(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Oliver Sartor discussing clinical outcomes among patients with metastatic hormone-sensitive prostate cancer (mHSPC) in contemporary real-world US clinical practice. The incidence of mHSPC is increasing in the US, partly due to screening practices.
There has also been a rapid increase in recent years in the number of treatment options that can improve progression-free and overall survival for these patients. However, initial real-world evidence has suggested that uptake of these therapies has been slow. The objective of the current study was to evaluate the clinical outcomes among patients with mHSPC treated in contemporary US clinical practice (2020 to 2025).
This retrospective, observational cohort study used data from PRECISION, a harmonized dataset on advanced prostate cancer in patients in the US treated in a range of clinical settings. Patients aged ≥18 years who were diagnosed with mHSPC during January 1, 2020 – December 22, 2025, and who initiated ≥1 therapy (index date = first line treatment initiation) were included:
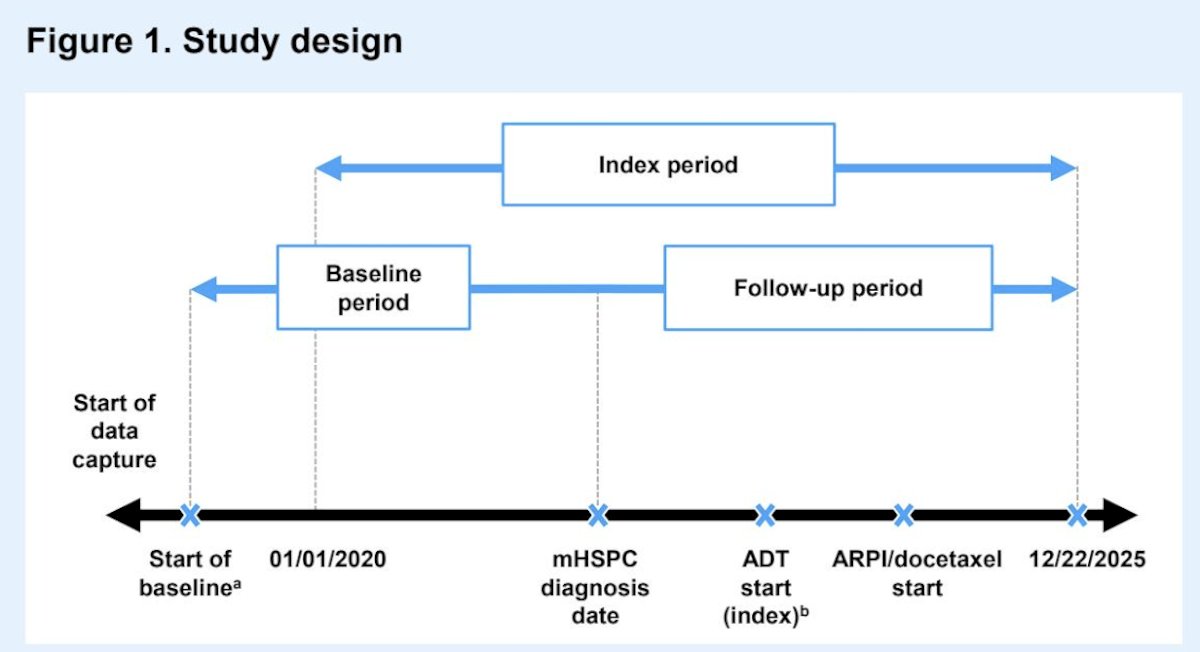
Patient characteristics at mHSPC diagnosis and treatment utilization were evaluated descriptively. Castration resistance-free survival (defined as the time to castration-resistant prostate cancer or death) and overall survival were evaluated from the index using Kaplan–Meier analysis.
