparable or superior to radiofrequency ablation (92%), microwave ablation (86%), and cryoablation (90%). Importantly, for tumors ≥4 cm, SBRT maintained the highest 5-year local control at 93%, versus 79% with radiofrequency ablation, 82% with microwave ablation, and 85% with cryoablation. These data underscore the durability of SBRT, even in larger tumors.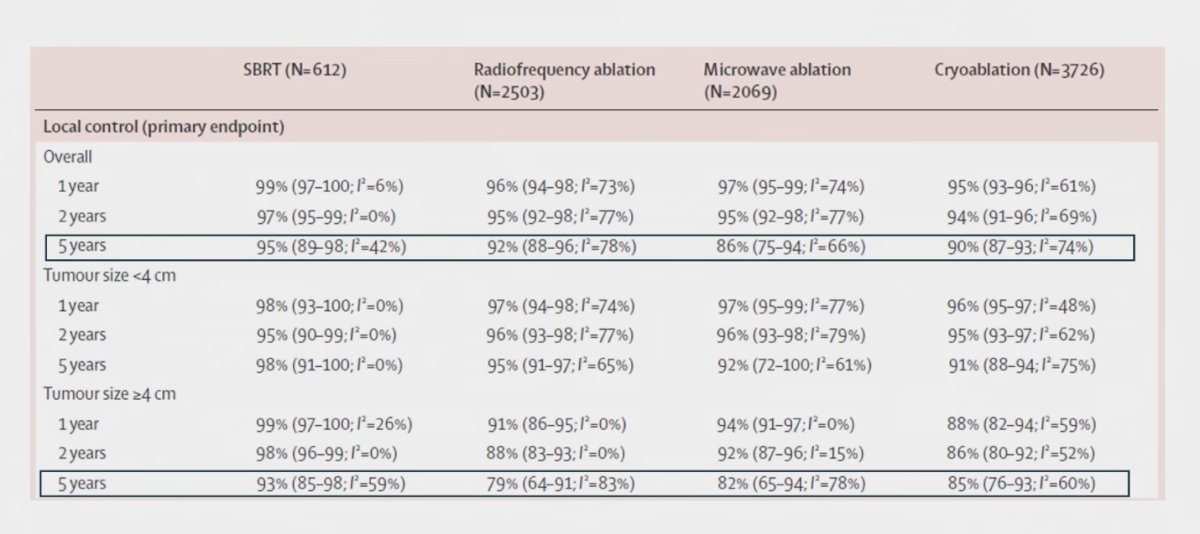
Another key finding across both trials was excellent cause-specific survival. Dr. Onishi reported a 5-year CSS of 95.2%, while Dr. Siva’s pooled FASTRACK analysis demonstrated a 5-year CSS of 98%, underscoring the durability of SBRT in primary RCC.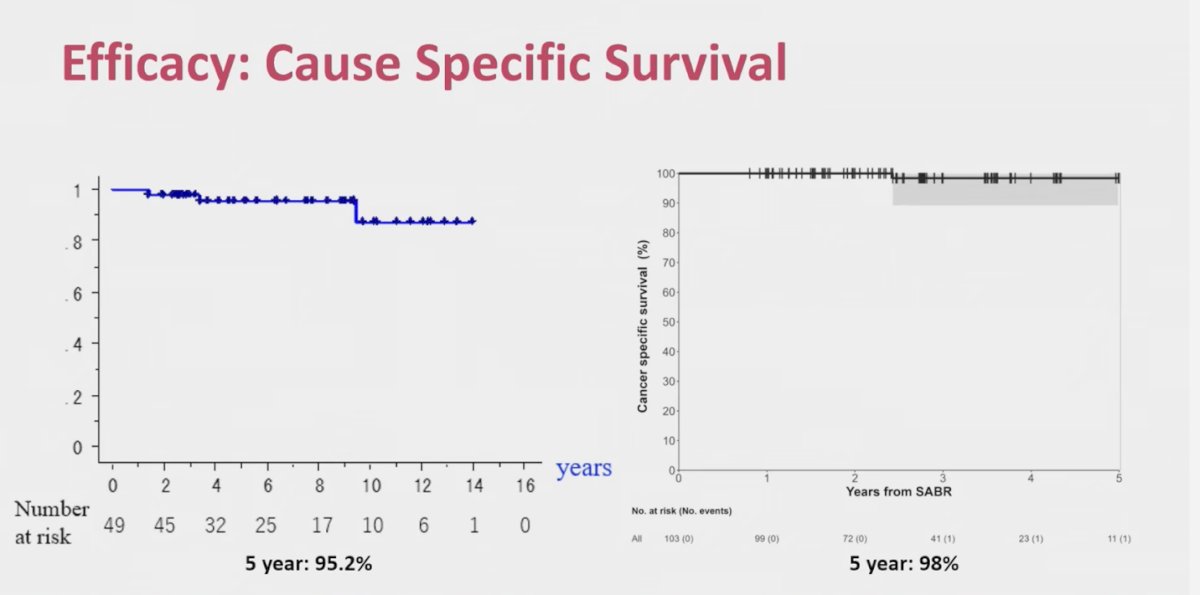
This finding was consistent with the Huang et al. meta-analysis, where 5-year CSS exceeded 95% across SBRT, radiofrequency ablation, microwave ablation, and cryoablation. These results reinforce that localized RCC treated with ablative therapies rarely results in disease-specific mortality.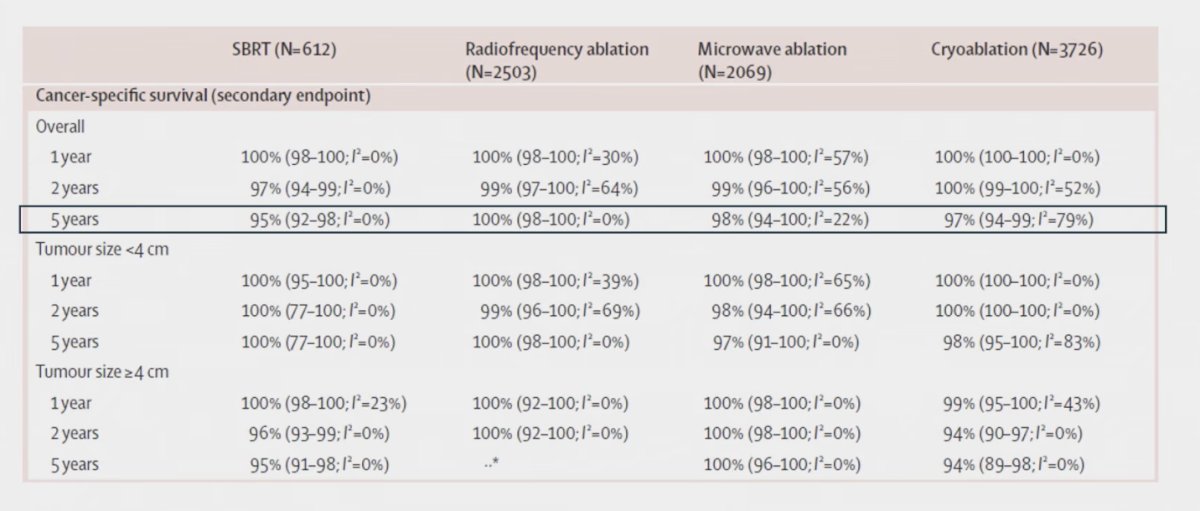
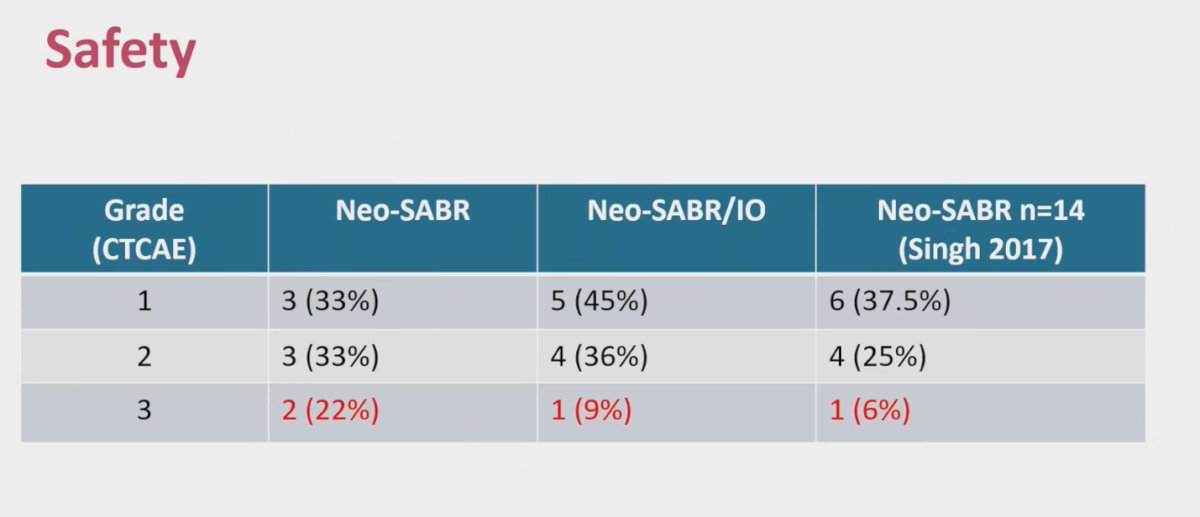
Finally, both trials confirmed that SBRT is generally safe and well tolerated. Dr. Tang noted that he counsels patients about the possibility of a one-quarter decline in renal function, consistent with the observed creatinine increases in 24.5% of patients, particularly those with a solitary kidney. Grade 3–4 gastrointestinal events were rare, occurring in only one patient in each study, both with tumors adjacent to the duodenum or colon. Overall, grade 3 toxicities were reported in 7.7%, with no grade 4 or 5 events, aligning with the safety profile seen in the meta-analysis. Localized RCC- Neoadjuvant Dr. Tang next discussed the NAPSTER trial, presented by Dr. Ali, a randomized phase II study enrolling 20 patients with primary clear cell RCC (T1b–T3a, N1, or low-volume M1) planned for nephrectomy. Patients were randomized to receive SABR alone (42 Gy in three fractions) or SABR combined with three cycles of neoadjuvant pembrolizumab, administered prior to surgery. The primary endpoint was major pathological response, defined as <10% residual tumor at nephrectomy, along with evaluation of tumor-responsive T cells. Secondary endpoints included safety, immune correlates, and PD-L1/L2 expression.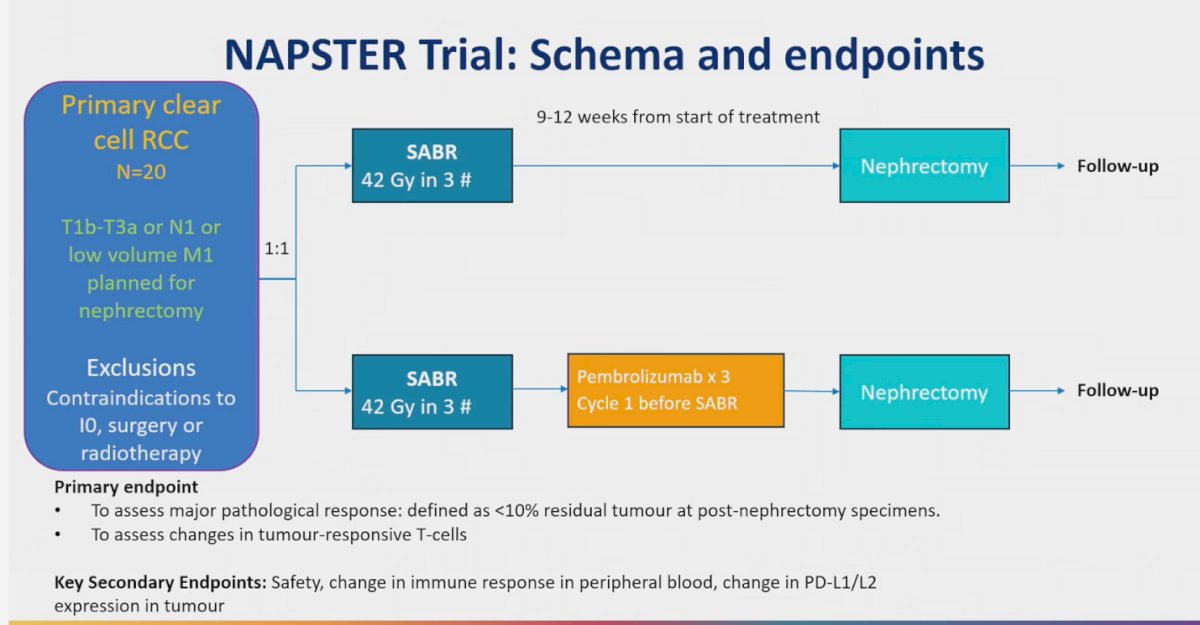
