(UroToday.com) The 2022 ASTRO annual meeting featured a Presidential Symposium session on artificial intelligence opportunities in today’s patient’s journey, including a presentation by Dr. Alejandro Berlin discussing clinical integration of machine learning for curative-intent radiation treatment of patients with prostate cancer. Dr. Berlin notes that the typical radiation oncology treatment planning includes analyzing imaging contouring radiation beam therapy planning optimization dosing. However, artificial intelligence/machine learning has the opportunity to create a new paradigm:

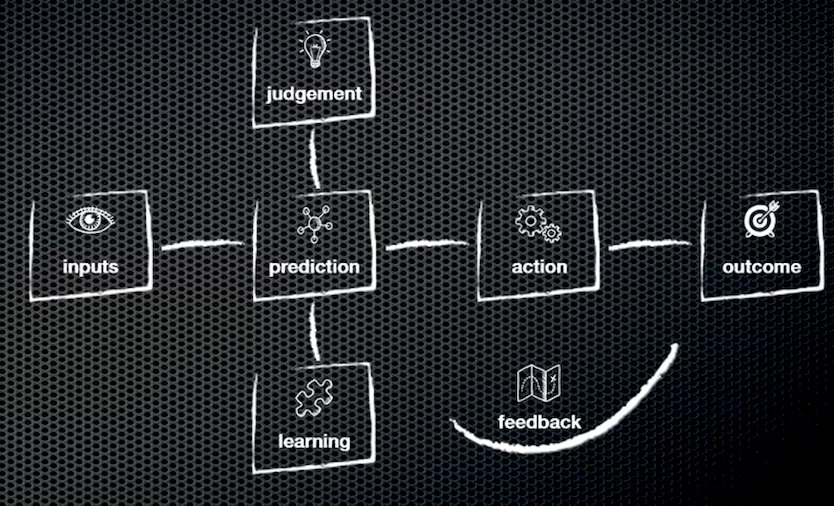
The technology adoption life cycle typically includes a chasm between the early adopters (the visionaries) and the early majority (the pragmatists). The goal in these situations, especially as pertaining to artificial intelligence/machine learning, is to narrow this chasm. A simple view of artificial intelligence/machine learning is that information inputs lead to predictions, however, the human view of artificial intelligence/machine learning is more complex and is associated with a number of decisions and tasks:
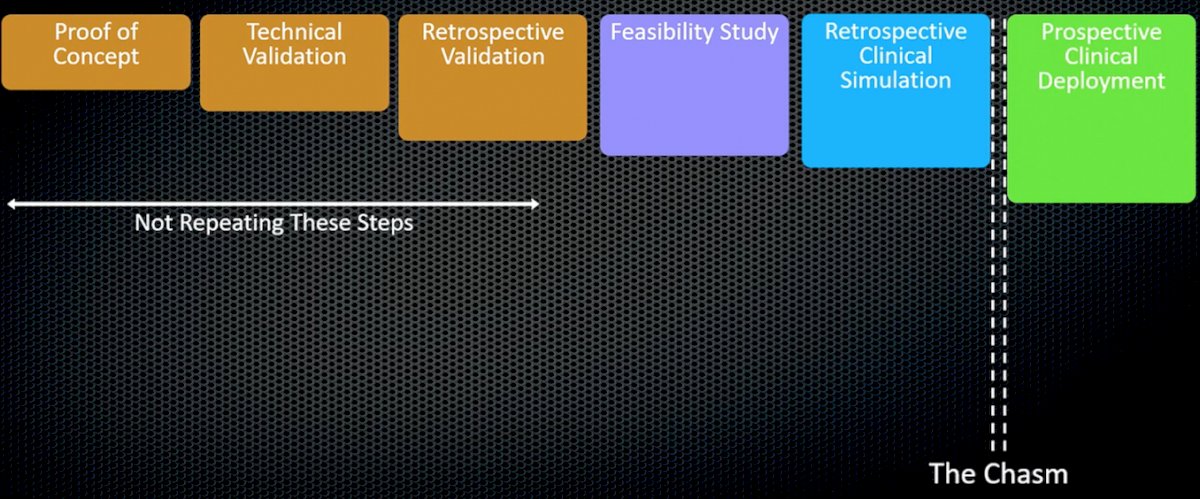
Dr. Berlin notes that the clinical validation framework for optimizing radiation oncology treatment planning is made up of several parts. First, in his opinion, the proof of concept, technical validation, and retrospective validation does not need to be repeated. However, a feasibility study and retrospective clinical simulation are necessary in order to be able to bridge the chasm for prospective clinical deployment:
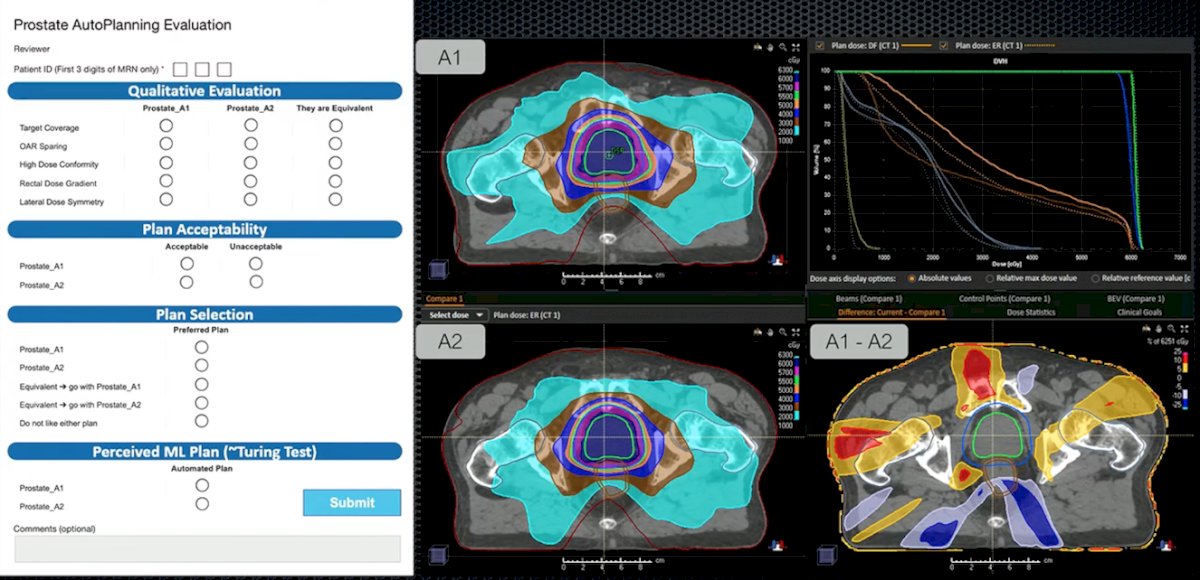
In the Princess Margaret Cancer Center feasibility study and clinical validation framework, 3 reviewers for 17 patients (51 plans) assessed human and artificial intelligence/machine learning plans. There was consistent evaluation throughout, including a prostate auto-planning evaluation:
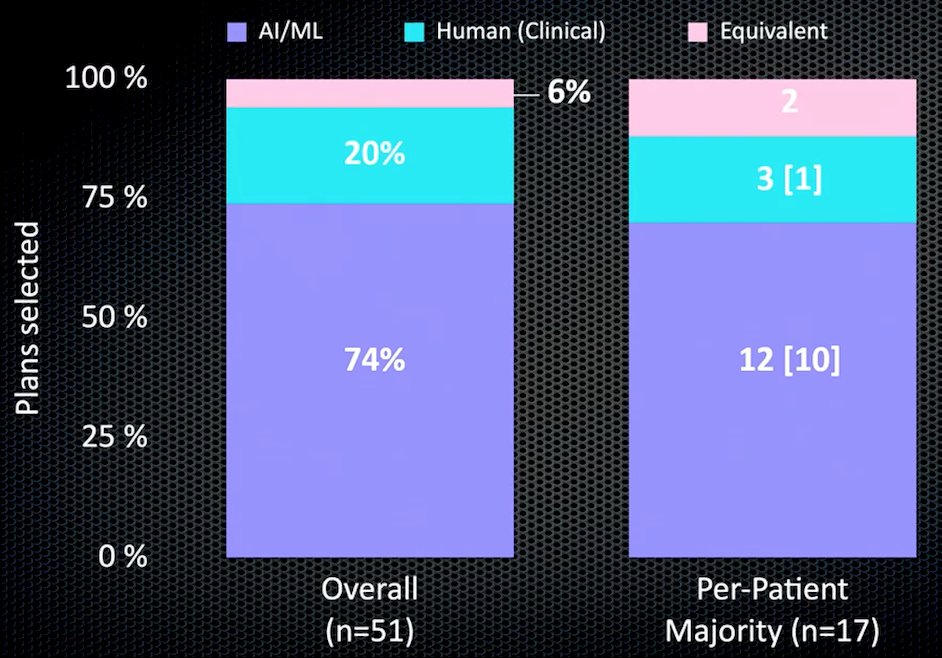
The results of the feasibility study of artificial intelligence/machine learning versus human plans selected are as follows:
Subsequently, for the retrospective clinical validation, there were 7 radiation oncologists for 50 patients, assessing human and artificial intelligence/machine learning plans. Furthermore, in the prospective clinical deployment phase, there were 9 radiation oncologists for 50 patients, again assessing human and artificial intelligence/machine learning plans. What they found was that in the shift from code to the clinic, artificial intelligence/machine learning performance was unaltered (~90% acceptability) and human judgment changes (83% -> 61% artificial intelligence/machine learning plans selected):

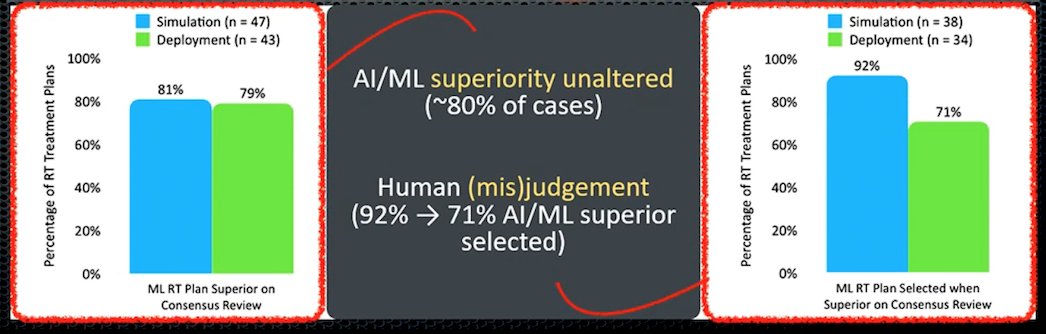
