(UroToday.com) The 2022 ASTRO annual meeting featured a session on considerations for the treatment of PSMA-staged high-risk patients, including a presentation by Dr. Evan Thomas discussing when occult metastases become oligometastatic disease with PSMA PET staging. With regards to PSMA PET, Dr. Thomas notes that there is a new sheriff in town. Indications for PSMA PET/CT include (i) upfront staging in the setting of suspected metastasis for potentially curable men, and (ii) suspected recurrence based on increasing PSA after prior therapy. However, there are several questions surrounding PSMA PET/CT:
- What are the implications of PSMA PET/CT findings before definitive treatment?
- What do we do with the new sites we find?
- How do new metastatic findings affect our decision to treat the primary?
- When do we consider metastasis directed therapy?
Fortunately, data is coming, given that there is a very large number of open and planned studies for PSMA PET based staging and decision making. From a review from the EAU Section of Oncological Urology (ESOU) board,1 the following are ongoing trials assessing the role of metastasis-directed therapy in metastatic prostate cancer:
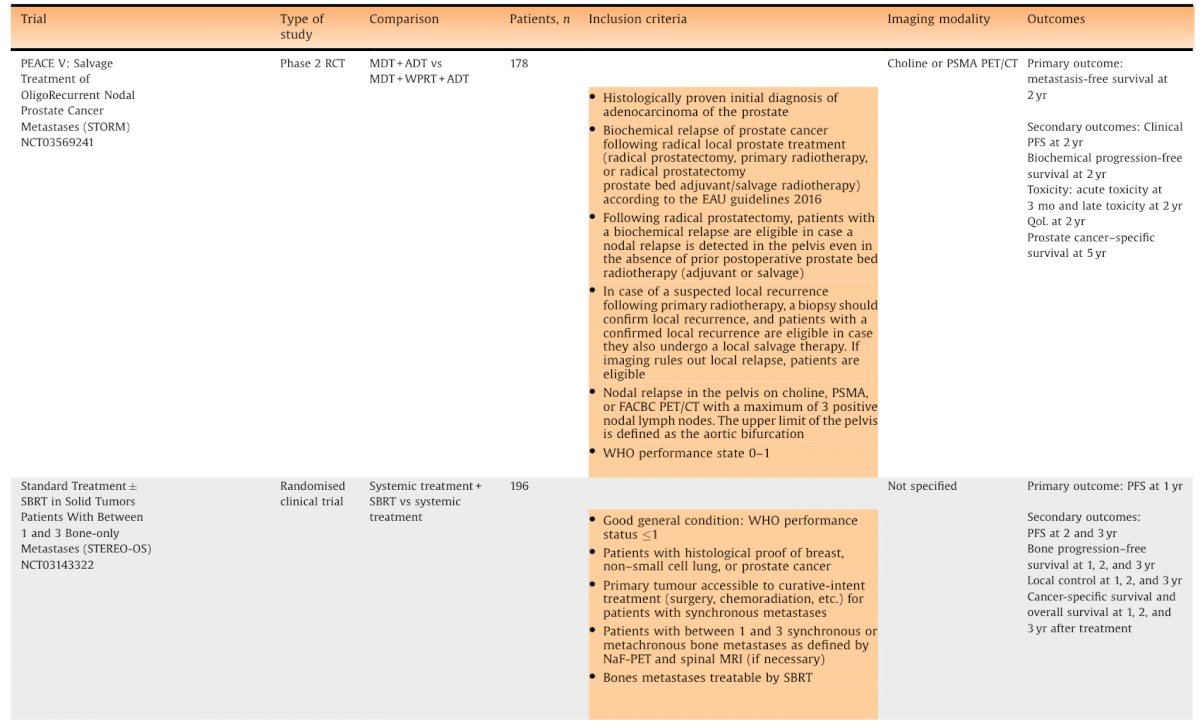
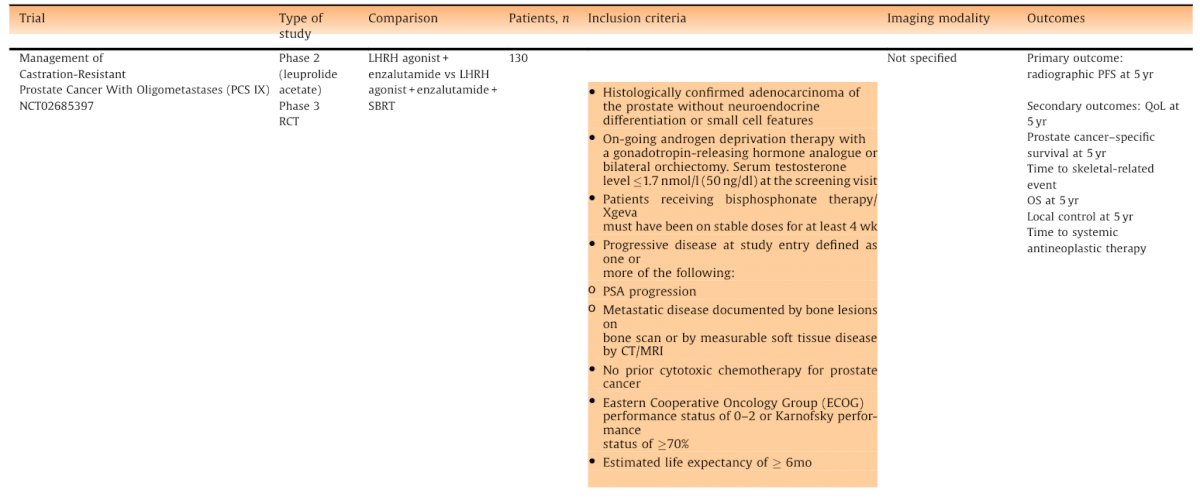
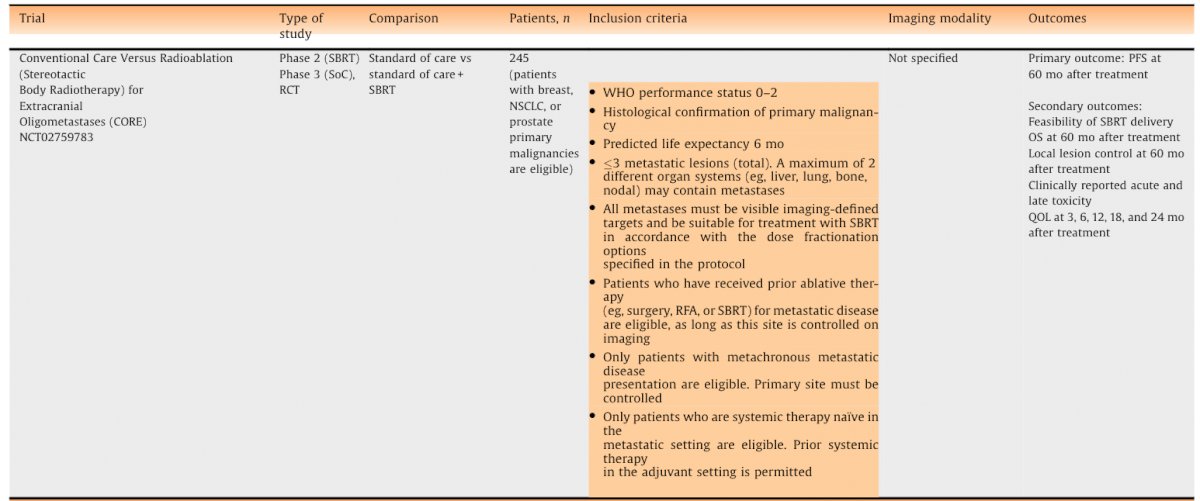
Indeed, there is emerging evidence for metastasis-directed therapy, with a potential OS benefit in appropriately selected patients. Prostate cancer patients comprise a large majority of patients accrued to oligometastatic metastasis directed therapy studies. However, there is no phase 3 data for PSMA-directed prostate cancer oligometastatic data, although there are promising phase 2 data with an overall response rate of 60%, including 22% rendered biochemical no evidence of disease.2
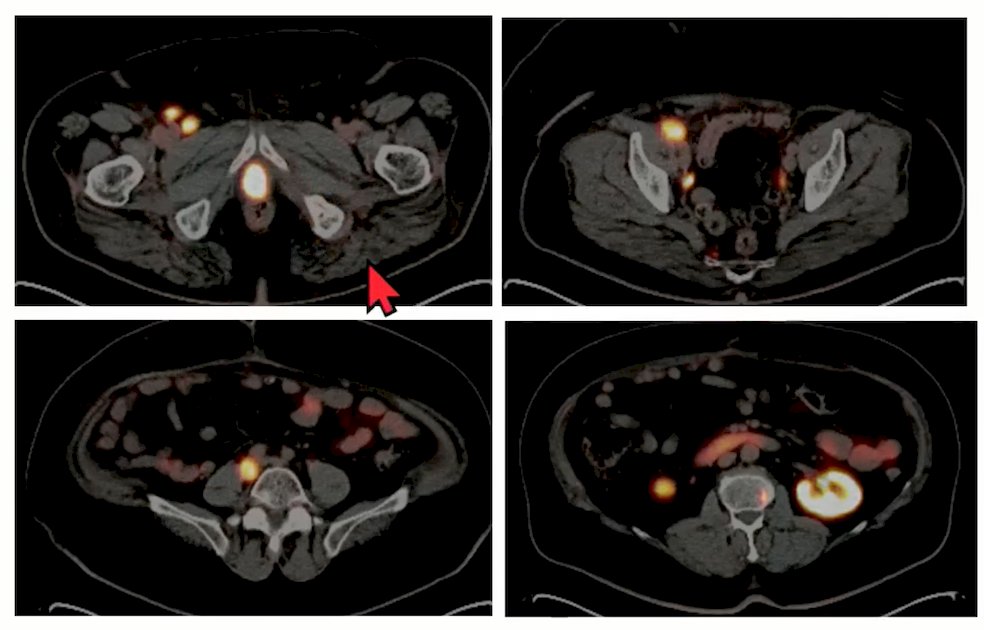
Dr. Thomas then discussed four cases utilizing PSMA PET/CT in the oligometastatic disease setting. Case 1 was a 55 year old healthy male with regional risk prostate cancer (T1cN1, Gleason grade 5 in 2/12 cores) and a PSA of 90.1 ng/mL. A Tc-99m nuclear bone scan was negative and a CT scan showed a solitary 1 cm peri-rectal lymph node. The patient declined radical prostatectomy + pelvic lymph node dissection, and thus a PSMA PET/CT was ordered and confirmed the positive lymph node, in addition to 3 PSMA-avid bone metastases:
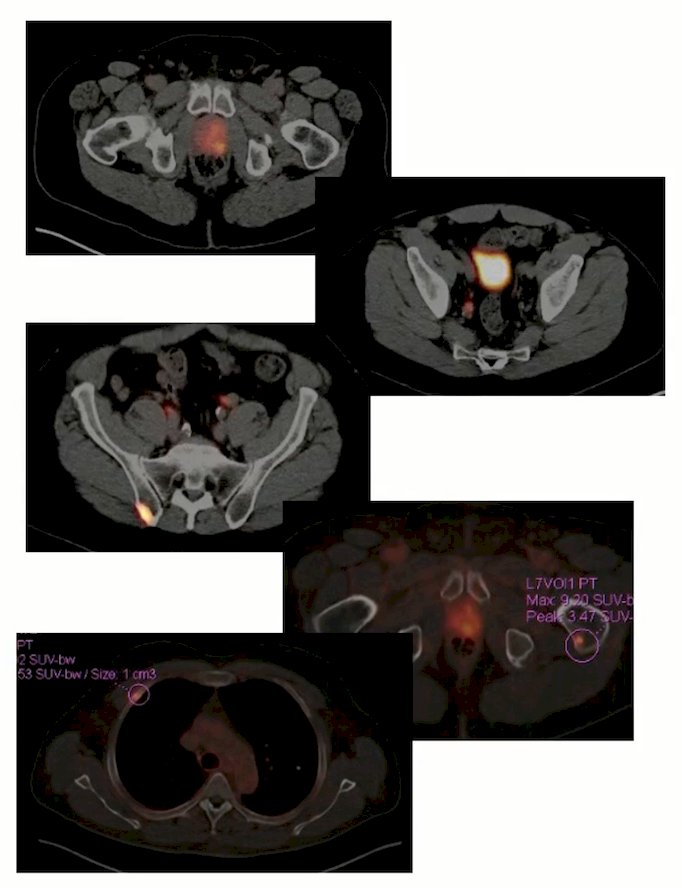
Management of this patient is challenging: do you manage him as N1 (based on the pre-PSMA PET era) or as low volume M1 (based on the PSMA PET era)? An N1-based regimen would include external beam radiotherapy to the prostate (with pelvic lymph node coverage) and a long course of ADT (+/- abiraterone). Bone metastases would be left to the systemic therapy for treatment. An M1-based regimen would include ADT + abiraterone