(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Trials in Progress Poster Session A: Prostate Cancer. Dr. Neal D. Shore presented the trial in progress: Phase 2 study of ASP5541 (PRL-02), a long-acting intramuscular depot injection of abiraterone decanoate, in patients with advanced prostate cancer.
Dr. Shore outlined the design of an ongoing randomized phase 2 study evaluating ASP5541, a long-acting intramuscular depot formulation of abiraterone decanoate, in patients with advanced prostate cancer.
He began by highlighting the clinical context. Abiraterone acetate has improved survival in both metastatic hormone-sensitive and metastatic castration-resistant prostate cancer; however, it is associated with low oral bioavailability and risks of hepatotoxicity and mineralocorticoid-related adverse events, often necessitating glucocorticoid coadministration. ASP5541 is designed to deliver abiraterone via a long-acting intramuscular depot injection, targeting tissues and lymphatics while reducing systemic exposure. Its pharmacokinetic profile may decrease the need for prednisone, mitigate mineralocorticoid toxicity, and reduce treatment burden. A prior phase 1 study established 1260 mg every 12 weeks as the recommended phase 2 dose based on safety, pharmacodynamics, and preliminary efficacy.
This ongoing phase 2 trial (NCT07005154) plans to enroll approximately 218 adults across three cohorts in the Americas, Europe, and Asia-Pacific
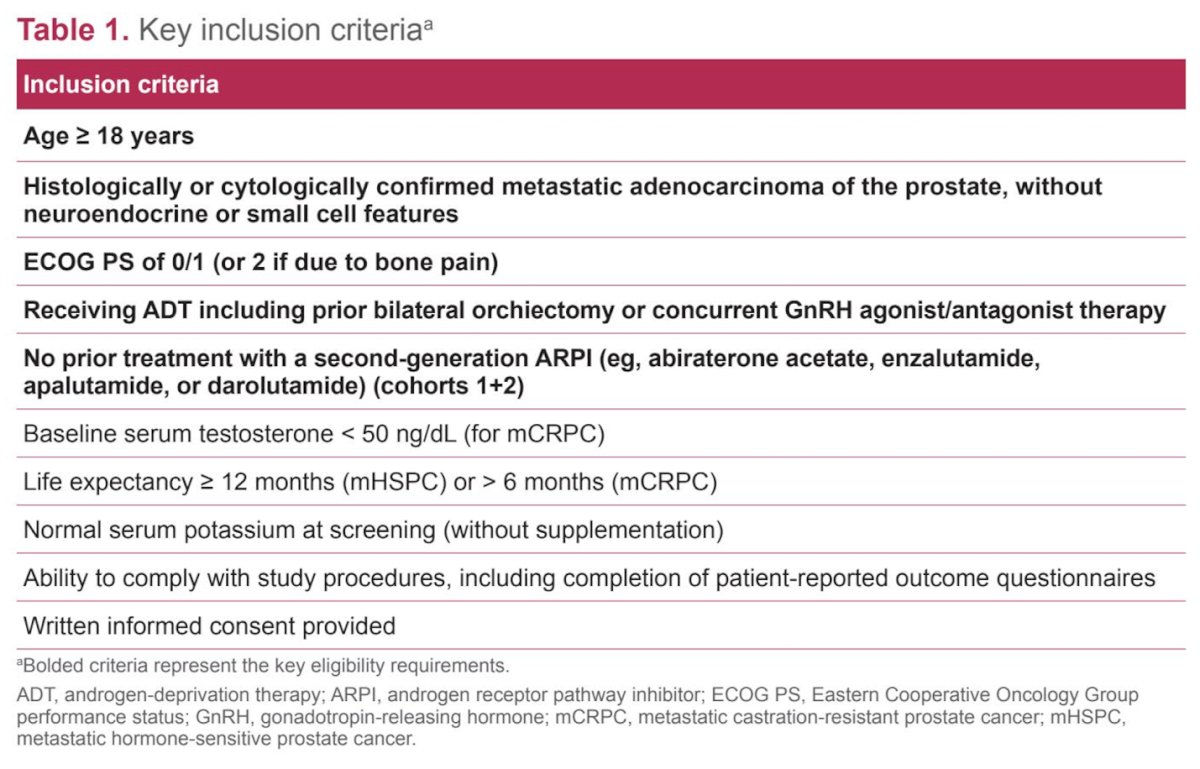
Eligible patients must have histologically or cytologically confirmed metastatic prostate cancer, ECOG performance status 0–1 (or 2 if due to bone pain), and ongoing androgen deprivation therapy through orchiectomy or concurrent GnRH agonist or antagonist therapy. For the mCRPC cohort, baseline serum testosterone must be <50 ng/dL.
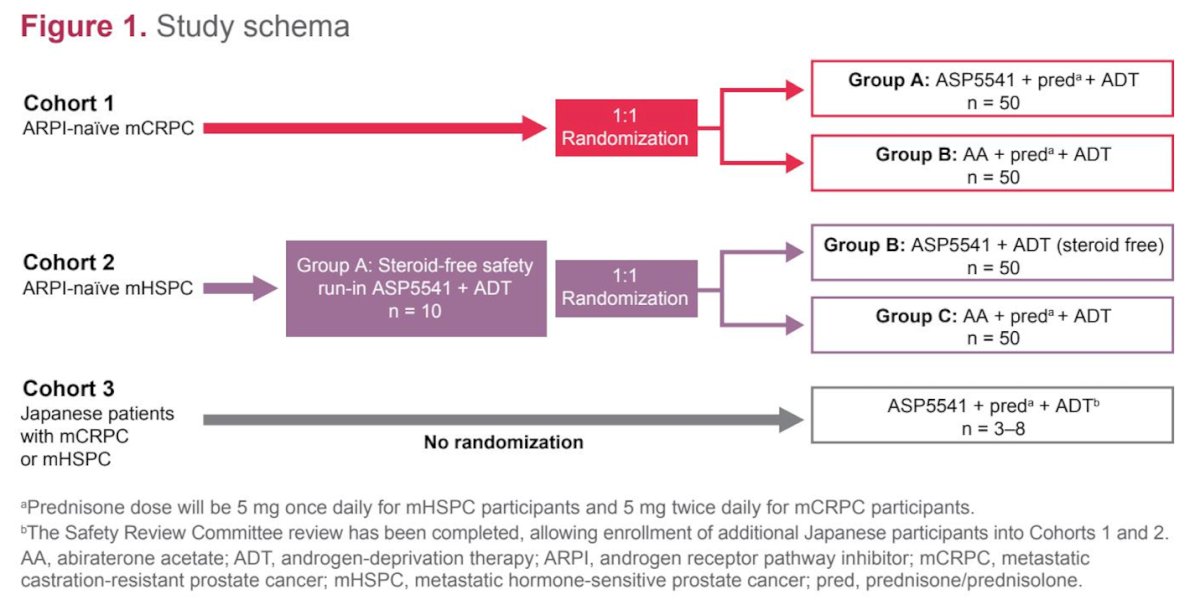
The study includes three distinct cohorts:
Cohort 1: ARPI-naïve mCRPC
Patients are randomized 1:1 (approximately 50 per group).
- Group A: ASP5541 + prednisone + ADT
- Group B: Abiraterone acetate + prednisone + ADT
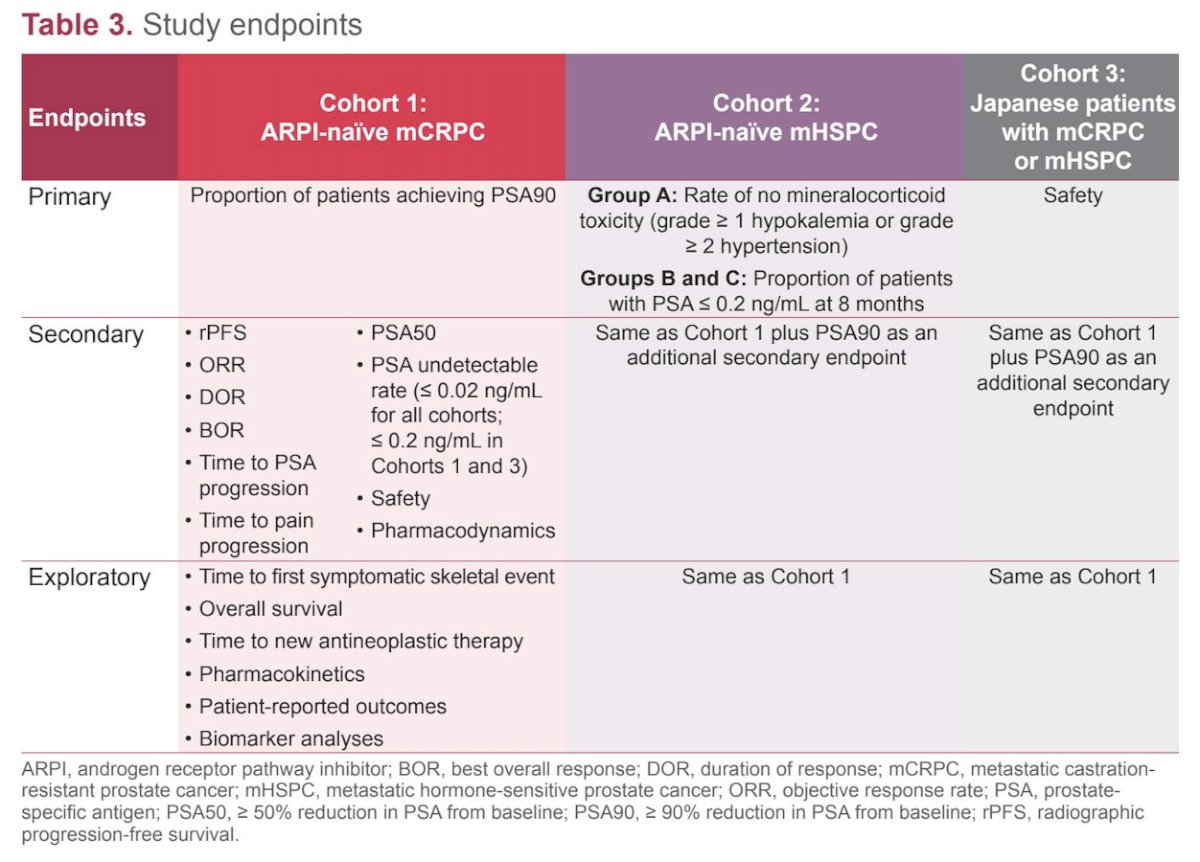
Primary endpoint: proportion of patients achieving PSA90.
Cohort 2: ARPI-naïve mHSPC
This cohort includes a safety run-in (Group A, n=10) followed by randomized groups (Groups B and C, n=50 each).
- Group A (safety run-in): ASP5541 + ADT without prednisone (steroid-free)
- Group B: ASP5541 + ADT (steroid-free)
- Group C: Abiraterone acetate + prednisone + ADT
Primary endpoints: - For Group A: rate of no mineralocorticoid toxicity (defined as absence of grade ≥1 hypokalemia or grade ≥2 hypertension)
- For Groups B and C: proportion of patients achieving PSA ≤0.2 ng/mL at 8 months.
Cohort 3: Japanese patients with mCRPC or mHSPC
This non-randomized cohort (n=3–8) will receive ASP5541 + prednisone + ADT, with safety as the primary endpoint.
Endpoints vary by Cohort. The primary and Secondary endpoints are shown below. Across cohorts secondary endpoints include radiographic progression-free survival, PSA50, PSA90 (in Cohorts 2 and 3), time to PSA progression, objective response rate, duration of response, best overall response, PSA undetectable rates (≤0.02 ng/mL for all cohorts; ≤0.2 ng/mL for Cohorts 1 and 3), safety, pharmacodynamics, and time to pain progression.
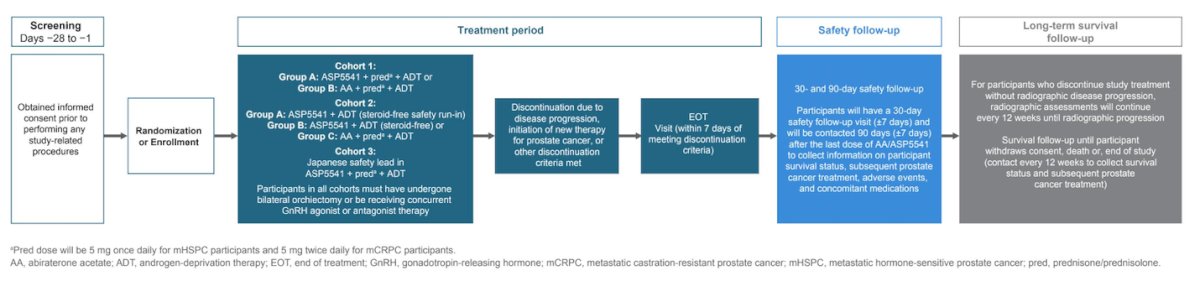
The study included a screening phase (Days −28 to −1), during which informed consent was obtained and pre-treatment procedures were completed, followed by randomization or enrollment. The treatment period consisted of multiple cohorts evaluating ASP5541 in combination with ADT or abiraterone, depending on disease setting, with predefined criteria for treatment discontinuation due to disease progression, toxicity, or other reasons, as well as an end-of-treatment visit.
After treatment, patients entered a safety follow-up phase 30 to 90 days after the last dose to assess adverse events, concomitant medications, and survival status. This was followed by long-term survival follow-up, conducted approximately every 12 weeks in patients who discontinued without radiographic progression, and every 12 weeks after progression for those who discontinued with disease progression, to capture overall survival and subsequent prostate cancer therapies.
Dr. Shore highlighted that study enrollment for Cohorts 1 and 2 is ongoing and Cohort 3 enrollment and Safety Review Committee review have been completed.
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.