Subsequently, artificial intelligence/machine learning superiority was unaltered (~80% of cases), and human (mis) judgment was still present (92% -> 71% artificial intelligence/machine learning superior selected):
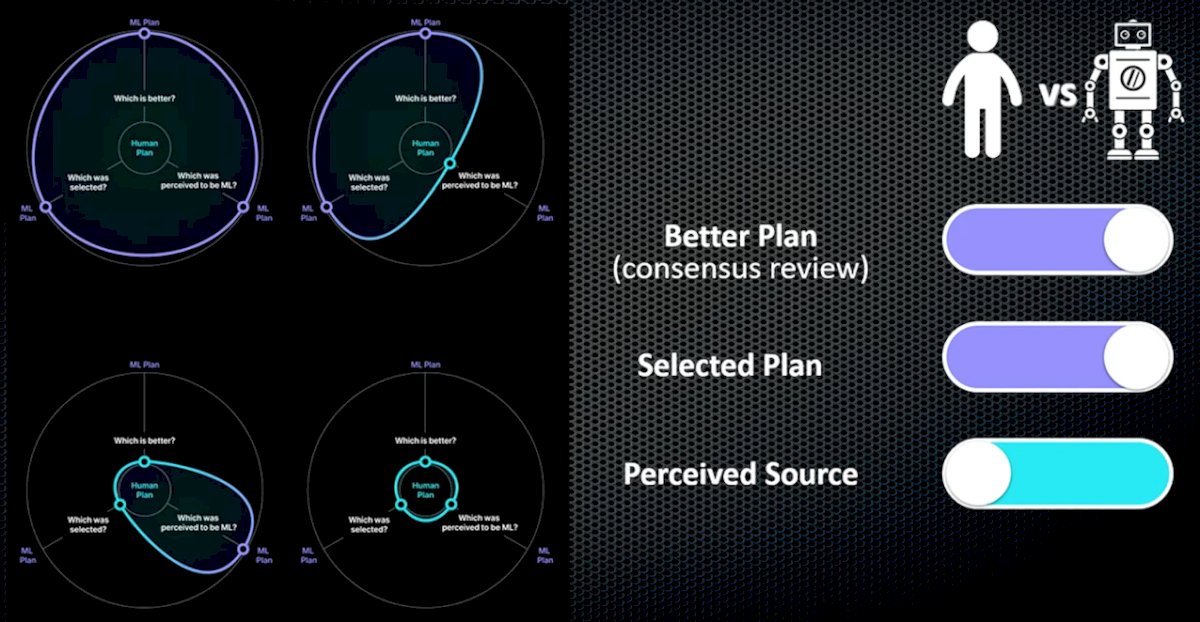
Dr. Berlin emphasized that perhaps there is a radiation oncologist preference (bias?) toward artificial intelligence/machine learning or human planning. The better plan and the selected plan were artificial intelligence/machine learning, however, the perceived source of the plan was from humans:
The objective gains from an artificial intelligence/machine learning plan are several-fold:
- Collapsing the planning time: ~60 minutes -> ~10 minutes
- Overall process median time savings: 71 hours (61% improvement)
- This may enable the shifting of resources and allow new workflow paradigms
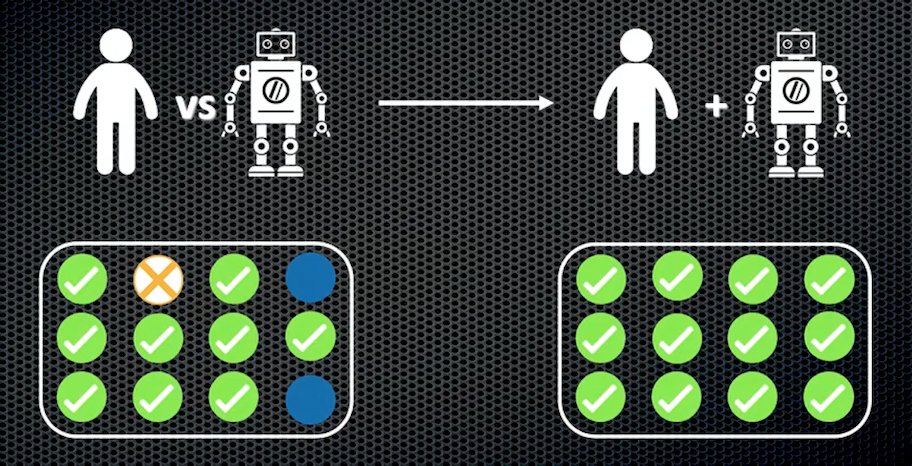
What happened next at Dr. Berlin’s institution of the Princess Margaret Cancer Centre, is that more than 100 patients have had two artificial intelligence/machine learning plans created, of which 80% were selected and only ~20% were human-generated treatment plans. Thus, this has become a new standard of care at his institution. Indeed, Dr. Berlin notes that an apocalyptic view is non-realistic, and that we need both artificial intelligence/machine learning and humans in a decision-making loop:
Dr. Berlin’s group is now working on bringing it all together with simulation, segmentation, treatment planning, quality assurance, and treatment delivery. The ultimate goal is moving from the traditional platform of diagnostic imaging -> consultation simulation -> segmentation -> planning -> quality assurance -> delivery of the first fraction of treatment to a same-day, one-stop shop incorporating all of these steps, thus saving time, and resources, and improving the patient experience.
Dr. Berlin concluded his presentation discussing the clinical integration of machine learning for curative-intent radiation treatment of patients with prostate cancer with the following take-home messages:
- Artificial intelligence/machine learning in radiation oncology can lead to automation, with the ability to enhance many processes in the radiation oncology field
- Prediction algorithms are (mostly) predictable, while humans (interacting with machines are not). We need to fully evaluate and understand automation biases
- Humans in the decision loop allows judicious maximization of artificial intelligence/machine learning potential, and promotion of human/machine collaboration
- Radiation oncology is uniquely poised to lead this field
Presented by: Alejandro Berlin, MD, MSc, Princess Margaret Cancer Centre, Toronto, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Radiation Oncology (ASTRO) Annual Hybrid Meeting, San Antonio, TX, Sat, Oct 22 – Wed, Oct 26, 2022.