(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a discussant presentation by Dr. Bridget Koontz, discussing two abstracts, “Hormone therapy use and duration with post-operative radiotherapy for recurrent prostate cancer: An individual patient data meta-analysis” by Dr. Dr. Amar Kishan, and “Fifteen-year survival analysis from the ASCENDE-RT randomized trial of external beam boost versus brachytherapy boost in localized prostate cancer” by Dr. Scott Tyldesley.
Dr. Koontz started her presentation by highlighting that external beam radiotherapy continues to be a highly effective curative treatment for men with prostate cancer, with reported 10-year metastasis-free survival rates of 74% for post-operative radiation therapy, and 15-year disease-specific survival of 84% for patients with high-risk disease treated with external beam radiotherapy. How can we improve these outcomes further? Perhaps with ADT and dose escalation.
The rationale for androgen ablation with post-operative radiotherapy is that it allows radiosensitization of bad biology prostate cancer and that it treats disease missed by radiotherapy fields (ie, micrometastases). The guidelines for treatment are loose, based on the current evidence, which has been conflicting and underpowered. However, there have been four trials that have investigated this question: GETUG-16,1 RTOG 9601,2 RTOG 0534,3 and RADICALS.4
POSEIDON was a patient-level meta-analysis of post-operative radiotherapy, showing that for overall survival, pre-radiotherapy PSA <0.51 ng/mL did not benefit from concurrent ADT, and that additional analyses are needed for long-term ADT, given that it is currently limited to highly elevated PSAs.
Dr. Koontz’s critique of POSEIDON is that post-operative radiotherapy is highly effect, and that the use of ADT should be focused on those patients with bad biology or high risk of micrometastases. Moreover, she notes:
- Negative PET imaging may ultimately change the PSA cutoff
- For younger patients: Is there a late conversion from metastasis-free survival benefit to overall survival benefit?
- This analysis does not include GU006, which recently reported a benefit of apalutamide for PAM50 luminal B prostate cancer
The impact of POSEIDON is that not all patients need ADT as part of salvage post-operative radiation therapy treatment:

Additionally, we must use common sense with high-risk features; these data are only applicable for PET-negative biochemical recurrence patients, and there is still a developing role for biomarkers.
Dr. Koontz then discussed ASCENDE-RT, noting that the rationale for brachytherapy as a form of dose-escalated radiotherapy is that external beam dose escalation has physical limitations due to adjacent organs and prostate motion considerations. Additionally, brachytherapy can dose escalate 1.5-2x beyond that of external beam radiotherapy.
Previous ASCENDE-RT results include:
- Improved 10 year biochemical control: 85% versus 67%, p < 0.001
- Similar metastasis-free survival: 88% versus 86%, p = 0.56
- No impact on overall survival: 80% versus 75%, p = 0.51
- More frequent genitourinary toxicity: 5 year cumulative grade – 18% versus 5%, p < 0.001
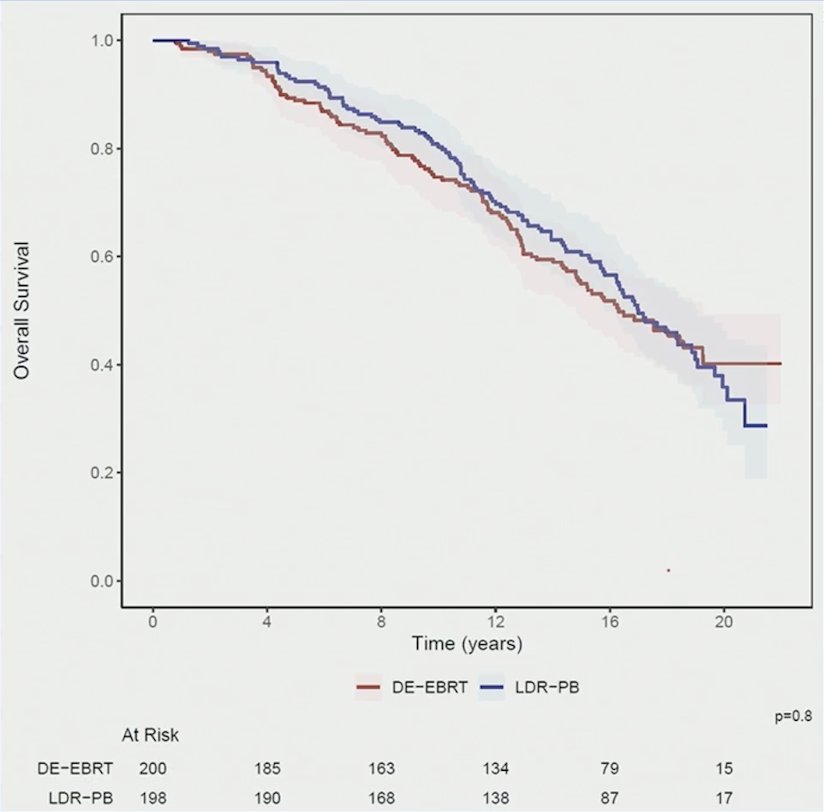
In the presentation of 15 year survival outcomes of ASCENDE-RT, Dr. Koontz notes that there still is no survival benefit at 15 years. Overall survival at 15 years was 55.0% (95% CI 48.4 – 62.4) and 60.9% (95% CI 54.4 – 68.1) for external beam radiotherapy and prostate brachytherapy arms, respectively (HR 1.02, 95% CI 0.78 – 1.33, p = 0.908 on multivariable analysis):
Regarding the context and application of this trial, ASCENDE-RT used standard delivery methods for boost, whereas newer technology offers stereotactic body radiotherapy with better imaging and setup. Notably, brachytherapy offers newer techniques too, including HDR boost, which has similar efficacy but better quality of life scores than LDR boost.
Dr. Koontz concluded her discussant presentation with the following take-home points:
- External beam radiotherapy continues to be a highly effective curative treatment for prostate cancer
- In the PSMA PET post-operative radiation therapy setting, we should minimize the use of ADT to 6 months for PSAs >=0.5 ng/mL
- ADT is reserved for very high PSAs (>= 1.6 ng/ml) and N1 disease
- In intact high-risk prostate cancer, a brachytherapy boost may benefit young men with anticipated longevity, very high-risk localized disease, and reduce their ADT exposure
Presented by: Bridget F. Koontz, MD, FASTRO, Advent Health Cancer Institute, Orlando, FL
References:
- Carrie C, Hasbini A, de Laroche G, et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): A randomized, multicentre, open-label phase 3 trial. Lancet Oncol 2016;17(6):747-756.
- Shipley WU, Seiferheld W, Lukka HR, et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med 2017;376(5):417-428.
- Pollack A, Karrison TG, Balogh AG, et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): An international, multicentre, randomized phase 3 trial. Lancet. 2022 May 14;399(10338):1886-1901.
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomized, controlled phase 3 trial. Lancet 2020;396(10260):1413-1421.