Unlike in other malignancies, complete histologic tumor clearance is rarely observed in RCC. In NAPSTER, residual tumor was present in nearly all patients, regardless of whether they received SABR alone or in combination with pembrolizumab. However, early immune correlates suggested biological activity, with increases in CD8+ T-cell subsets, including effector and exhausted populations, in patients receiving combined therapy. These findings indicate that while SABR ± IO may not induce total histologic regression, it may prime the immune microenvironment and warrant further investigation.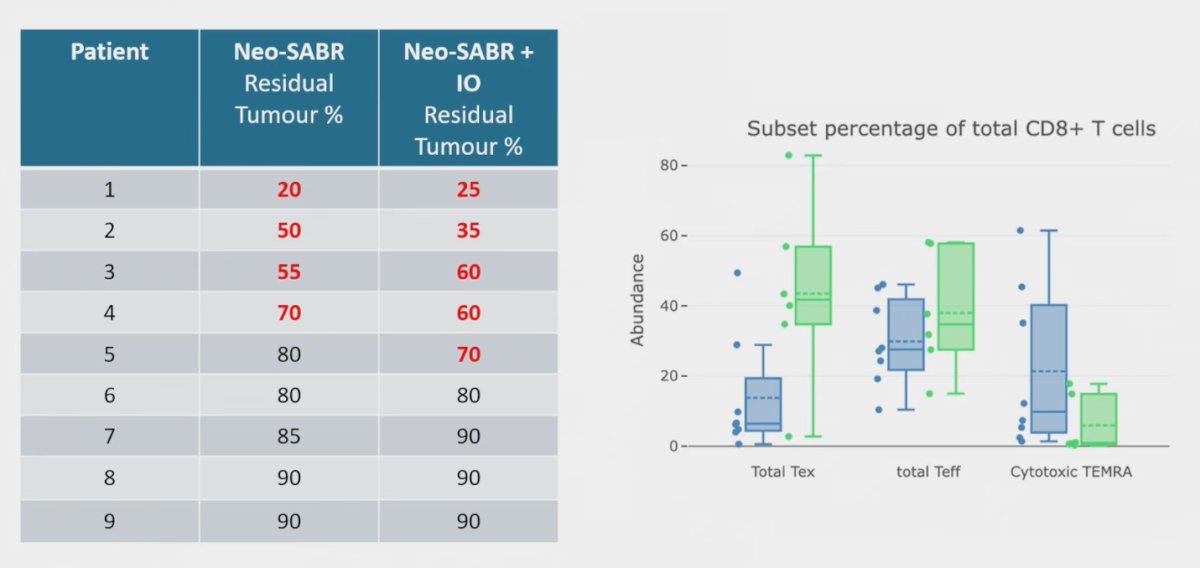
Dr. Tang compared these findings with a pilot study of SBRT combined with cytoreductive nephrectomy in metastatic RCC. While overall CD8+ infiltration was not significantly increased, SBRT was associated with higher levels of proliferating CD8+ T