(UroToday.com) The 2022 ASTRO annual meeting featured a session on considerations for treatment of PSMA-staged high-risk patients, including a presentation by Dr. Jeremy de Leon discussing PSMA PET staging for high-risk patients. Dr. de Leon notes that PSMA is a type II transmembrane glycoprotein overexpressed in more than 90% of prostate epithelial cells. Furthermore, many different tracers are available, including [68Ga]-PSMA-11 and [18F]-DCFPyL-PSMA, with [68Ga]-PSMA-11 being the first tracer available in 2012. PSMA is important in primary staging with regards to guiding treatment intent, treatment volume in the prostate +/- pelvis, and systemic therapy. Furthermore, PSMA for primary staging is now approved by the NCCN guidelines.
Published in 2020, the proPSMA study was a multi-center, two-arm randomized controlled trial of men with histologically confirmed prostate cancer who were being considered for curative intent radical prostatectomy or radiotherapy.1 To be eligible for inclusion, men must have had at least one high-risk factor including PSA ≥ 20 ng/mL, ISUP grade group 3-5, or clinical stage T3 or greater. Following enrollment, patients were randomly assigned in a 1:1 ratio to either conventional imaging consisting of bone scan and CT or 68Ga-PSMA-11 PET/CT. In patients who had fewer than three unequivocal sites of metastasis, cross-over imaging for confirmation was performed within 14 days. Confirmatory testing following imaging was performed at the discretion of the treating physician and included biopsy confirmation.
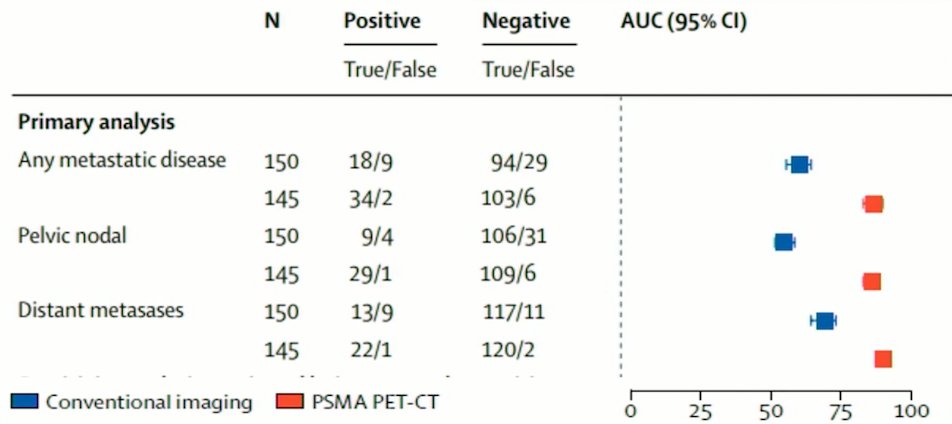
The primary study outcome was the accuracy of first-line diagnostic imaging for identifying either pelvic nodal or distant metastatic disease. Accuracy was reported using the AUC of the ROC curve. The reference standard was a composite panel of histopathology, imaging, and biochemistry at 6-month follow-up. Between 2017 and 2018, 302 patients were randomized to either conventional imaging (n = 152) or 68Ga-PSMA-11 PET/CT (n = 150). As planned, the study cohort exhibited high-risk disease features: 293 (97.0%) men had ISUP grade 3 or higher, 65 (21.5%) had PSA 20 ng/mL or higher, and 82 (27.2%) had clinical stage T3 or T4 disease. Of note, 96% (n = 146) of men assigned to conventional imaging underwent subsequent second line PSMA PET-CT. Of 295 (98%) men with follow-up, 87 (30%) had pelvic nodal or distant metastatic disease. With regards to the primary outcome, PSMA PET/CT had a 27% absolute