or darolutamide or enzalutamide, or ADT + docetaxel + abiraterone or darolutamide, or ADT + radiotherapy to the primary (most would probably include the lymph nodes). Again, bone metastases would be left to the systemic therapy for treatment. Although we do have some data regarding metastasis directed therapy, in this setting, metastasis directed therapy should still be considered experimental. Existing evidence, according to Dr. Thomas, suggest there is probably a benefit in properly selected patients, particularly those with a long life expectancy. Ultimately, well-designed randomized clinical trials are necessary to test metastasis directed therapy in the setting of de novo, oligometastatic prostate cancer. Regarding the case 1 patient, options were discussed with the patient to understand how aggressive he wanted to be and his threshold for risk/benefit of therapy. This patient desired aggressive therapy, so he received 70 Gy in 28 fractions to the prostate with a boost to the dominant nodule (84 Gy), 50.4 Gy in 28 fractions with a boost to PET-avid node (61.6 Gy), 30 Gy in 3 fractions to each of the 3 bone metastasis sites, and ADT (neoadjuvant and concurrent) + abiraterone.
Case 2 was a 49 year old male with mCRPC to the bone and past medical history of Lynch syndrome, hypertension, and stage 3 kidney disease. In June 2020, his PSA was 169 ng/mL and he was diagnosed with Gleason 5 + 4 prostate cancer and subsequently treated with Casodex/Lupron; he also received ADT + radiotherapy (50 Gy to the pelvis with a 30 Gy boost to the prostate). In February 2021, he completed radiotherapy with a PSA nadir of 4.62 ng/mL and remained on ADT. In November 2021, his PSA was rising and an L4 and calvarial metastasis was discovered:
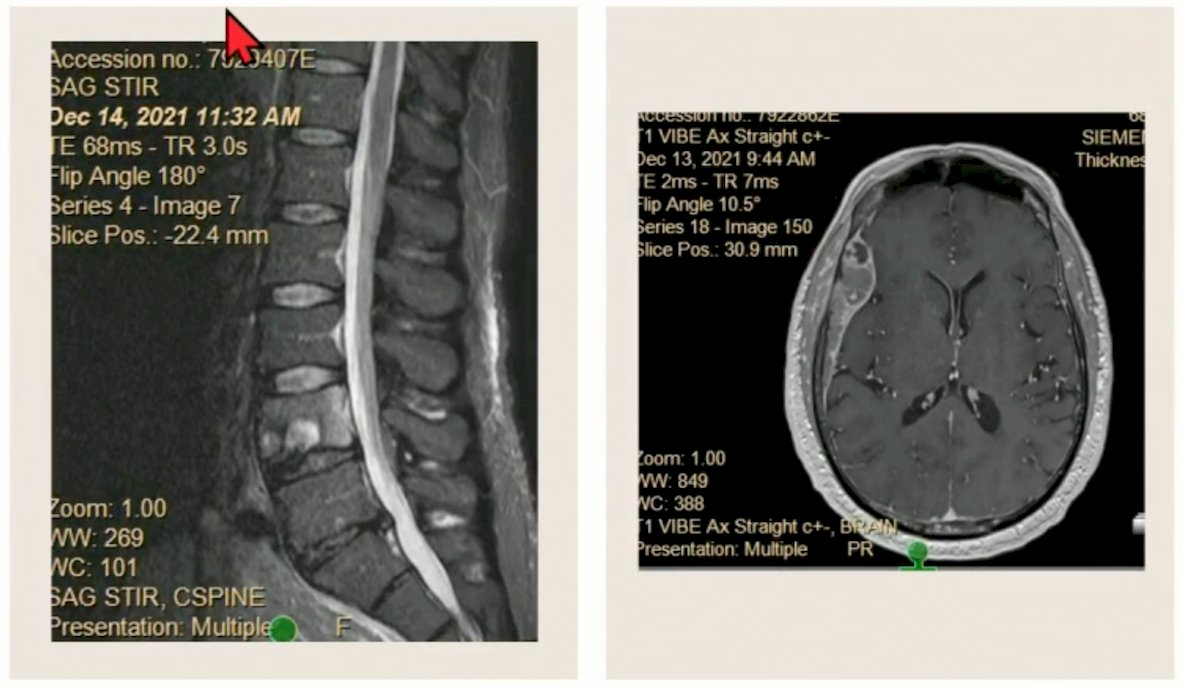
In December 2021 (PSA 30.73 ng/mL), his calvarial metastasis was biopsied, which demonstrated prostate cancer positive for MSI-H and a tumor mutational burden > 50 mutations/Mb. He subsequently completed 35 Gy of radiotherapy in 5 fractions to the epidural metastasis and 30 Gy in 3 fractions to the L4 metastasis. His PSA decreased to 11.55 ng/mL followed by 4.29 ng/mL at which time he started Keytruda, which eventually drove his PSA down to undetectable in April 2022 (where it remains as of September 2022).
Case 3 was a 61 year old male with low volume mCRPC. In 2010, he was diagnosed with prostate cancer at a PSA of 32.8 ng/mL. He subsequently underwent a radical prostatectomy with pathology significant for Gleason 5 + 4 disease, with positive seminal vesicle invasion, positive surgical margins, and 5/16 lymph nodes positive (pT3bN1). Radiotherapy was deferred as he developed a fistula post-operatively. He then was started on Lupron and in 2015 he had a cystoscopy that demonstrated local recurrence, at which time he received