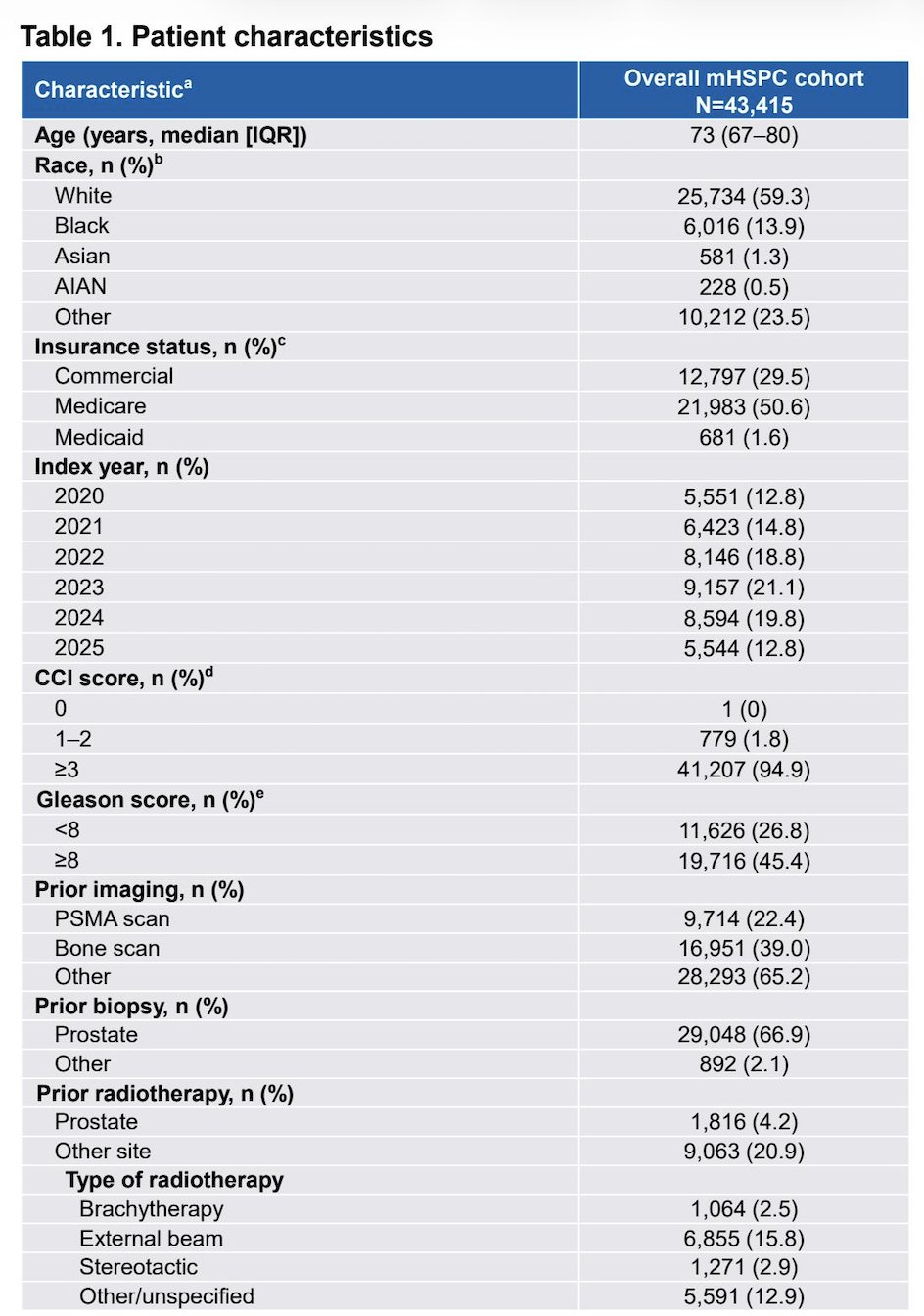
A total of 43,415 patients were included, with a median age of 73 years (IQR 67-80). Overall, 34,882 (80.3%) were treated in community urology, 7,273 (16.8%) in community oncology, and 1,260 (2.9%) in academic oncology centers at index. The median PSA level was 8 ng/mL (IQR 1.4-37.6), with 58.4% of patients having bone metastases, 47.3% lymph node metastases, and 6.5% visceral metastases:
With regards to treatment utilization, 49.2% received ADT monotherapy, 48.3% received doublet therapy (ADT + androgen receptor pathway inhibitor, 46.6%; ADT + docetaxel, 1.7%), and 2.5% received triplet therapy (ADT + androgen receptor pathway inhibitor + docetaxel). Among patients receiving androgen receptor pathway inhibitors as part of doublet therapy, 32.4% had enzalutamide, 29.9% had apalutamide, 26.6% had abiraterone, and 11.1% had darolutamide. Among patients receiving androgen receptor pathway inhibitors as part of triplet therapy, 65.3% had darolutamide, 19.8% had abiraterone, 8.0% had enzalutamide, and 6.8% had apalutamide: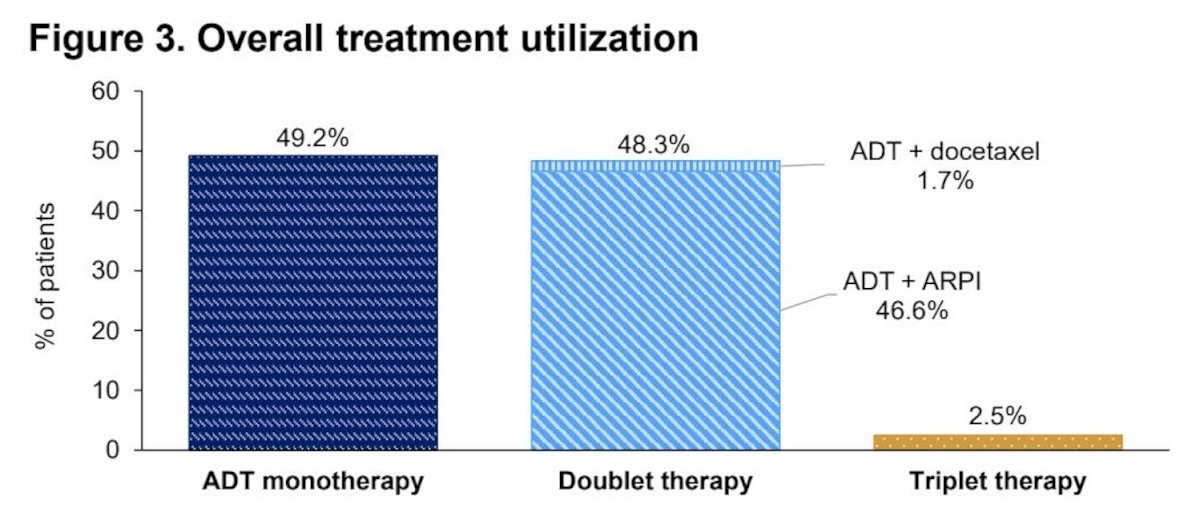
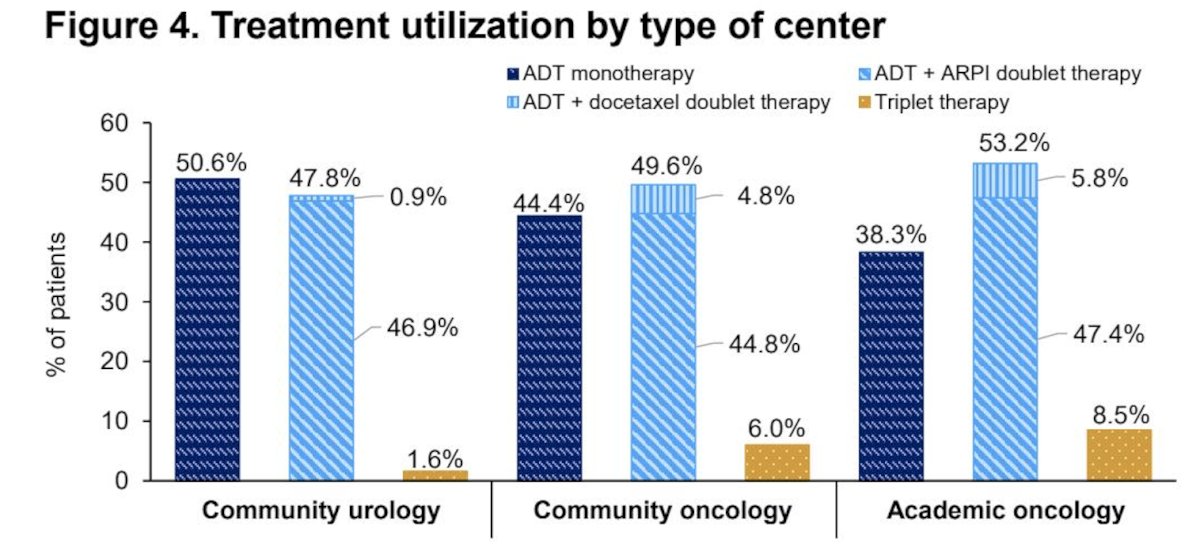
Patients receiving triplet therapy were significantly younger, more likely to be treated in oncology settings and to have synchronous disease, and had higher Gleason scores and higher PSA levels than patients receiving ADT monotherapy or doublet therapy (p<0.001 for all comparisons). Moreover, patient characteristics were more similar between patients receiving ADT monotherapy and doublet therapy. Treatment rates and type by center are shown in the following figure:
Overall, the median castration resistance-free survival was 34.3 (95% CI, 33.3–35.4) months, and the 3-year castration resistance-free survival rate was 49.1% (95% CI, 48.4%–49.7%). Patients receiving doublet or triplet regimens had significantly longer castration resistance-free survival than those receiving ADT monotherapy (p < 0.001):
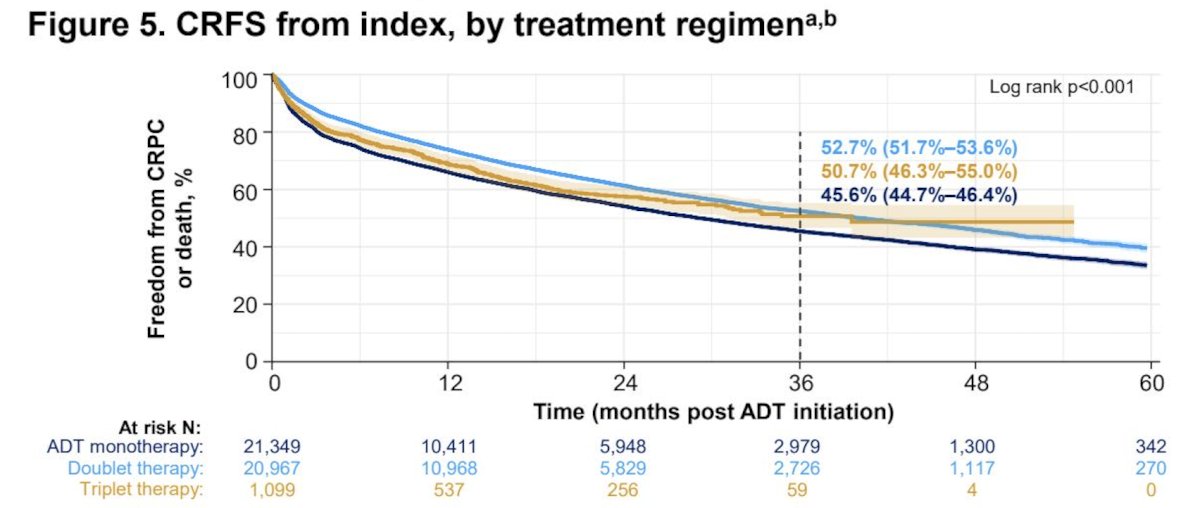
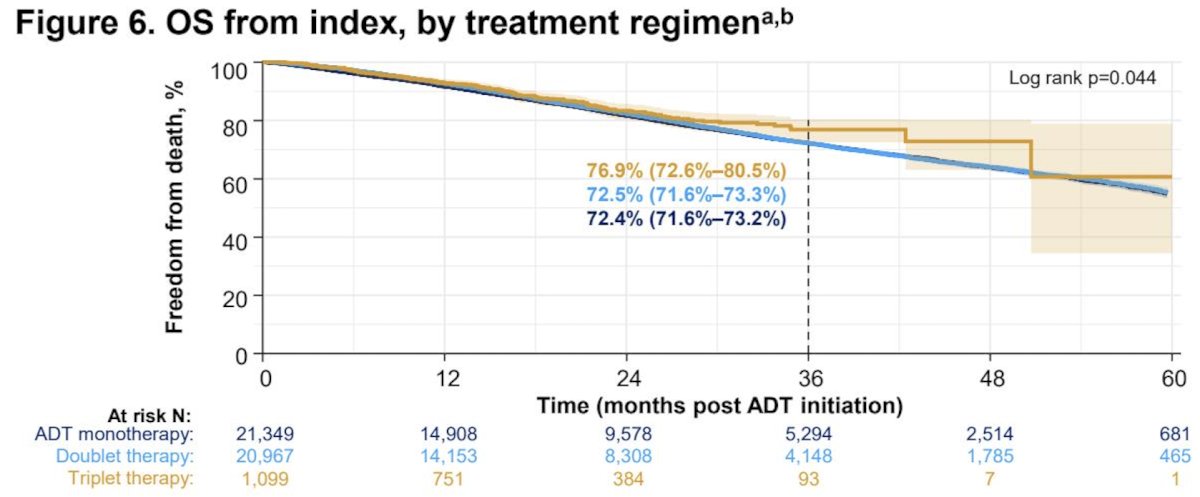
