(UroToday.com) At ASCO GU 2026, Dr. Daniel Kwon and colleagues presented results from a cluster-randomized implementation trial designed to improve delivery of prostate cancer germline testing within the U.S. Department of Veterans Affairs (VA).
Approximately 15,000 men with metastatic prostate cancer (mPCa) receiving care in the Veterans Administration (VA) could benefit from germline testing to inform treatment options, yet germline testing remains underutilized. In 2021, the VA implemented strategies to shift testing to oncologists (i.e., mainstreaming) to increase guideline-concordant testing. Mainstreaming led to increased adoption of germline testing by VA oncologists and was more efficient and timelier than genetics referral. However, germline testing rates remain low for many VA oncologists due to numerous barriers, including a lack of oncologist preparedness for germline testing, workflow issues, and systems challenges. This trial was designed to systematically address those barriers using implementation science frameworks.
This was a mixed-methods, cluster-randomized trial comparing the effectiveness of implementation strategies. VA oncologists not meeting a pre-specified germline test-order benchmark of 35% will be randomized to receive an additional strategy versus no additional strategy.
Eligibility criteria are as follows:
- VA oncologist who has authored progress notes in oncology clinics for ≥5 mPCa patients in the preceding year.
- Practicing at VA facilities with germline test order capability in the electronic health record.
- <35% of their mPCa patients have had mainstream germline test orders in the past two years.
A qualitative plan was embedded throughout the project. Investigators conducted four semi-structured interviews, informed by the Consolidated Framework for Implementation Research (CFIR), to understand:
- Local germline testing workflows.
- Challenges and enabling factors to mainstream testing.
- Challenges and enabling factors to the strategies.
Fidelity and adaptations will be assessed using the Longitudinal Implementation Strategy Tracking System through check-ins every two months.
The quantitative plan, informed by RE-AIM, will compare effectiveness (percentage meeting the 35% test-order rate benchmark) of strategies B versus B+C using mixed-effects modeling to account for clustering and effect sizes of implementation strategies.
The project schema illustrates a staged implementation approach.
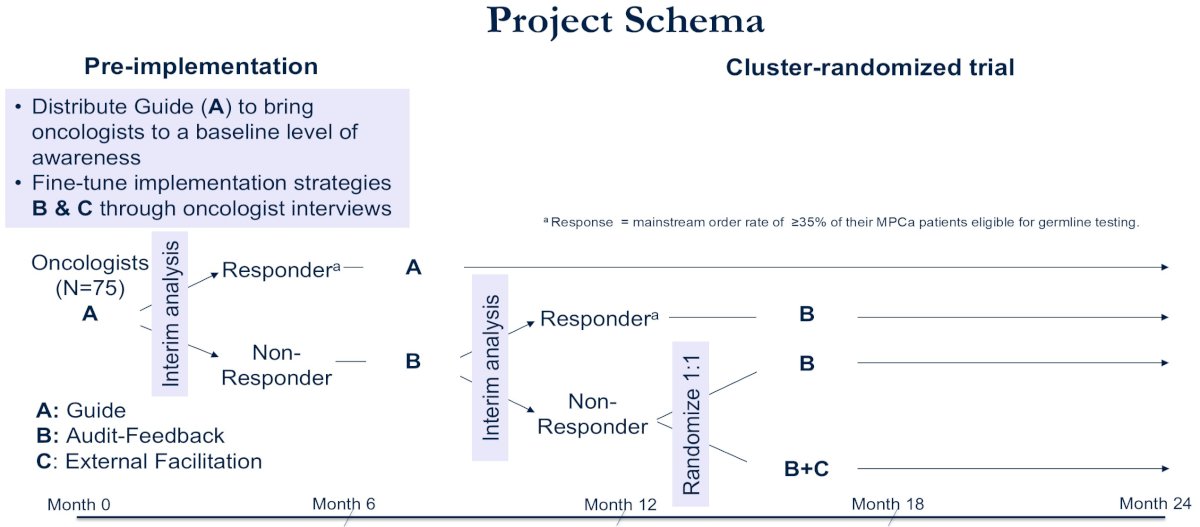
Pre-implementation
Guide (A) will be distributed to bring oncologists to a baseline level of awareness. Implementation strategies B and C will be fine-tuned through oncologist interviews.