radiotherapy to the prostate bed (40 fractions). In October 2015, he was restarted on Lupron + nilandron after a rising PSA. In April 2018, nilandron was discontinued and he was started on apalutamide, which he continued until January 2021. In January 2021, he completed a palliative course of radiotherapy to the left ischium and in March 2021 he completed a course of Provenge. Dr. Thomas then saw the patient as a consult and a PSMA PET/CT showed multiple tracer avid lymph nodes involving the right common iliac, right external iliac, and the right inguinal lymph nodes, as well as a small presacral nodule compatible with metastatic disease. Additionally, there was a tracer avid osseous lesion involving the left L2 vertebral body:
The patient then had SBRT to all sties of PSMA-avid disease in January 2022, including 27 Gy in 3 fractions to L2 and the right common iliac nodes, and 28 Gy in 4 fractions to the right external iliac and right inguinal lymph nodes. His PSA subsequently went from 15.29 ng/mL down to 4.9 ng/mL, however by April 2022, his PSA was again up to 28.37 ng/mL. He completed SBRT to additional lymph node metastasis, however the PSA in June 2022 was up to 164.51 ng/mL and restaging scans showed widespread systemic progression. In July 2022, he completed a 6 cycle course of Xofigo, in August 2022 his PSA was 1201 ng/mL, and in October 2022 he elected to proceed with hospice care.
Case 4 included a 76 year old healthy male diagnosed in 2017 with high risk prostate cancer (Gleason 4 + 4 in 3 cores, with a PSA of 13.30 ng/mL). In February 2018, he underwent a radical prostatectomy, with pathology showing Gleason 4 + 3 disease, positive for seminal vesicle invasion, 0 out of 2 lymph nodes positive, pathologic stage pT3bN0. His post-op PSA nadir was 1.03 ng/mL and he was started on intermittent ADT (August 2018 through February 2022). At this time, a PSMA PET/CT showed hyperavid pre-sacral and para-aortic lymphadenopathy. He was then treated with 28 Gy of radiotherapy in 4 fractions with a boost to 32 Gy in 4 fractions to GTV, with his PSA going up to 2.45 ng/mL in March 2022. In April 2022, he underwent SBRT to all PSMA-avid sites with his PSA increasing to 7.26 ng/mL in September 2022. His PSA continued to increase and he declined further ADT at this point in time. It was recommended that he have radiotherapy to the prostate bed, but he was very hesitant about empiric salvage treatment to the prostate bed and pelvis without an imaging correlation. Dr. Thomas is currently attempting to obtain repeat PSMA PET/CT.
The following points highlight how Dr. Thomas treats PSMA-directed oligometastasis:
- Initial staging: conventional imaging + PSMA PET: PSMA PET is likely superior to conventional imaging, but should not yet completely replace it
- Re-staging: conventional imaging + PSMA PET: treated lesions may remain PSMA PET avid for months after treatment
- Hormone-therapy sensitive patients de novo oligometastatic: Hormone therapy + locoregional radiotherapy + metastasis directed therapy. The goal is long-term biochemical control, it not a cure.
- Oligometastatic recurrent castrate-sensitive (ADT naïve): metastasis directed therapy, with consideration of prostate bed treatment if s/p radical prostatectomy. The goal is ADT-free survival
- Oligometastatic recurrent castrate-resistant: metastasis directed therapy + maintenance of current systemic therapy. The goal is assisting biochemical control and obtaining maximum mileage from current systemic regimen without needing to switch to next line of therapy
- No stringent cutoff for number of oligometastasis: this is still an evolving constraint and prospective trials continue to inform cutoffs
- Include the gland in radiotherapy planning if present, and if untreated
Dr. Thomas cautions about potential prostate cancer mimics on PSMA PET/CT scans. This may include physiologic (ie. celiac, cervical, and sacral ganglia) or pathologic (Paget’s disease, fractures, desmoid tumor, nerve sheath tumors, etc). Finally, there are two important ongoing clinical trials. First, INDICATE is a phase III study of local or systemic therapy intensification directed by PET in prostate cancer patients with post-prostatectomy biochemical recurrence. The primary objectives of this trial are (i) to evaluate PFS for addition of enhanced systemic therapy (apalutamide) to standard of care for patients without PET evidence of extra-pelvic metastases, and (ii) to evaluate PFS for addition of metastasis directed radiotherapy to apalutamide and standard of care for patients with PET evidence of extra-pelvic metastases. Second, the NRG-GU011 PROMETHEAN trial is testing the addition of relugolix to the usual radiation therapy for advanced stage prostate cancer. This trial will include men post-prostatectomy or radiotherapy recurrence with <= 5 oligometastasis. The primary objective is to evaluate PFS for SBRT to all sites versus SBRT + 6 months of relugolix.
Dr. Thomas concluded his presentation discussing when occult metastases become oligometastatic disease with PSMA PET staging with the following take home messages:
- More data is needed, especially prostate centric data, and specifically in the de novo oligometastatic setting
- Until data are more mature, multi-disciplinary discussions should be held for non-straightforward cases
- Oligo- vs poly-metastatic disease may sometimes be difficult to distinguish, even with PSMA PET/CT, thus there may be a role for quantitative ctDNA biomarkers
- PSMA PET/CT directed total metastatic ablation will likely be shown a reasonable treatment for properly selected oligometastatic patients, with an unequivocal PFS benefit in most and ~20% potentially achieving biochemical no evidence of disease status
Presented by: Evan M. Thomas, MD, PhD, Ohio State University, Columbus, OH
References:
- Fossati N, Giannarini G, Joniau S, et al. Newly diagnosed oligometastatic prostate cancer: Current controversies and future developments. Eur Urol Oncol. 2022;5:587-600.
- Glicksman RM, Metser U, Vines D, et al. Curative-intent metastasis-directed therapies for molecularly-defined oligorecurrent prosate cancer: A prospective phase II trial testing the oligometastasis hypothesis. Eur Urol. 2021 Sep;80(3):374-382.