Multivariable analysis confirmed that both doublet (HR 0.7, 95% CI, 0.7–0.7) and triplet therapy (HR 0.7, 95% CI, 0.7–0.8) were associated with a lower risk of progression/mortality than ADT monotherapy. The median overall survival was not reached, and the 3-year overall survival rate was 72.5% (95% CI, 72.0%–73.1%). Overall survival was longest with triplet therapy (p < 0.05), and it appeared to be similar with ADT monotherapy and doublet therapy. However, after adjustment, doublet therapy was associated with a lower risk of mortality than ADT monotherapy (HR 0.9, 95% CI, 0.9–1.0). Given that the median overall survival was not reached in any group, longer follow-up may be required to capture this endpoint fully:
Dr. Sartor concluded his presentation discussing clinical outcomes among patients with mHSPC in contemporary real-world US clinical practice with the following take-home points:
- Although previous studies have suggested that real-world castration resistance-free survival and overall survival appear to be increasing among patients with mHSPC, the median castration resistance-free survival in this study was <3 years
- Treatment patterns differed by type of treatment center; however, nearly half of patients overall received ADT monotherapy, which was associated with shorter castration resistance-free survival and overall survival compared with doublet and/or triplet therapies
- ADT monotherapy was the most common treatment type in community urology centers and the second most common treatment type in community and academic oncology centers
- Triplet therapies were associated with the longest overall survival; only 2.5% of patients in the overall cohort received triplet therapies
- These results support treatment guidelines that recommend the use of combined systemic treatment regimens for improved survival outcomes in mHSPC, confirming the importance of implementing these therapies in real-world practice
Presented by: A. Oliver Sartor, MD, Director, Transformational Prostate Cancer Research Center, East Jefferson General Hospital Cancer Center, Tulane University Cancer Center, New Orleans, LA