(UroToday.com) The 2022 ASTRO annual meeting featured an improving prostate cancer survival session, including a presentation by Dr. James Assif discussing conditional survival probabilities in recurrent prostate cancer patients receiving radiation ± antiandrogen therapy. Salvage radiation therapy and androgen-deprivation therapy (ADT) are routinely used in patients with elevated PSA levels after radical prostatectomy. Although overall survival (OS) and biochemical-failure following salvage radiation therapy are useful when counseling patients at the time of treatment, the utility of survival data from time of diagnosis diminishes over time. Conditional survival can provide more relevant estimates, especially given long-term prostate cancer survivorship. The primary aim of this study presented by Dr. Assif and colleagues was to analyze conditional survival estimates for recurrent prostate cancer patients undergoing salvage radiation therapy ± ADT. The secondary objective was to determine if factors prognostic of OS and biochemical-failure at diagnosis remain relevant in survivorship.
This study analyzed data from 760 post-radical prostatectomy patients enrolled in NRG/RTOG 9601 (1998–2003) [1]. Eligible patients included men who had undergone prior radical prostatectomy and had pT2/T3 disease without nodal involvement and detectable PSA levels of 0.2–4.0 ng/mL. Patients were randomly assigned to undergo salvage radiation therapy and receive either 24 months of ADT or placebo:
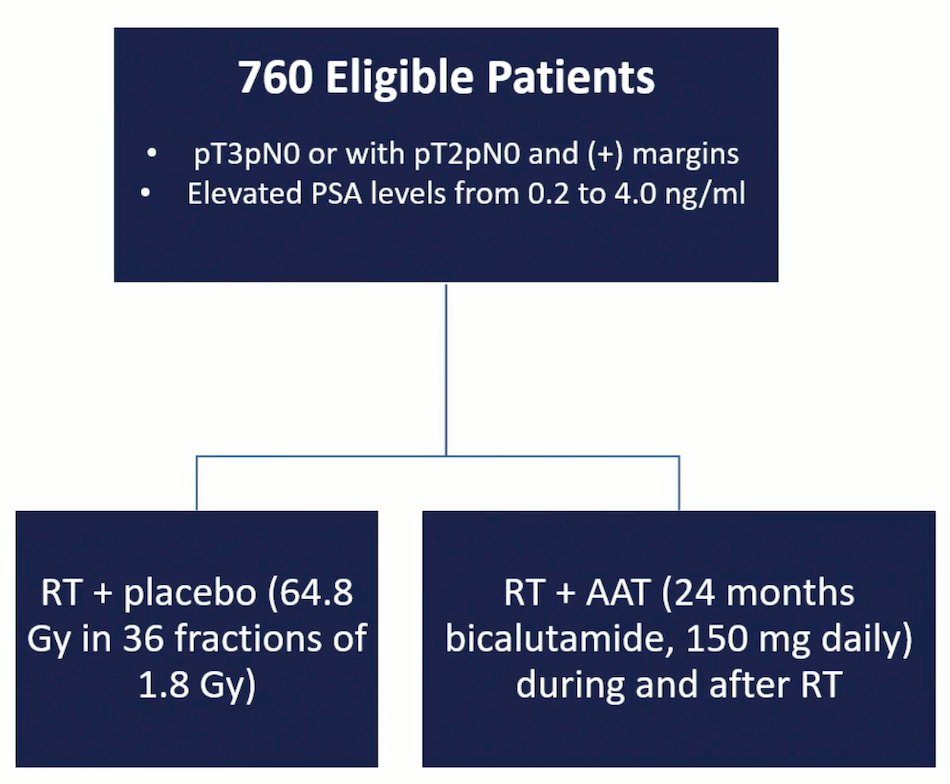
OS was calculated (Kaplan–Meier), cumulative incidence was used to estimate biochemical-failure rates, and prognostic factors associated with OS and biochemical-failure were analyzed by multivariable Cox proportional hazards modeling.
Patients were followed for a median of 13 years. The 5- and 10-y rates of biochemical-failure from diagnosis were 36% and 52%, respectively. For patients who survived 1 (n = 725), 3 (n = 560), 5 (n = 435), 8 (n = 320), and 10 (n = 268) years without biochemical-failure, chances of biochemical-failure at an additional 5 years were 39%, 33%, 26%, 20%, and 20%, respectively:

The 5- and 10-year OS estimates from diagnosis were 93% and 80%, respectively. At 1- (n = 755), 3- (n = 727), 5- (n = 680), 8- (n = 602), and 10-year (n = 543) survivorship, chances of surviving an additional 5 years were 92%, 89%, 86%, 80%, and 72%, respectively:

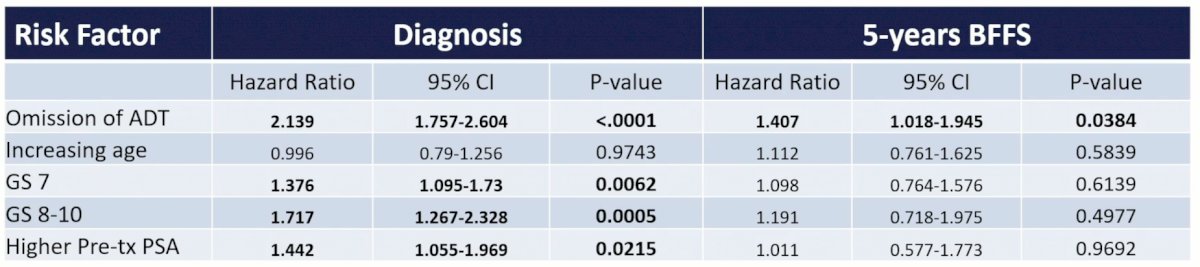
On multivariable analysis at time of salvage radiation therapy, omission of ADT (HR 2.139, p < 0.0001), Gleason score 7 (HR 1.376, p = 0.0062), Gleason score 8–10 (HR 1.717, p = 0.0005), and higher pretreatment PSA (HR 1.442, p = 0.0215), were associated with biochemical-failure. For those who survived 5 years after treatment without failure, only omission of ADT (HR 1.407, p = 0.0384) was prognostic of biochemical-failure:
On multivariable analysis at diagnosis, omission of ADT (HR 1.308, p = 0.0403), increasing age (HR 2.761, p < 0.0001), and Gleason score 8−10 (HR 1.938, p = 0.0005), were associated with all-cause mortality. For those who achieved survivorship at 5 years, only age (HR 2.973, p < 0.0001) and Gleason score 8–10 (HR 1.801, p = 0.0063) were prognostic of mortality on multivariable analysis:

Dr. Assif concluded his presentation discussing conditional survival probabilities in recurrent prostate cancer patients receiving radiation ± antiandrogen therapy with the following concluding points:
- Conditional risk of biochemical-failure for patients treated with salvage radiation therapy remains elevated at levels similar to those at initial treatment for up to 3 years after salvage radiation therapy, after which biochemical-failure rates decrease
- ADT continues to confer a reduced risk for biochemical-failure for long-term survivors
- Age and Gleason score 8-10 are prognostic for mortality
- This data can be used to inform survivorship care planning and highlights the need for continued PSA surveillance after completion of treatment
Presented By: James W. Assif, Department of Radiation Oncology, University of Maryland School of Medicine, Baltimore, MD
Co-Authors: G. S. Alexander2, R. F. Krc2, K. Sun3, J. K. Molitoris4, Z. H. Rana5, P. T. Tran6, S. M. Bentzen3, and M. V. Mishra7; 1Department of Radiation Oncology, University of Maryland School of Medicine, Baltimore, MD, 2Department of Radiation Oncology, University of Maryland Medical Center, Baltimore, MD, 3Division of Biostatistics and Bioinformatics, University of Maryland Greenebaum Cancer Center, and Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, MD, 4University of Maryland School of Medicine, Baltimore, MD, 5Northwell Health, Lake Success, NY, 6Johns Hopkins University, Baltimore, MD, 7Maryland Proton Treatment Center, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Radiation Oncology (ASTRO) Annual Hybrid Meeting, San Antonio, TX, Sat, Oct 22 – Wed, Oct 26, 2022.
References: