(UroToday.com) In a session at the American Society for Radiation Oncology (ASTRO) Annual Congress focused on the care of patients with intermediate and high-risk prostate cancer, Dr. Romero presented on the relationship between androgen deprivation therapy (ADT) duration and external beam radiotherapy (EBRT) with or without brachytherapy boost in high-risk prostate cancer.
To begin, Dr. Romero highlighted that NCCN clinical practice guidelines recommend 18 to 36 months of ADT for patients receiving EBRT for high-risk prostate cancer. This is based on three trials which have shown improved overall survival for patients who received longer (24-36 months) compared to shorter (4-6 months) ADT courses. A further one trial showed improved prostate cancer specific mortality for patients who received 18 months compared to 6 months of ADT while a single trial failed to show a benefit of 36 months compared to 18 months of ADT.
In patients who are receiving brachytherapy boost with EBRT for high-risk disease, NCCN clinical practice guidelines recommend 12 to 36 months of ADT. This is based off a single trial which demonstrated improved progression-free survival. However, no randomized trial has assessed the optimal duration of ADT among patients receiving EBRT + brachytherapy boost.
Despite these recommendations, and the underpinning data showing survival benefits, ADT is widely underutilizing in real world practice, particularly among patients receiving high dose EBRT or EBRT + brachytherapy boost.
Thus, the authors sought to examine specific ADT thresholds that provide benefit in distant metastasis free survival for patients receiving high dose EBRT (defined as 74 Gy or higher) or EBRT + brachytherapy boost. This was first examined among a multi-institutional cohort of patients across 16 tertiary care centers and then among individual patient data from the TROG RADAR trial (which compared 6 vs 18 months of ADT) and the GICOR trial (which compared 4 vs 28 months of ADT).
The authors used multivariable Cox proportional hazards models to evaluate the association between various durations of ADT (<6 months, 6-18 months, and >18 months) and metastasis-free survival and overall survival. These models accounted for covariates including PSA, clinical T stage, Gleason grade group, age at treatment, treatment type, and the interaction between ADT duration and treatment. They further used splines to assess the continuous, non-linear association between ADT duration and metastasis free survival.
Similar analyses were performed using the datasets from RADAR and GICOR, with inverse probability of treatment weighting used for comparisons of MFS and OS between trials.
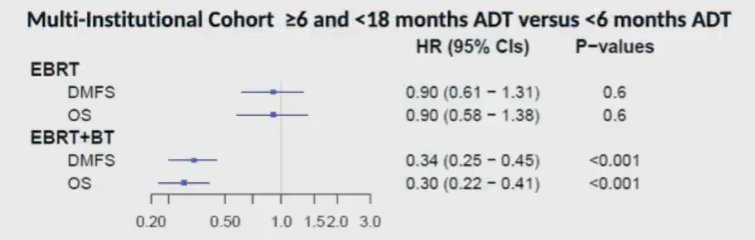
In the initial multi-institutional cohort, the authors found significant benefit of ADT durations 6-18 months, compared to <6 months, among patients who received EBRT + brachytherapy boost (HR 0.34 for MFS and 0.30 for OS) but not among those who received EBRT alone (HR 0.90 for MFS and 0.90 for OS). There was, therefore, a significant interaction between treatment type and the effect of ADT duration (p<0.01).
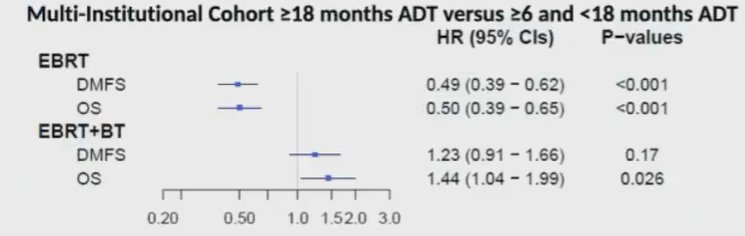
In contrast, when the authors compared >18 months of ADT with 6-18 months of ADT, there was no significant benefit for the additional duration among patients who received EBRT + brachytherapy boost, and actually decreases in overall survival, whereas for patients receiving EBRT without brachytherapy boost, the additional duration of ADT was associated with improved MFS (HR 0.49) and OS (HR 0.50). Again, this analysis demonstrated a significant interaction between treatment type and the effect of ADT duration (p<0.01).
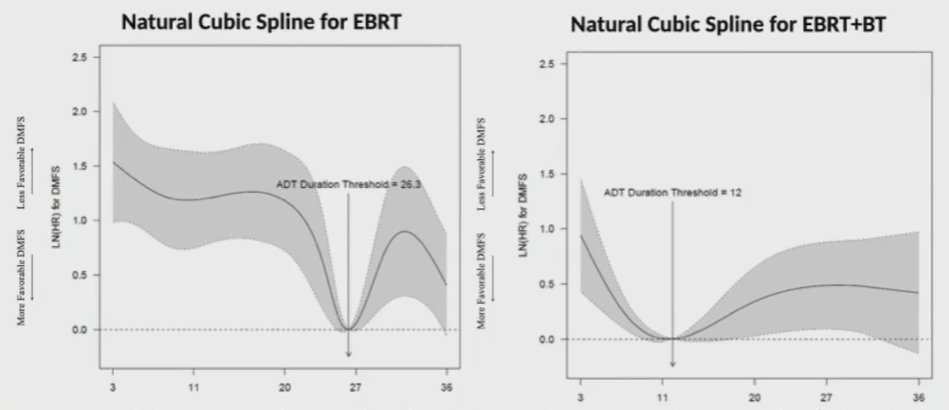
Using cubic splines, the authors determined that the optimal duration for ADT among patients receiving high dose EBRT was 26.3 months (95% CI 25.4 to 36.0 months) whereas for those receiving EBRT + brachytherapy boost it was 12 months (95% CI 4.9 to 36.0 months).
Within the RADAR trial, patients receiving EBRT + brachytherapy boost who received 18 months of ADT, compared to 6 months, had improved MFS (HR 0.56, 95% CI 0.36-0.87) but not OS (HR 0.61, 95% CI 0.36-1.02) though this may represent a tyle II error. In a comparison between GICOR and RADAR, among patients who received high dose EBRT, use of 28 months compared to 18 months of ADT was associated with improvements in both MFS (HR 0.37, 95% CI 0.17-0.80) and OS (HR 0.34, 95% CI 0.12-1.00).
Thus. Dr. Romero concluded that there appears to be an interplay between radiotherapy dose and the optimal duration of ADT in patients with high risk disease. Patients who receive EBRT without brachytherapy boost likely benefit from longer durations of therapy (approximately 26 months) whereas those who receive EBRT + brachytherapy boost may have a shorter optimal duration.
Presented by: Tahmineh Romero, MS, MSSc, BS, Senior Statistician, Division of General Internal Medicine and Health Services Research, UCLA Department of Medicine Statistics Core, UCLAWritten by: Christopher J.D. Wallis, University of Toronto, Twitter: @WallisCJD during the 2021 American Society for Radiation Oncology (ASTRO) Hybrid Annual Meeting, Sat, Oct 23 – Wed, Oct 27, 2021.