(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Pedro Barata discussing the clinical and cost impact of cabazitaxel versus Lu-PSMA for patients with metastatic castration resistant prostate cancer (mCRPC). The TheraP trial compared cabazitaxel to Lu-PSMA in patients with mCRPC who previously received docetaxel.
In TheraP, Lu-PSMA achieved greater PSA responses than cabazitaxel (66% versus 37%; p = 0.0016), while overall survival was similar (HR 0.97, p = 0.99; difference –0.5 months, p = 0.77).1 Rates of grade 3-4 adverse events were also similar. In this study, Dr. Barata and colleagues aimed to quantify the direct cost differences and assess the clinical outcomes associated with the use of cabazitaxel compared to Lu-PSMA in this population
An Excel-based model was developed to assess clinical and economic outcomes at 6, 12, 18, and 24 months in a US patient population from the US Medicare payer perspective. Efficacy and safety were informed by the TheraP study, supplemented by literature when data were lacking, and confirmed by a genitourinary oncologist. Drug costs were based on Medicare ASP (or RedBook):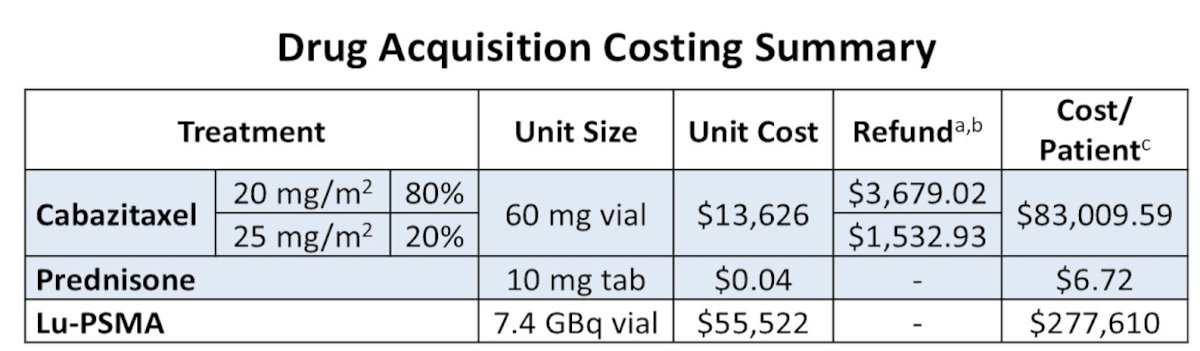
Costs of grade 3-4 adverse events were estimated by weighing inpatient and outpatient management costs. Outcomes included direct costs related to PSMA testing, drug acquisition and administration, supportive care, adverse events, and end-of-life care. Clinical outcomes included the number of patients in overall survival, progression-free survival, PSA progression-free survival, and radiographic progression-free survival. The cost impact was modeled for a cohort of 100 mCRPC patients receiving cabazitaxel or Lu-PSMA. A base case time horizon of 18 months was chosen to correspond with available clinical trial follow-up data, provide a balanced assessment of costs and outcomes, and align with a prior published model in third-line mCRPC. Costs were reported in 2025 US dollars
At 18 months, total costs for a 100-patient cohort were $9.97 million with cabazitaxel versus $29.37 million with Lu-PSMA, equating to $19.40 million in savings overall:
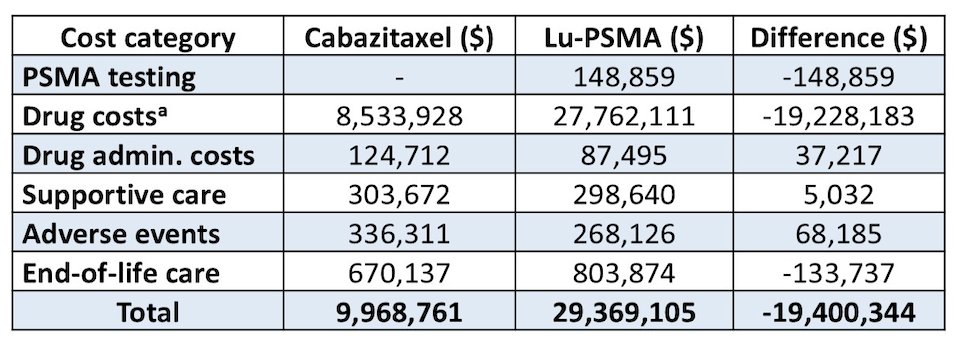
Cabazitaxel costs were about one-third those of Lu-PSMA, driven primarily by drug acquisition ($8.53 million versus $27.76 million; –$19.23 million). Other cost categories contributed smaller differences, ranging from savings with PSMA testing (–$0.15 million) to incremental costs associated with adverse event management (+$0.07 million): 
Clinically, at the primary analysis timepoint of 18 months, cabazitaxel was modeled to yield 9 fewer deaths, though this numerical advantage favoring cabazitaxel should be interpreted cautiously, as TheraP found no overall survival difference and reported overall survival results accounting for non-proportional hazards. Lu-PSMA demonstrated greater disease control, with 8 additional patients free of progression and PSA progression-free survival at 18 months, consistent with TheraP findings:
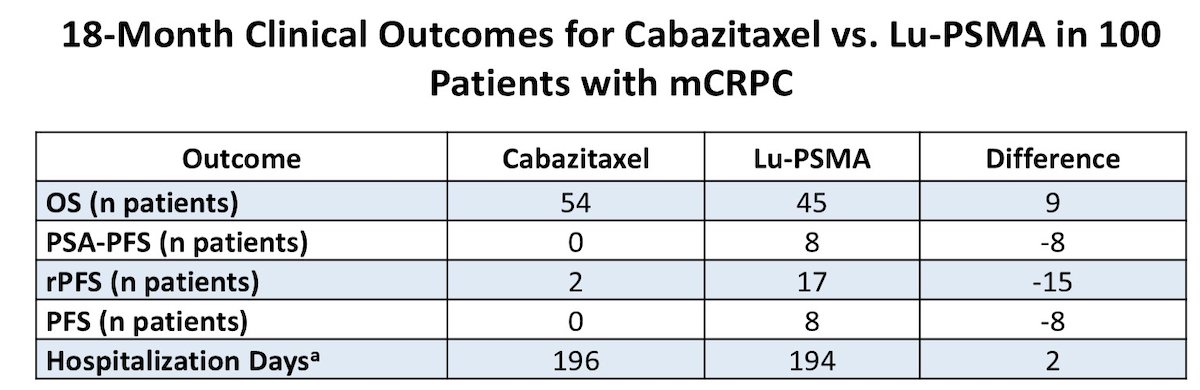
Cabazitaxel was associated with consistent and substantial cost savings across all time points. Lu-PSMA conferred greater progression-free survival and PSA benefits, especially during the 12–18 month interval.
Dr. Barata concluded his presentation discussing the clinical and cost impact of cabazitaxel versus Lu-PSMA for patients with mCRPC with the following take-home points:
- Cabazitaxel is estimated to reduce direct payer costs by approximately $194,000 per patient relative to Lu-PSMA, driven primarily by lower drug acquisition expenses
- These savings contrast with Lu-PSMA’s improved progression-free survival and PSA outcomes
Presented by: Pedro C. Barata, MD, MSc, FACP, Miggo Family Chair in Cancer Research, Co-Leader Genitourinary (GU) Disease Team, Director of GU Medical Oncology Research Program, University Hospitals Seidman Cancer Center, Associate Professor of Medicine, Case Western Reserve University, Case Comprehensive Cancer Center, Cleveland, OH
Reference: