(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Poster Session A: Prostate Cancer. Neal Shore presented Poster 338: Patient preferences for treatment of nmHSPC: A discrete choice experiment.
Dr. Shore began by emphasizing that an androgen receptor pathway inhibitor plus androgen deprivation therapy is recommended as an effective alternative to ADT alone for patients with high-risk biochemically recurrent non-metastatic hormone-sensitive prostate cancer. In the EMBARK trial, both enzalutamide plus ADT and enzalutamide monotherapy significantly prolonged PSA progression compared with ADT alone in this population.1
While ARPI-based approaches consistently demonstrate improved efficacy with acceptable tolerability across multiple disease settings compared with ADT alone, he underscored the importance of understanding which treatment attributes patients value most. Incorporating patient preferences into shared decision-making is essential to optimizing clinical outcomes and aligning therapy with individual goals.
This was a non-interventional, international, discrete choice experiment designed to evaluate treatment preferences among patients with non-metastatic hormone-sensitive prostate cancer. Patients who had undergone definitive treatment for prostate cancer were recruited from the United States, United Kingdom, Germany, Spain, France, Italy, South Korea, Australia, and Brazil. Eligible participants were aged 18 years or older and had a diagnosis of hormone-sensitive prostate cancer treated with radical prostatectomy and/or radiotherapy. Patients with castration-resistant or metastatic disease were excluded.
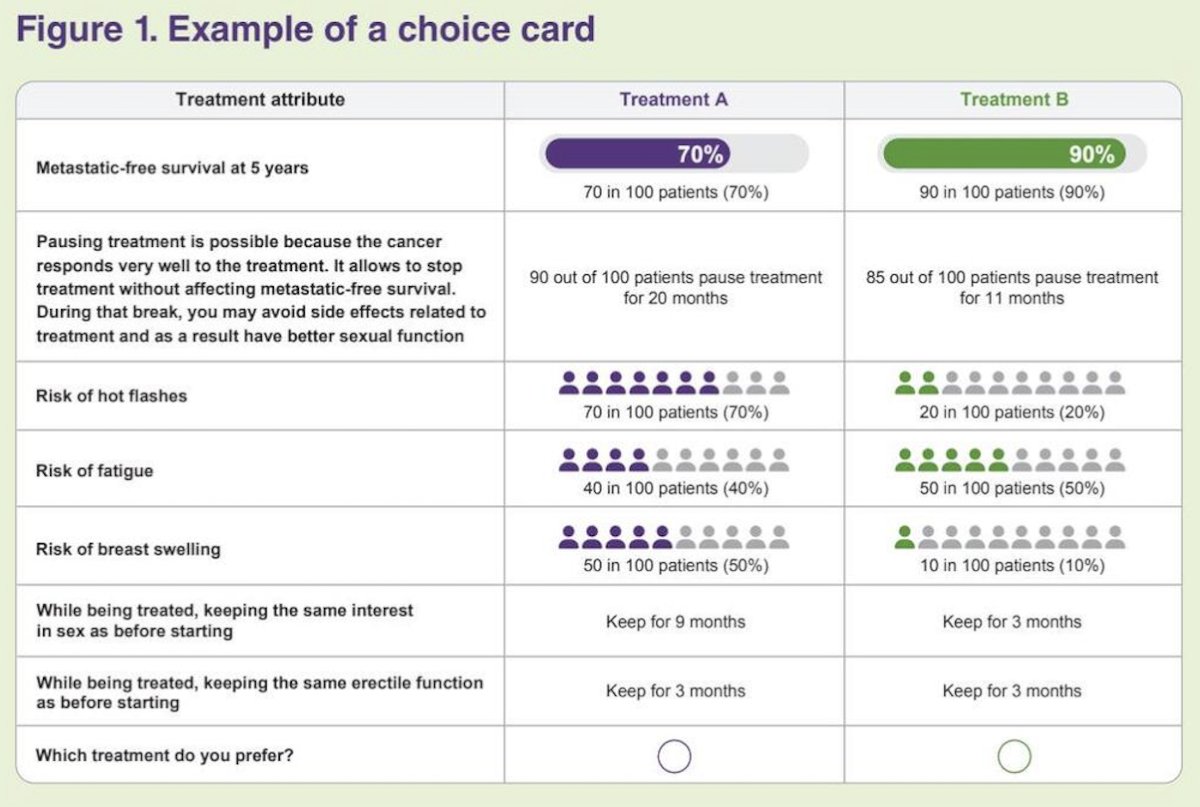
Key treatment attributes were identified through a targeted literature review and expert clinician input and included efficacy endpoints such as metastasis-free survival and the possibility of treatment suspension; safety considerations including risks of fatigue, hot flashes, and breast swelling; and sexual well-being factors such as duration of maintained sexual interest and erectile function. These attributes were refined through one-on-one semi-structured interviews with patients and physicians across multiple countries. In the discrete choice experiment, participants completed 12 choice tasks, each presenting two hypothetical treatment profiles with varying attribute levels, allowing estimation of the relative importance of each attribute in shaping patient treatment preferences (illustration of a choice card below)
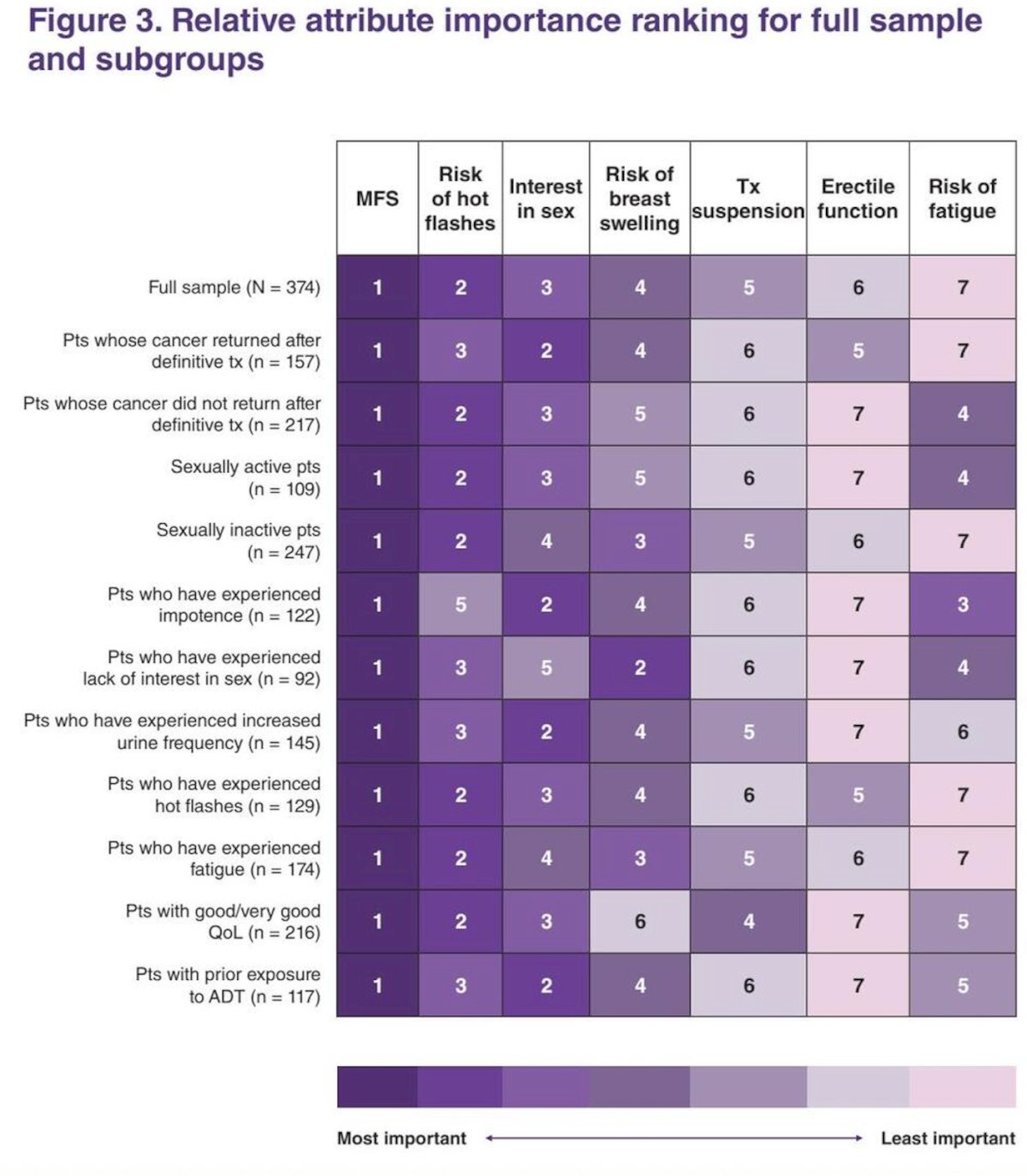
Preference weights were estimated using a regression-based discrete choice model and formed the basis for deriving the relative importance of each treatment attribute in patient decision-making, as well as for calculating predicted choice probabilities. Higher preference weights reflected greater relative importance within the DCE framework. Relative attribute importance rankings were generated for the overall sample and relevant subgroups, allowing assessment of how preferences varied across different patient characteristics.
