(UroToday.com) The 2022 ASTRO annual meeting featured a session on new insights into post-prostatectomy radiotherapy, including a presentation by Wesley Armstrong discussing results from the prospective randomized phase 3 trial PSMA SRT. For men with recurrence after primary local therapy, salvage therapy is a chance for disease control (and potentially a cure), which may be aided by PSMA guidance:

The purpose of the randomized PSMA SRT trial is to compare the success rate of salvage radiation therapy for recurrence of prostate cancer after radical prostatectomy with (intervention arm) and without (control arm) planning based on PSMA PET/CT. At the ASTRO 2022 annual meeting, Armstrong and colleagues reported the secondary endpoint of the trial: impact of PSMA PET/CT on the treatment plan.
This is a randomized, controlled, prospective, open label, phase 3 clinical trial with institutional funding. There were 193 patients randomized to proceed with standard salvage radiation therapy with any conventional imaging aside from PSMA PET/CT (control arm) or undergo a 68Ga-PSMA-11 PET/CT scan prior to salvage radiation therapy (investigational arm). The following information was collected on case-report forms before randomization (intended salvage radiation therapy plan) and after treatment:
- Radiation field region (prostate fossa, pelvic lymph node)
- Total dose
- Dose per fraction
- Duration
- ADT use and duration
- PSMA influence on target volume
- Other (free-text)
Changes between salvage radiation therapy plan before randomization and delivered treatment were classified as Major, Minor or No Change.
Major change: change of ADT duration ≥3 months, change of standard radiotherapy volumes (prostate fossa and pelvic lymph node), target volume delineation beyond standard radiotherapy field, simultaneous-integrated boost beyond standard radiotherapy fields, and initiation of advanced systemic therapy (novel ADT agents, chemotherapy).
Minor change: simultaneous-integrated boost within standard radiotherapy fields. Fisher exact test was used to compare prevalence of events between study arms.
These 193 patients were enrolled from September 6, 2018 to August 17, 2020 and enrollment is complete. There were 90 patients randomized to the control group and 103 to the PSMA group. The median time from radical prostatectomy to enrollment and median PSA was 20.3 months (IQR 1.4–245) and 0.3 ng/ml (IQR 0.2-10.3), and 28.3 months (IQR 1.2–21) and 0.23 ng/ml (IQR 0.1-29.9), respectively. The control arm had 13 dropouts (17%) while the intervention had one (1%):
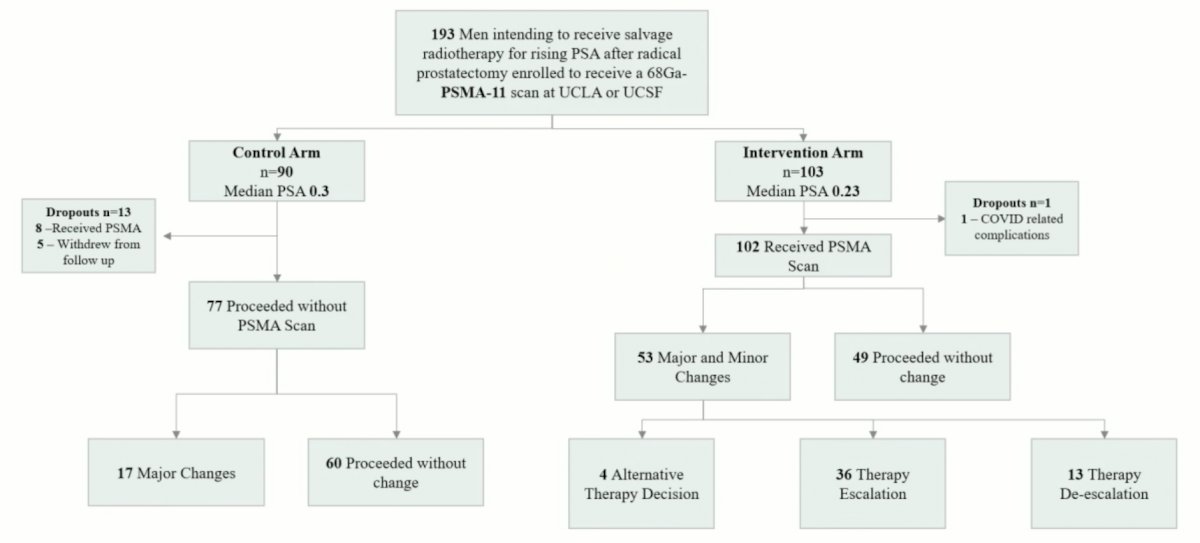
PSMA was positive in 38% of patients at a median PSA of 0.23: 12% outside of pelvis (M1), 31% in pelvic lymph nodes (N1), and 18% in the prostate (T+). Pre-randomization radiotherapy plan and delivered radiotherapy plan were available in 100% of patients, including 86% of the controls and 99% of those in the PSMA arm (p = 0.0004). There were 0% and 7% minor changes in the control and PSMA groups, respectively (p = 0.02). There were 22% and 44% major changes in the control and PSMA groups, respectively (p = 0.004). Treatment escalation occurred in 41% and 69% (p = 0.048), and de-escalation in 59% and 19% (p = 0.004), respectively. There were 9 patients that received advanced systemic therapy in relation to PSMA findings whereas only 1 patient in the control received advanced therapy (p = 0.044).
Wesley Armstrong concluded his presentation discussing results from the prospective randomized phase 3 trial PSMA SRT with the following take home messages:
- Current guidelines recommend PSMA use for restaging but lack guidelines for “how to use” in management guidance
- In this prospective randomized phase 3 study, major changes between the pre-randomization salvage radiation therapy plan and the delivered radiotherapy plan was more common in the PSMA intervention group than the conventional imaging control group
- We await biochemical recurrence free survival data in this cohort and will evaluate differences in benefit in relation to escalation, de-escalation, and PSMA influence
Presented by: Wesley R. Armstrong, MD, PhD candidate, Ahmanson Translational Theranostics Division, UCLA Nuclear Medicine, Los Angeles, CA
Co-Authors: A. U. Kishan2, K. Booker1, W. P. Fendler1, T. Hope3, N. G. Nickols4, J. Czernin1, and J. Calais1; 1Ahmanson Translational Theranostics Division, UCLA Nuclear Medicine, Los Angeles, CA, 2Department of Radiation Oncology, University of California, Los Angeles, Los Angeles, CA, 3Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, 4University of California Los Angeles, Department of Radiation Oncology, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Radiation Oncology (ASTRO) Annual Hybrid Meeting, San Antonio, TX, Sat, Oct 22 – Wed, Oct 26, 2022.