greater AUC for accuracy compared to conventional imaging (95% CI for difference: 23 – 31%): 92% (95% CI: 88 – 95%) vs. 65% (95% CI: 60 – 69%). Conventional imaging had both a lower sensitivity (38% vs. 85%) and specificity (91% vs. 98%). Subgroup analyses by site of metastasis demonstrated the superiority of PSMA PET/CT for pelvic nodal (AUC: 91% versus 59%) and distant metastases (AUC: 95% versus 74%):
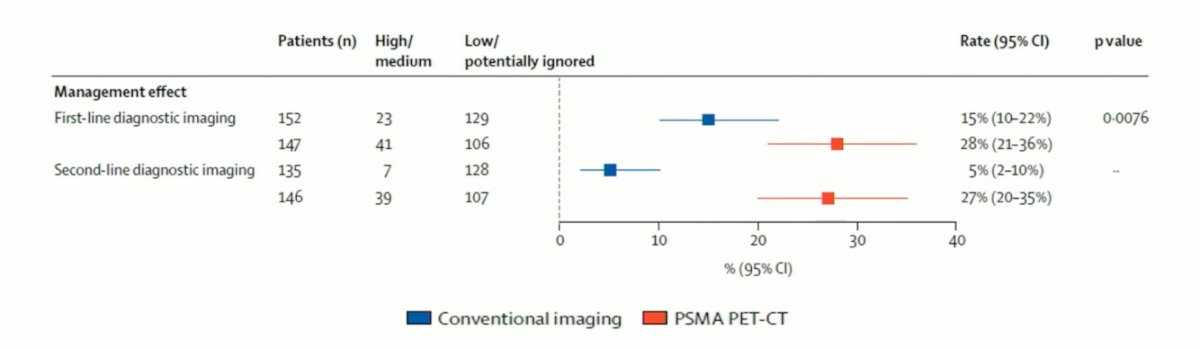
Imaging findings led to changes in management (treatment intent, modality, or delivery) in 28% of men in the PSMA PET/CT arm versus 15% of men in the conventional imaging arm. Following first-line PSMA PET/CT, 20 (14%) of 148 patients were directed from curative to palliative-intent treatment, 11 (7%) had a change in radiotherapy technique, and 11 (7%) in surgical technique:
Hope and colleagues previously published a meta-analysis of 68Ga-PSMA-11 PET accuracy for the detection of prostate cancer validated by histopathology.2 This study included 5 studies of intermediate and high-risk prostate cancer, assessing pathology at the time of surgery. In this analysis, 68Ga-PSMA-11 PET had a sensitivity of 74% and a sensitivity of 96%.
The PRIMARY study was published in 2021 and aimed to determine whether the combination of PSMA + MRI was superior to MRI in diagnostic performance for detecting clinically significant prostate cancer.3 Among 291 men that underwent MRI, pelvic-only PSMA, and systematic ± targeted biopsy, 56% (n = 162) had clinically significant prostate cancer, 67% had PI-RADS 3-5, 73% were PSMA positive, and 81% were combined PSMA + MRI positive. Combined PSMA + MRI improved NPV compared with MRI alone (91% vs 72%, test ratio = 1.27 [1.11-1.39], p < 0.001). Sensitivity also improved (97% vs 83%, p < 0.001), however specificity was reduced (40% vs 53%, p = 0.011). Five clinically significant prostate cancer cases were missed with PSMA + MRI (four ISUP 2 and one ISUP 3).
Roberts and colleagues assessed the importance of primary tumor PSMA intensity as a prognostic biomarker for biochemical recurrence-free survival following radical prostatectomy.4 Among 848 men who underwent all of multiparametric MRI (mpMRI), transperineal prostate biopsy, and 68Ga-PSMA PET/CT prior to radical prostatectomy, the estimated 3-year biochemical recurrence free survival was 79% and the 5-year biochemical recurrence free survival was 70%. Increasing PSMA intensity was associated with less favorable biochemical recurrence free survival overall (log rank p < 0.001), and within subgroups of Gleason score category (log rank p < 0.03). As follows is biochemical recurrence free survival after radical prostatectomy according to Kaplan-Meier survival estimate by quartiles of SUVmax per biopsy grade group:
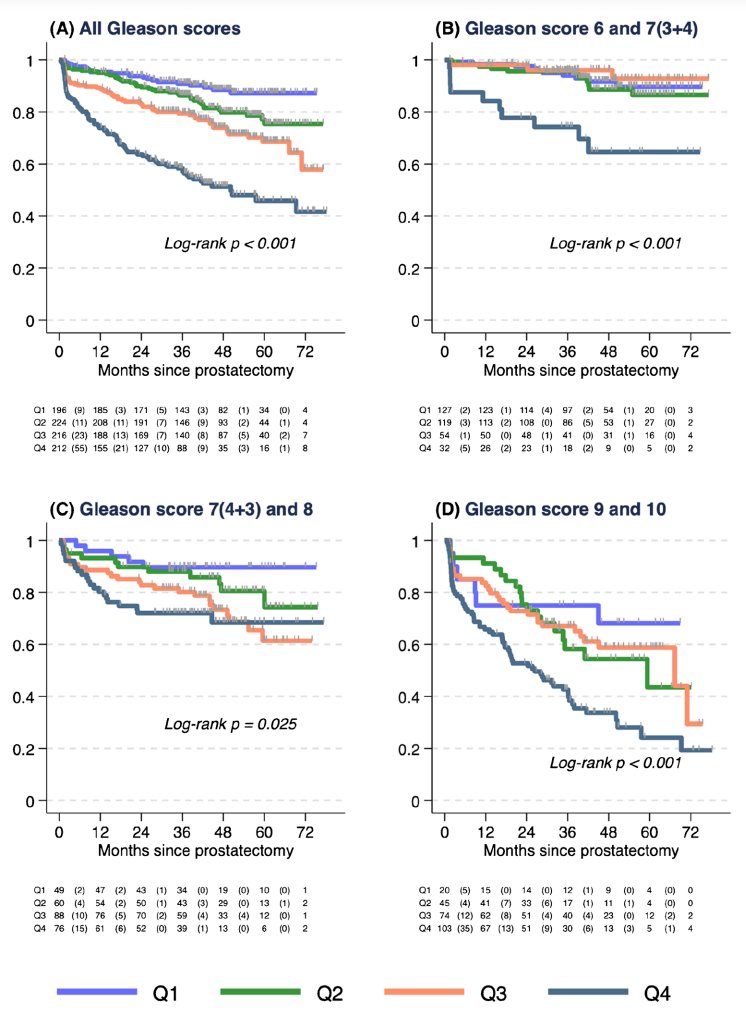
PSMA intensity was significantly associated with shorter time to biochemical recurrence, after adjusting for pre-operative (HR per 5-unit SUVmax increase = 1.15) and post-operative (HR per 5-unit SUVmax increase = 1.10) parameters.
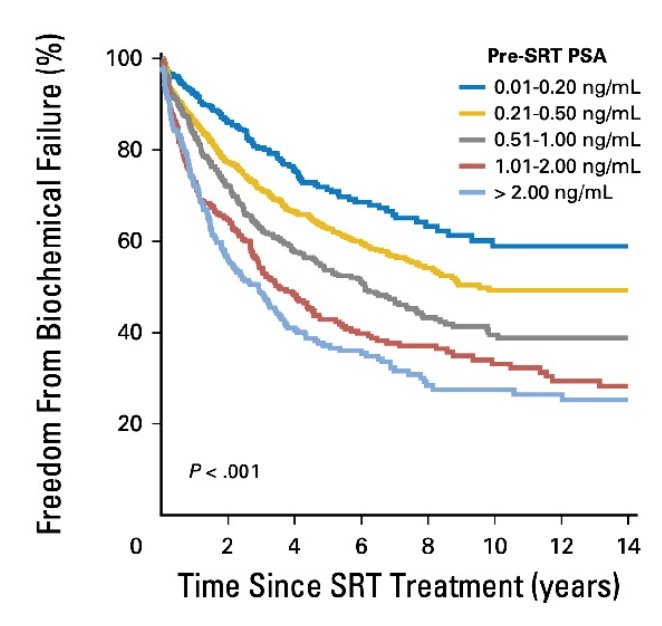
Dr. De Leon then discussed the importance of PSMA in the post-prostatectomy setting. PSMA in this setting is important for guiding prostate bed volume for radiotherapy +/- pelvis +/- dose escalation and systemic therapy. As such, PSMA imaging is included in most major guidelines as the recommended modality of choice. PSMA is important in the post prostatectomy setting given that we must decide if we are going to treat patients in the early or later salvage radiotherapy setting. Data from Tendulkar et al.5 suggest that higher pre-salvage radiotherapy PSAs lead to worse freedom from biochemical failure:
PSMA PET CT is also important for detecting nodal disease in the setting of biochemical recurrence. A systematic review and meta-analysis by Kimura et al.6 assessed 14 studies comprising 462 patients, noting that the positive predictive value of PSMA-PET before salvage lymph node metastasis on a patient-based analysis ranged between 0.70 and 0.93. The pooled sensitivity using lesion-based and field-based analyses were 0.84 (95% CI: 0.61-0.95) and 0.82 (95% CI: 0.72-0.89), respectively. The pooled specificity using lesion-based and field-based analyses were 0.97 (95% CI: 0.95-0.99) and 0.95 (95% CI: 0.70-0.99), respectively. Fendler et al. published the results of a single-arm, multicenter trial conducted at UCLA and UCSF that included 635 patients with biochemical recurrence following prostatectomy (41%), radiation therapy (27%), or both (32%).7 Biochemical recurrence was defined as a PSA of ≥ 0.2 ng/mL 6 weeks post-prostatectomy or a PSA rise ≥ 2 ng/ml above nadir following radiation therapy. The composite reference standard was the combination of (in descending priority) histopathologic analysis, imaging, and PSA follow-up after local/focal therapy. Among these patients, 42% had composite follow-up at a median duration of 9 months, and 18% had histopathologic follow-up. Median PSA at study entry was 2.1 ng/ml (range: 0.1 – 1,154.0). PET detection rates varied significantly by the PSA range:
- <0.5 ng/ml: 38%
- 0.5 – 0.99 ng/ml: 57%
- 1.0 – 1.99 ng/ml: 84%
- 2.0 – 5.0 ng/ml: 86%
- ≥5.0 ng/ml: 97%
Furthermore, 40% of patients had extrapelvic detected disease:
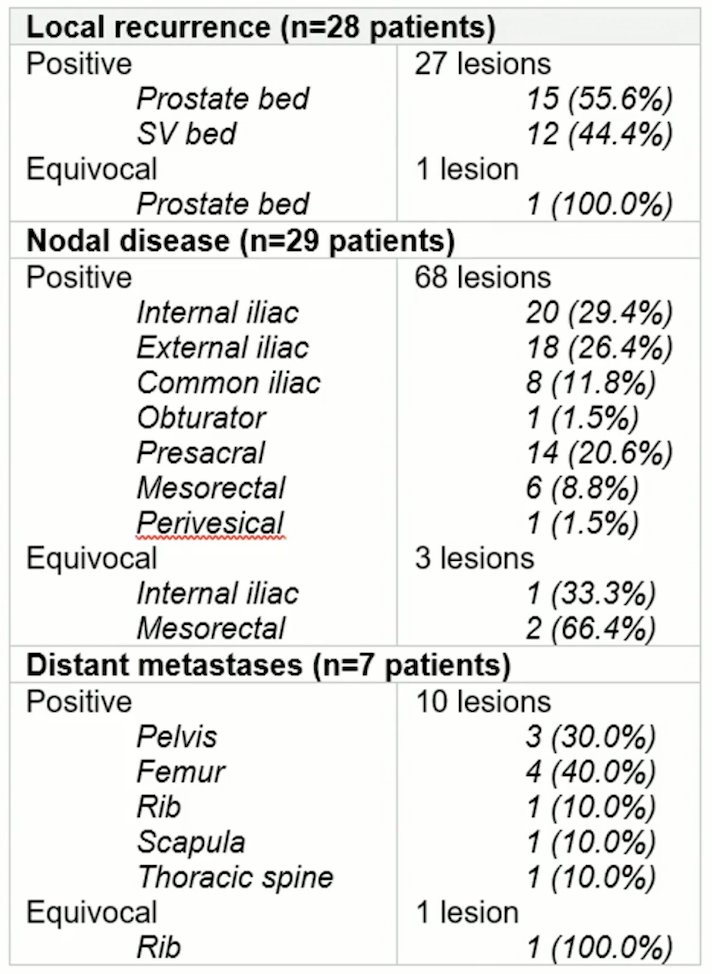
The IMPPORT trial was designed to assess patterns of disease detection, predictive factors and safety using [18F]DCFPyL PET/CT versus diagnostic CT in patients being considered for salvage radiotherapy with biochemical recurrence post prostatectomy.8 This included 100 patients with detectable PSA post prostatectomy (PSA 0.2-2.0 ng/mL) and referred for salvage radiotherapy from August 2018 to July 2020. All patients underwent a PSMA PET/CT using the [18F]DCFPyL tracer and a diagnostic CT. Of 100 patients recruited, 98 were suitable for analysis with a median PSA of 0.32 ng/mL. [18F]DCFPyL PET/CT was positive 46.4% and equivocal 5.2%, compared to 15.5% positivity for diagnostic CT. Local recurrence was detected on [18F]DCFPyL PET/CT in 28.5%, nodal disease in 27.5% and bony metastases in 6.1% of patients. Characteristics of recurrence were as follows:
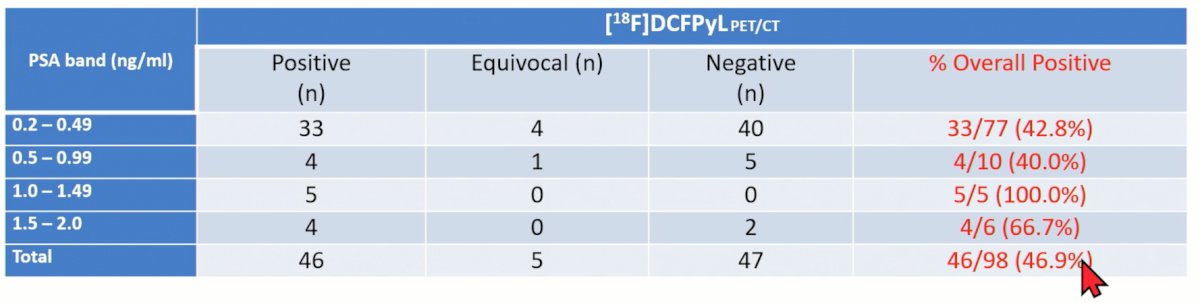
Both ISUP grade group (p < 0.001) and pre-scan PSA (p = 0.029) were significant predictors of [18F]DCFPyL PET/CT positivity, and logistic regression generated probabilities combining the two showed improved prediction rates. The positivity detection rate stratified by PSA level are as follows:
To guide treatment decision making and planning in the biochemical recurrent disease space, the EMPIRE-1 trial sought to evaluate whether 18F-fluciclovine improves cancer control compared to conventional imaging (bone scan + CT/MRI) alone for salvage post-prostatectomy radiotherapy.9 This was a single center, open label, phase 2/3 trial of post-prostatectomy patients with a detectable post-operative PSA and negative conventional imaging. These patients were randomly assigned in a 1:1 ratio to radiotherapy directed by conventional imaging alone or to conventional imaging plus 18F-fluciclovine-PET/CT. In the 18F-fluciclovine-PET/CT group, radiotherapy decisions were rigidly determined by PET findings, which were also used for target delineation. The primary study outcome was 3-year event-free survival, with events defined as biochemical or clinical recurrence or progression, or initiation of systemic therapy. Between 2012 and 2019, this trial recruited 165 patients, with a median follow-up of 3.52 years. The 3-year event-free survival was significantly improved in the 18F-fluciclovine arm: 75.5% versus 63.0% (difference 12.5; 95% CI: 4.3–20.8; p = 0.0028):

This was confirmed on adjust analysis (HR: 2.04, 95% CI: 1.06 – 3.93, p = 0.0327).
Dr. de Leon concluded his presentation discussing PSMA PET staging for high-risk patients by highlighting what he does in the primary setting and post-prostatectomy setting:
- Primary setting: PSMA PET/CT for ISUP Grade 3-5 disease, and high risk/very high risk disease. +/- negative conventional imaging
- Post-prostatectomy setting: PSMA PET/CT for post-prostatectomy PSA >= 0.2 ng/mL
Presented by: Jeremy de Leon, BSc, M.B.B.S (Honours), FRANZCR, Radiation Oncologist, Genesis Care, Darlinghurst, Australia
References:
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.
- Hope TA, Goodman JZ, Allen IE, et al. Metanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology. J Nucl Med 2019;60(6):786-793.
- Emmett L, Butaeu J, Papa N, et al. The Additive Diagnostic Value of Prostate-specific Membrane Antigen Positron Emission Tomography Computed Tomography to Multiparametric Magnetic Resonance Imaging Triage in the Diagnosis of Prostate Cancer (PRIMARY): A Prospective Multicentre Study. Eur Urol. 2021 Dec;80(6):682-689.
- Roberts MJ, Morton A, Papa N, et al. Primary tumour PSMA intensity is an independent prognostic biomarker for biochemical recurrence-free survival following radical prostatectomy. Eur J Nucl Med Mol Imag 2022;49:3289-3294.
- Tendulkar RD, Agrawal S, Gao T, et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J Clin Oncol. 2016 Oct 20;34(30):3648-3654.
- Kimura S, Abufaraj M, Janisch F, et al. Performance of [68Ga] Ga-PSMA 11 PET for detecting prostate cancer in the lymph nodes before salvage lymph node dissection: A systematic review and meta-analysis. Prostate Cancer and Prostatic Dis 2020;23:1-10.
- Fendler WP, Calais J, Eiber M, et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer. JAMA Oncol. 2019; 5(6):856-63.
- Koschel S, Taubman K, Sutherland T, et al. Patterns of disease detection using [18F]DCFPyL PET/CT imaging in patients with detectable PSA post-prostatectomy being considered for salvage radiotherapy: A prospective trial. Eur J Nucl Med Mol Imag. 2021 Oct;48(11):3712-3722.
- Jani AB, Schreibmann E, Goyal S, et al. 18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): A single centre, open-label, phase 2/3 randomized controlled trial. Lancet. 2021 May 22;397(10288):1895-1904.