cells (Ki67+) and FOXP3+ regulatory T cells. He noted that, when considered alongside NAPSTER, the addition of PD-1 inhibition may further shape the immune microenvironment, though more work is needed to fully define these interactions.2
Oligometastatic RCC
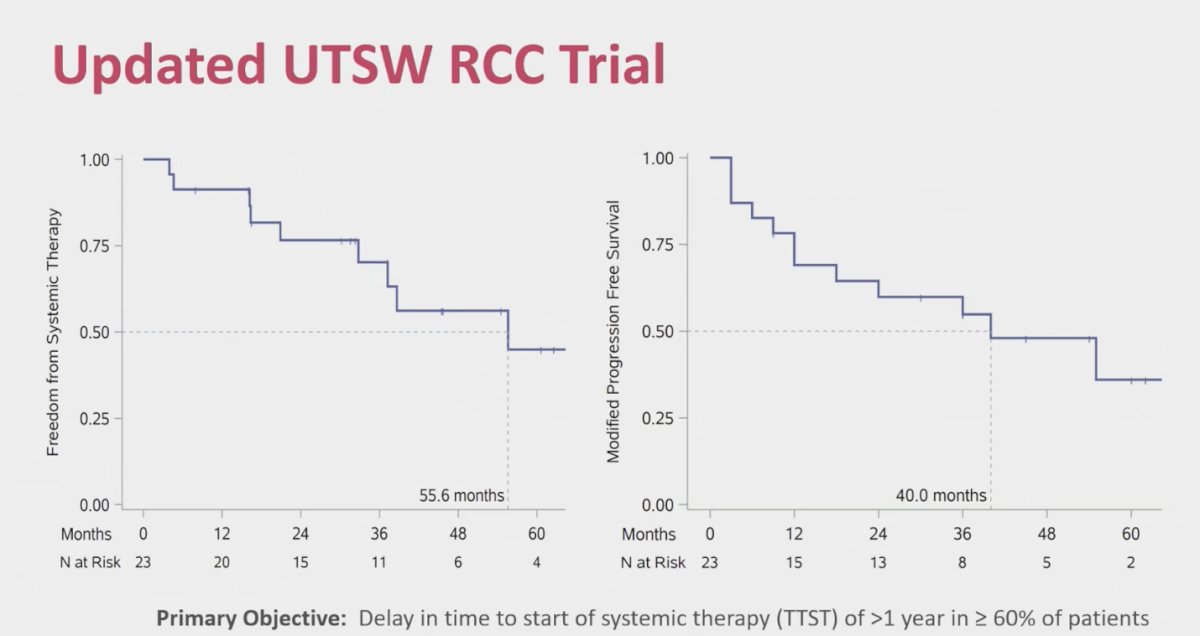
Lastly, Dr. Tang reviewed the updated UTSW RCC trial data presented by Dr. Assadi, which evaluated SBRT in systemic therapy–naïve oligometastatic RCC. The primary objective of delaying time to systemic therapy was achieved, with freedom from systemic therapy exceeding one year in more than 60% of patients and a median of 55.6 months. Modified progression-free survival was 40 months, highlighting the potential of SBRT to defer systemic treatment while maintaining disease control in this population.
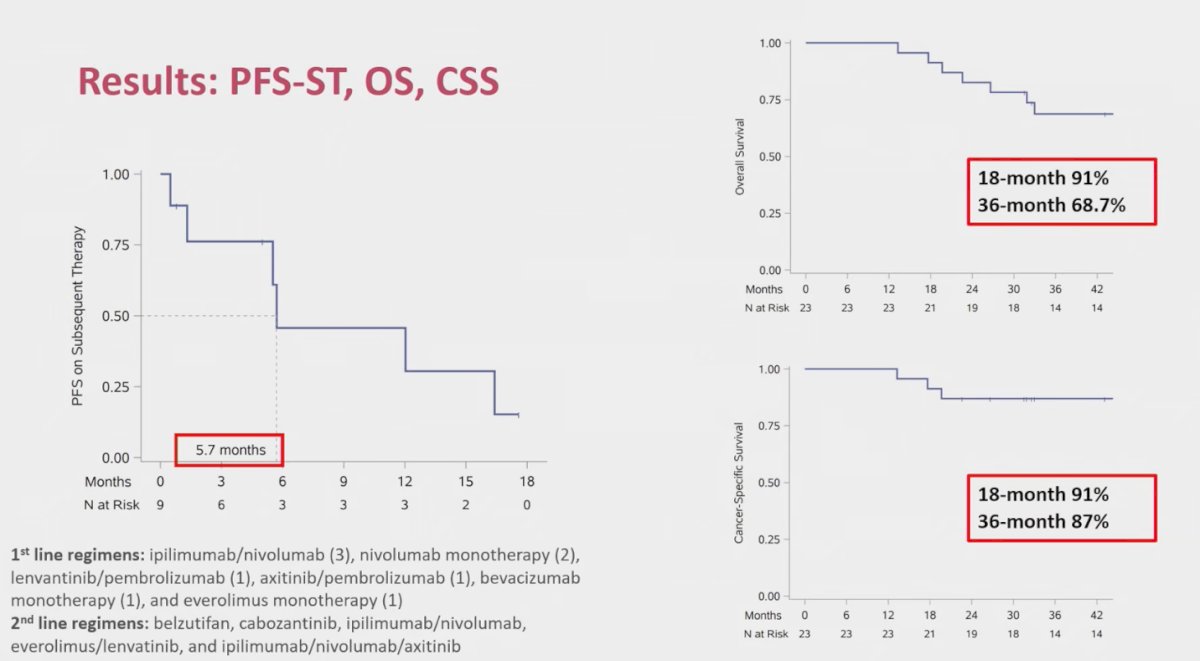
However, progression-free survival on first-line systemic therapy was shorter than expected, with a median of just under six months. In contrast, survival outcomes were encouraging, with overall survival rates of 91% at 18 months and 68.7% at 36 months, and cancer-specific survival of 91% at 18 months and 87% at 36 months. These data suggest that while subsequent systemic therapy responses may be modest, long-term outcomes with SBRT remain favorable.
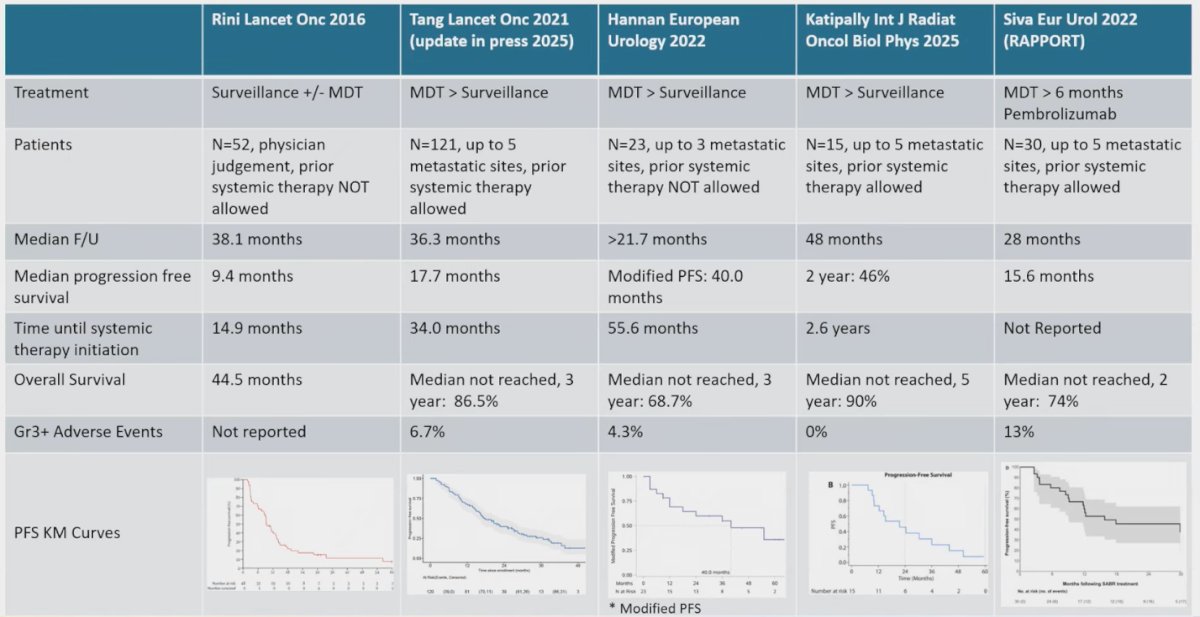
In the oligometastatic setting, Dr. Tang reviewed the growing body of evidence beginning with Rini et al. in 2016 and now supported by multiple series showing favorable outcomes with MDT, including improvements in median PFS and excellent OS. As summarized in the table, PFS has ranged from 15 to 55 months across recent studies, with 3-year OS rates consistently high. Dr. Tang highlighted the RAPPORT study presented by Dr. Siva, which combined MDT with pembrolizumab, reporting a median PFS of 15.6 months and a 2-year OS rate of 74%.3 He cautioned that careful attention should be paid to the tail of the PFS curves, as observed in several studies, suggesting that a subset of patients may derive long-term benefit from MDT.
Dr. Tang concluded his presentation with the following take-home messages:
- For localized RCC, Onishi et al and Siva et al. showed that radiation to the primary tumor leads to excellent long-term local control
- In the pre-operative setting, Ali et al. show that radiation and pembrolizumab alter the recruitment of immune cell populations into the kidney stroma
- In the oligometastatic setting, Assadi et al. show long-term control and freedom from systemic therapy with SBRT and surveillance
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.
References:
- Huang RS, Chow R, Benour A, Chen D, Boldt G, Wallis CJD, Swaminath A, Simone CB 2nd, Lock M, Raman S. Comparative efficacy and safety of ablative therapies in the management of primary localised renal cell carcinoma: a systematic review and meta-analysis. Lancet Oncol. 2025 Mar;26(3):387-398. doi: 10.1016/S1470-2045(24)00731-9. Epub 2025 Feb 5. PMID: 39922208.
- Singh AK, Winslow TB, Kermany MH, Goritz V, Heit L, Miller A, Hoffend NC, Stein LC, Kumaraswamy LK, Warren GW, Bshara W, Odunsi K, Matsuzaki J, Abrams SI, Schwaab T, Muhitch JB. A Pilot Study of Stereotactic Body Radiation Therapy Combined with Cytoreductive Nephrectomy for Metastatic Renal Cell Carcinoma. Clin Cancer Res. 2017 Sep 1;23(17):5055-5065. doi: 10.1158/1078-0432.CCR-16-2946. Epub 2017 Jun 19. PMID: 28630212; PMCID: PMC5581708.
- Siva S, Bressel M, Wood ST, Shaw MG, Loi S, Sandhu SK, Tran B, A Azad A, Lewin JH, Cuff KE, Liu HY, Moon D, Goad J, Wong LM, LimJoon M, Mooi J, Chander S, Murphy DG, Lawrentschuk N, Pryor D. Stereotactic Radiotherapy and Short-course Pembrolizumab for Oligometastatic Renal Cell Carcinoma-The RAPPORT Trial. Eur Urol. 2022 Apr;81(4):364-372. doi: 10.1016/j.eururo.2021.12.006. Epub 2021 Dec 23. PMID: 34953600.