Oncologists (N=75) will undergo interim analysis to classify them as responders (≥35% mainstream order rate) or non-responders.
Responders will continue to Guide (A). Non-responders will be randomized 1:1 at month 12 to:
- Audit-Feedback alone (B)
- Audit-Feedback plus External Facilitation (B+C)
The timeline extends to month 24, with re-evaluation at month 30.
This adaptive cluster-randomized structure allows escalation of implementation intensity only among clinicians failing to meet the benchmark.
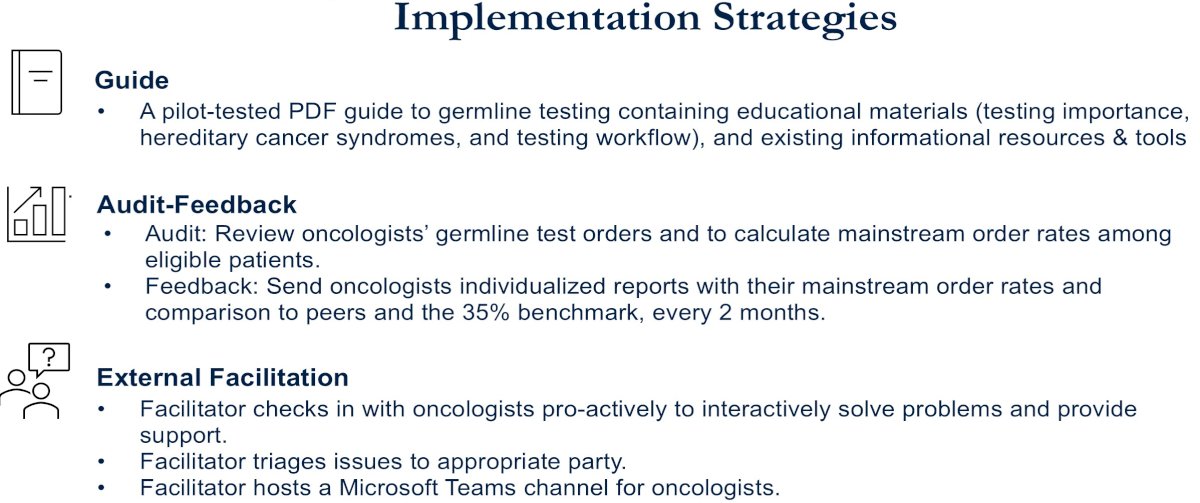
Implementation Strategies
Three implementation strategies will be deployed:
Guide (A): A pilot-tested PDF guide to germline testing containing educational materials (testing importance, hereditary cancer syndromes, and testing workflow), and existing informational resources and tools.
Audit-Feedback (B): Auditors will review oncologists’ germline test orders and calculate mainstream order rates among eligible patients. Feedback will include individualized reports comparing each oncologist’s order rate to peers and the 35% benchmark, delivered every two months.
External Facilitation (C): Facilitators check in with oncologists proactively to interactively solve problems and provide support. Facilitators triage issues to appropriate parties and host a Microsoft Teams channel for oncologists.
Project Procedures
- In the first 6 months, the investigators will disseminate a germline testing Guide (A)
- At month 7, for oncologists who do not exceed the 35% benchmark, the investigators will administer audit-feedback reports (B)
- At month 12, oncologists whose order rates are <35% will be randomized to either continue audit-feedback alone (B) or receive facilitation and audit-feedback (B+C).
- At month 24, investigators will stop the audit-feedback and facilitation strategies.
- At month 30, investigators will re-evaluate oncologists' test order rates.
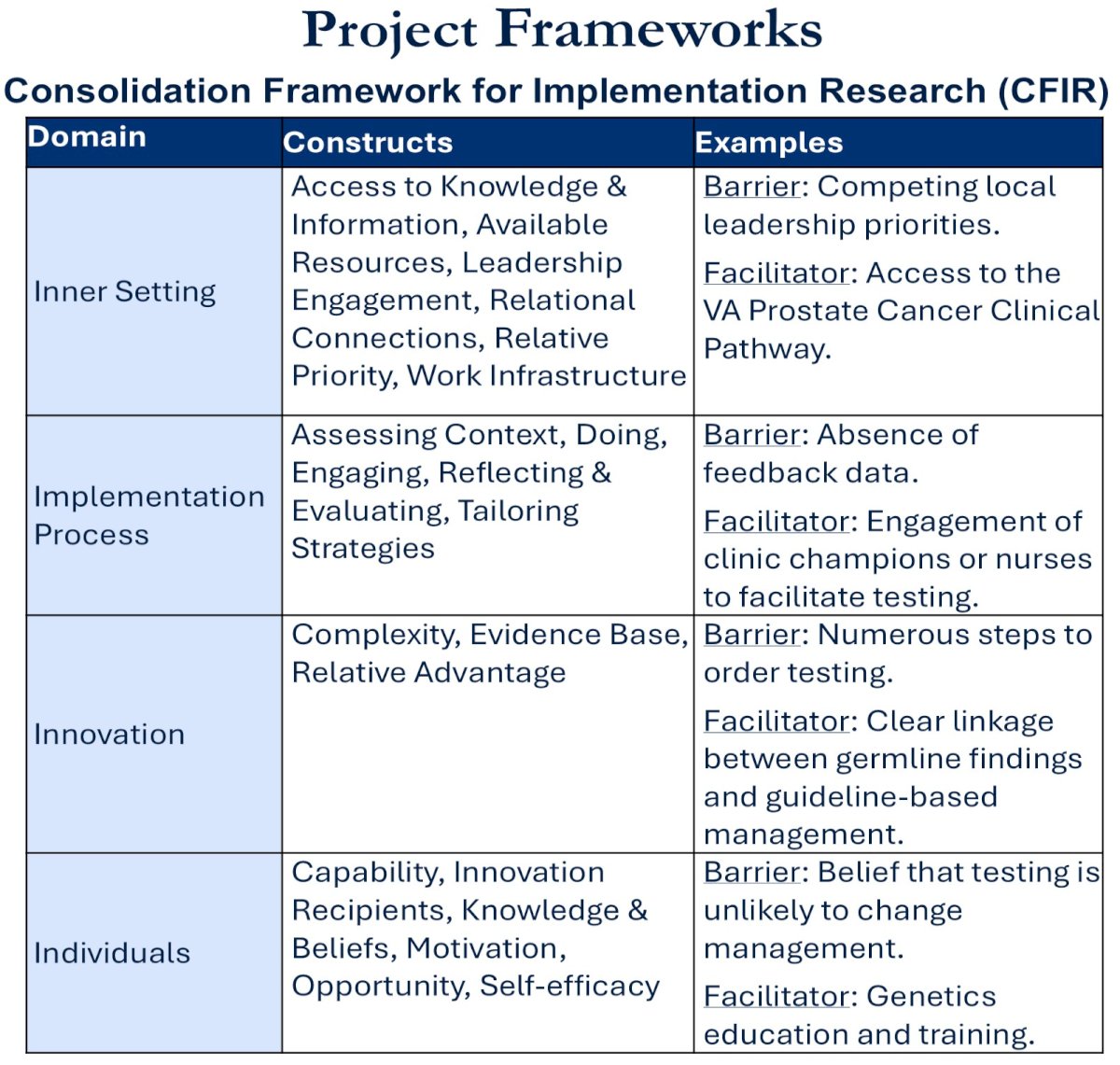
Project Frameworks
The Consolidation Framework for Implementation Research (CFIR) framework structures barrier identification across four domains:
- Inner setting
- Implementation Process
- Innovation
- Individuals
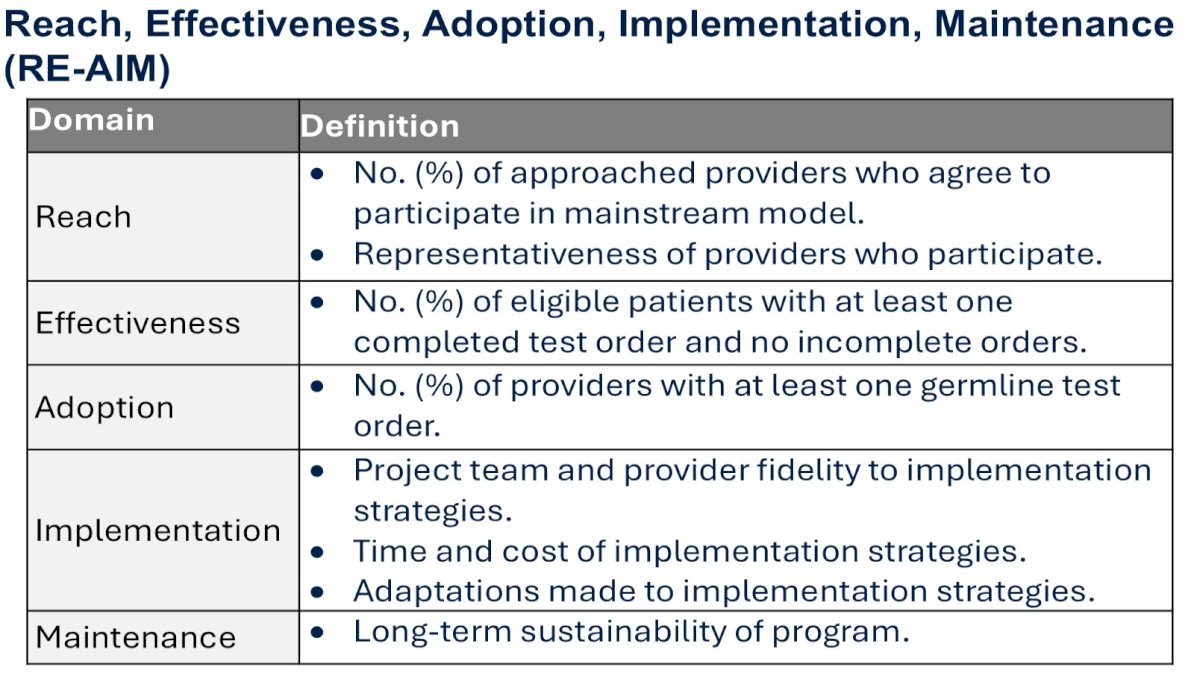
The Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework guides evaluation across:
- Reach: Percentage of approached providers agreeing to participate and representativeness of participating providers.
- Effectiveness: Percentage of eligible patients with at least one completed test order and no incomplete orders.
- Adoption: Percentage of providers with at least one germline test order.
- Implementation: Provider fidelity to strategies, time, and cost of implementation, and adaptations made.
- Maintenance: Long-term sustainability of the program.
Overall, this study aims to address a critical implementation gap: translating guideline-recommended germline testing into routine oncologic practice in a large integrated health system. Rather than focusing on patient-level barriers alone, this trial systematically evaluates provider-level behavior change using structured implementation science methodology.
The adaptive design is particularly notable. Instead of universally intensifying intervention, escalation (B+C) was targeted only to oncologists who remained below the 35% benchmark after audit-feedback. This improves efficiency and resource allocation.
By embedding CFIR and RE-AIM frameworks, the study rigorously evaluates not only effectiveness but also adoption, implementation fidelity, and sustainability—elements often absent in guideline uptake studies.
If successful, this model may serve as a scalable template for improving germline testing delivery in other integrated healthcare systems.
Presented by: Daniel Kwon, MD, Assistant Professor, Genitourinary Medical Oncology, Department of Medicine, University of California, San Francisco, CA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.