Predicted preferences among the three treatment strategies, ARPI plus ADT, ARPI monotherapy, and ADT alone, were derived from these relative importance weights. Statistical analyses were conducted using a random parameter logit model, which accounts for heterogeneity in patient preferences and allows for variation in the strength of attribute importance across individuals. Treatment profiles from the EMBARK trial informed modeled treatment choice probabilities.
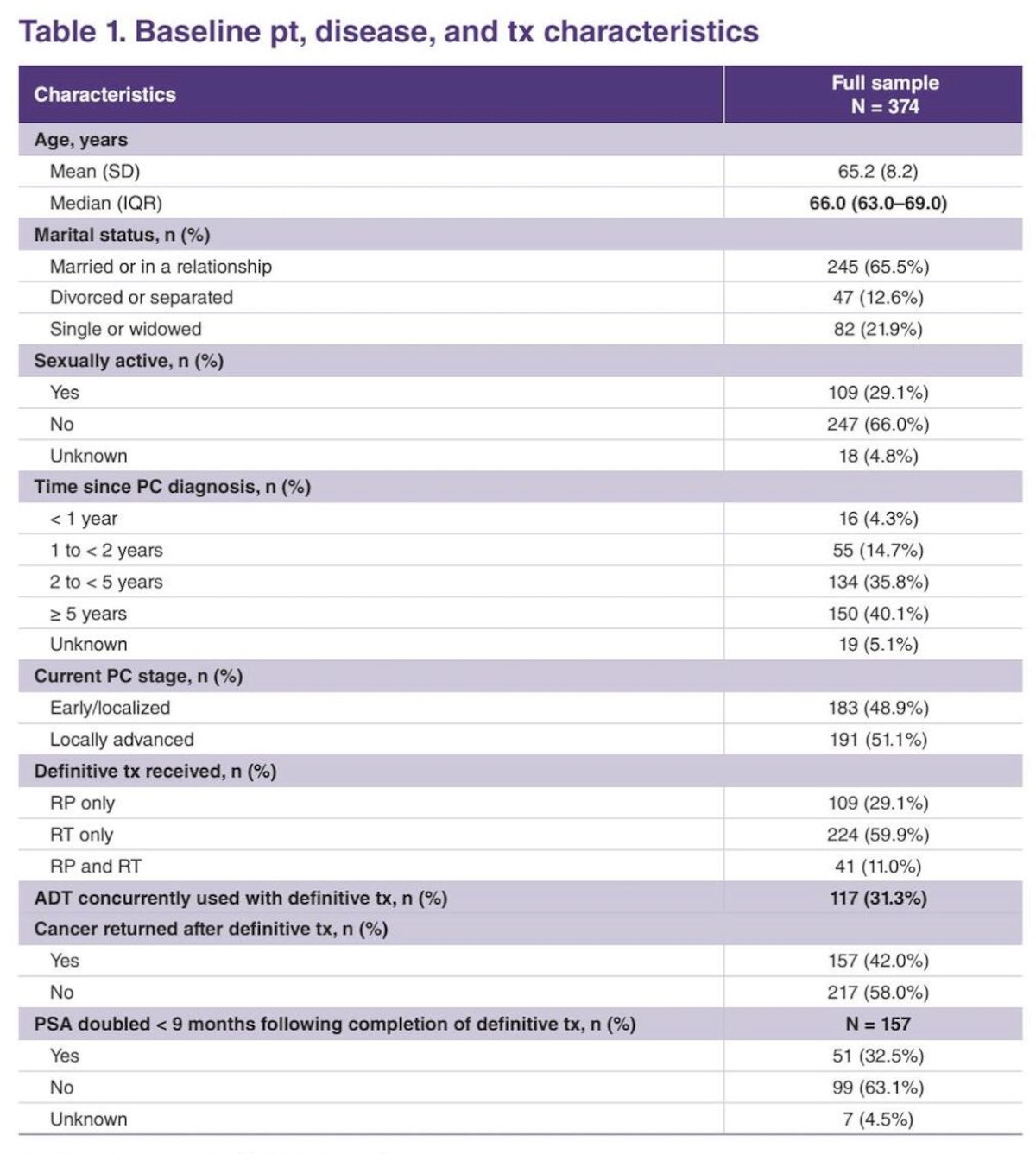
A total of 374 pls completed the tasks. The median age of respondents was 66 years. Most participants were married or in a relationship, and approximately 29% reported being sexually active. Forty-two percent experienced recurrence following definitive treatment. Baseline characteristics are shown below.
The most influential factors driving patient preference were:
- Five-year metastasis-free survival (28.9%)
- Risk of hot flashes (18.6%)
- Duration of sexual interest relative to baseline (17.4%)
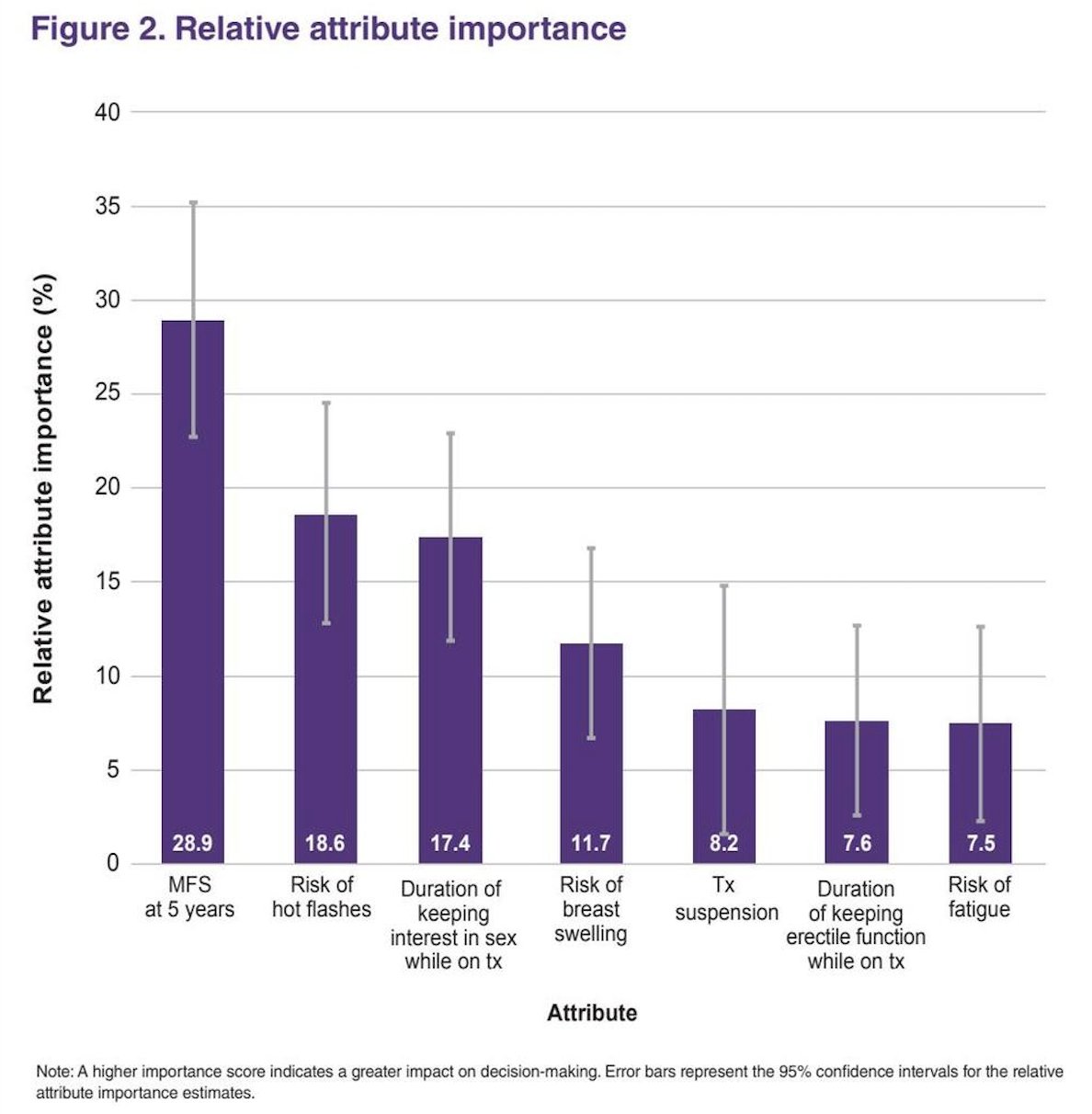
The least influential attributes in treatment decision-making were risk of breast swelling (11.7%), treatment suspension (8.2%), duration of maintaining erectile function while on therapy (7.6%), and risk of fatigue (7.5%), indicating that these factors carried comparatively lower weight in shaping overall patient preferences within the discrete choice framework. Overall, MFS remained the most influential attribute across all subgroups, including in the sexually active subgroup.
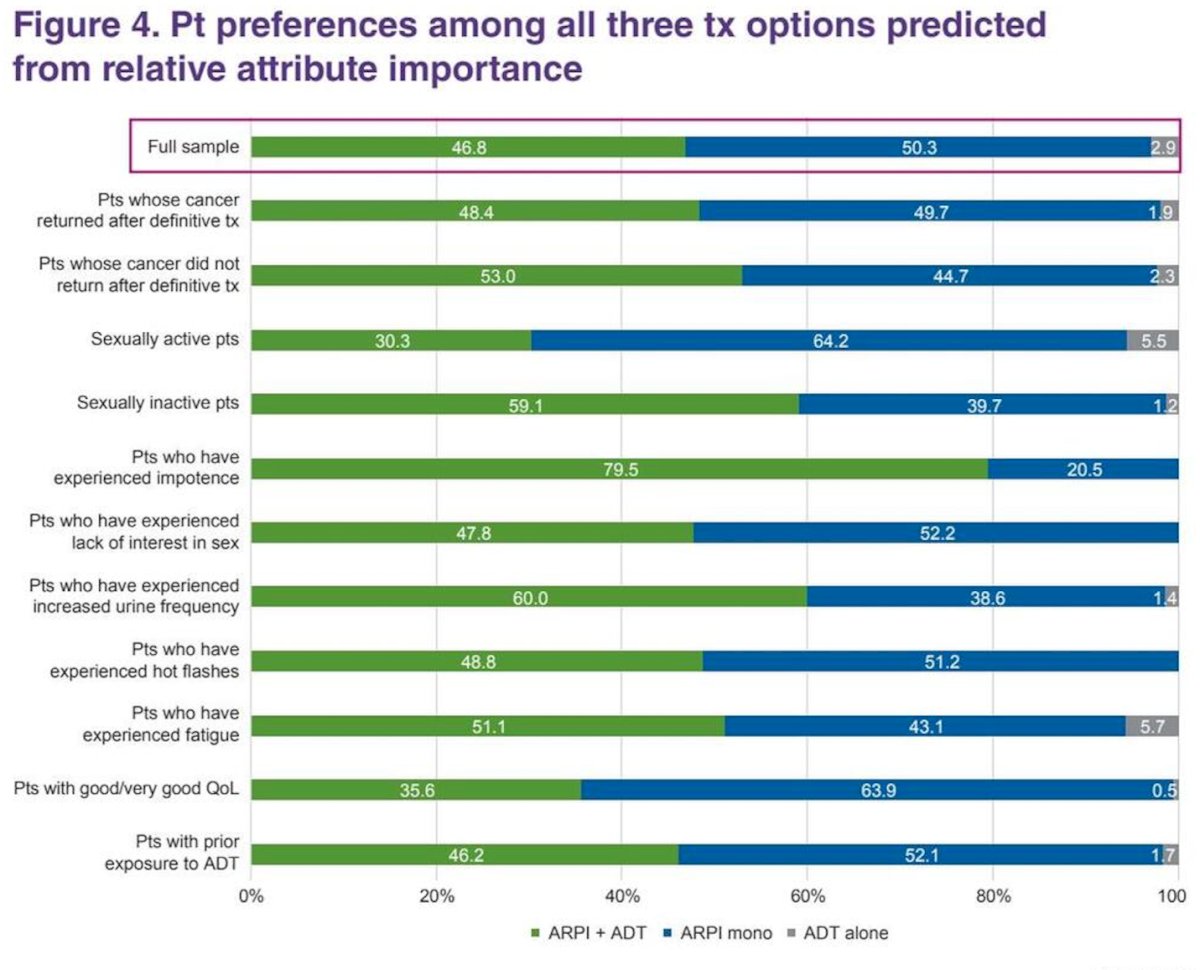
Based on modeled choice probabilities using EMBARK-based profiles, when all three treatment options were considered, the vast majority of patients (97.1%) demonstrated a strong preference for ARPI-based strategies compared with ADT alone (2.9%)
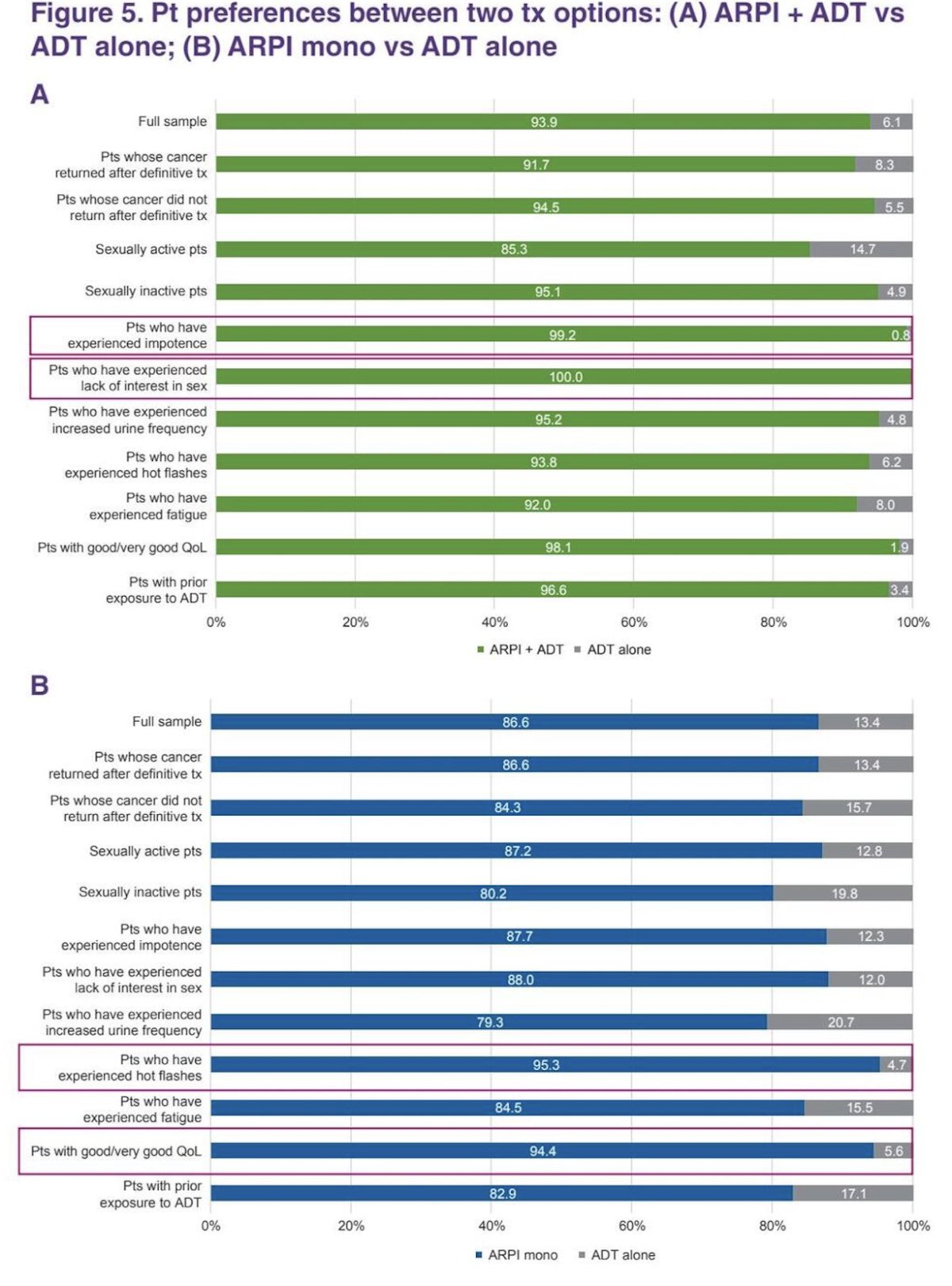
When evaluated in pairwise comparisons, a substantially larger proportion of patients preferred ARPI-based therapy over ADT alone: 93.9% versus 6.1% for ARPI plus ADT, and 86.6% versus 13.4% for ARPI monotherapy (Figure 5). Notably, preference for ARPI plus ADT was particularly strong among patients who had experienced lack of interest in sex (100%) and impotence (99.2%). Preference for ARPI monotherapy was especially pronounced among those who had experienced hot flashes (95.3%) and those reporting good or very good quality of life (94.4%) as shown in the figures below.
Lastly, Dr. Shore acknowledged several important limitations. Not all participants were fully representative of the broader patient population of interest, and potential cultural differences across participating countries were not specifically explored. In addition, although key attributes such as efficacy, safety, and sexual well-being were included, other relevant factors that may influence real-world decision-making, such as treatment cost, pill burden, and monitoring requirements, were not captured.
He also noted that patient-reported disease characteristics were not independently verified, which may have introduced inaccuracies. Furthermore, in the treatment option analysis, patients were assigned to the therapy with the highest predicted probability; this approach does not account for the magnitude of differences between probabilities and may overestimate the certainty of individual-level preferences.
Dr. Shore highlighted several key takeaways:
- In this discrete choice experiment, patients demonstrated a more favorable perception of the benefits associated with ARPI plus ADT compared with ADT alone.
- For most patients, survival benefit outweighed concerns regarding toxicity.
- Metastasis-free survival was the strongest driver of treatment preference, followed by risk of hot flashes and maintenance of sexual interest.
- The preference for ARPI-based therapies reflects patient-driven risk–benefit trade-offs that prioritize clinical efficacy while considering adverse events and sexual well-being.
- Overall, these findings support the use of personalized care plans for patients with high-risk biochemically recurrent non-metastatic hormone-sensitive prostate cancer.
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References: