(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Martin Gleave discussing genomic alterations and pathologic responses to neoadjuvant androgen receptor pathway inhibitor doublets versus docetaxel triplets in the Genomic Umbrella Neoadjuvant Study.
GUNS (NCT04812366) is a multi-centre adaptive phase II trial evaluating 24 weeks of biomarker-selected, neoadjuvant androgen receptor pathway inhibitor therapies on depth of pathologic response (<5 mm minimal residual disease) in high-risk localized prostate cancer. After 8 weeks of an androgen receptor pathway inhibitor doublet (LHRH agonist + apalutamide), men are assigned to 1 of 4 sub-protocols combining 16 weeks of an androgen receptor pathway inhibitor doublet with drugs defined by specific genomic biomarkers. Sub-protocol 1 enrolls men with AR-associated genomic alterations (ETS fusions, FOXA1, SPOP) treated with an androgen receptor pathway inhibitor doublet +/- abiraterone. Sub-protocol 2 randomizes men with aggressive genomic alterations (RB1, PTEN, TP53, AKT) to an androgen receptor pathway inhibitor doublet +/- docetaxel. Biomarkers like PTEN loss are needed to identify men who benefit from ADT-docetaxel, and at ASCO GU 2026, Dr. Gleave and colleagues investigated pathologic response to androgen receptor pathway inhibitor-docetaxel triplet in a biomarker-selected high-risk localized prostate cancer setting: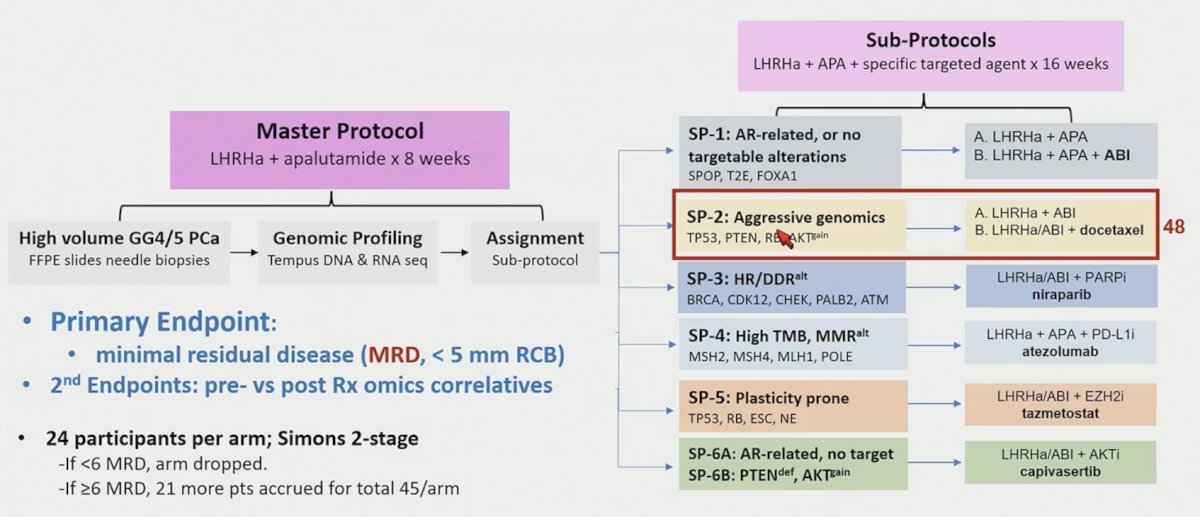
Diagnostic biopsies underwent Tempus’ CLIA-certified 648-gene panel DNA sequencing and whole-transcriptome RNA-seq. This analysis focuses on genomic analyses of the first 151 biopsies, and pathologic response rates in 48 men enrolled to the first stage of sub-protocol 2 who completed neoadjuvant therapy and surgery.
DNA sequencing from 129/151 biopsies reveals a genomic landscape dominated by ETS gene fusions (36%), FOXA1 (23%), TP53 (16%), SPOP (14%), PTEN (13%), and BRCA2 (9%) alterations. Overall tumor mutational burden of high-risk localized prostate cancer in GUNS is similar to metastatic prostate cancer and enriched for the unfavorable luminal PCS1 transcriptomic subtype. PTEN was IHC negative (≤10% positive prostate cancer cells) in 18%, half of whom had no reported genomic PTEN alteration. Most PTEN alteration cases, especially homologous deletions, were PTEN-IHC negative, but 2 PTEN homologous deletion cases were ≥50% PTEN-IHC positive, illustrating intra-patient or sampling heterogeneity. PTEN-IHC negative or TP53 genomic alterations, especially combined with an ETS fusion, was associated with intraductal carcinoma.
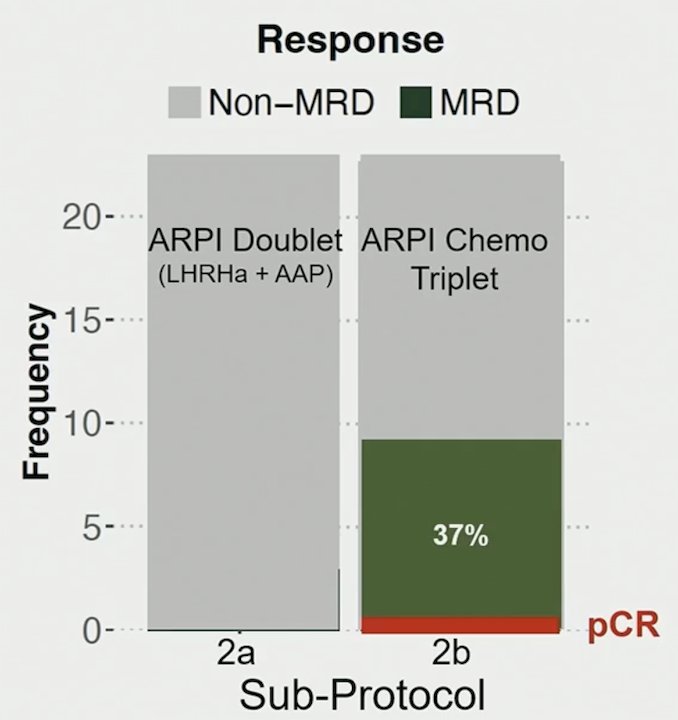
Sub-protocol 2 randomized 48 men with aggressive genomic alterations (TP53, PTEN, AKT) to an androgen receptor pathway inhibitor doublet (sub-protocol 2a) alone or with 6 cycles of docetaxel (sub-protocol 2b). Minimal residual disease rates were significantly higher in sub-protocol 2b (39% versus 0%, p-value = 0.016), including one pathological complete response:
While genomic PTEN alterations were excluded from sub-protocol 1, men assigned to sub-protocol 1 who were later found to be PTEN-IHC negative were more likely to be non-minimal residual disease (6/7) than minimal residual disease (1/7), suggesting PTEN-IHC negative may reduce response to androgen receptor pathway inhibitor. Additionally, an SPOP mutation was associated with minimal residual disease, and T2E fusions with non-minimal residual disease in sub-protocol 2b: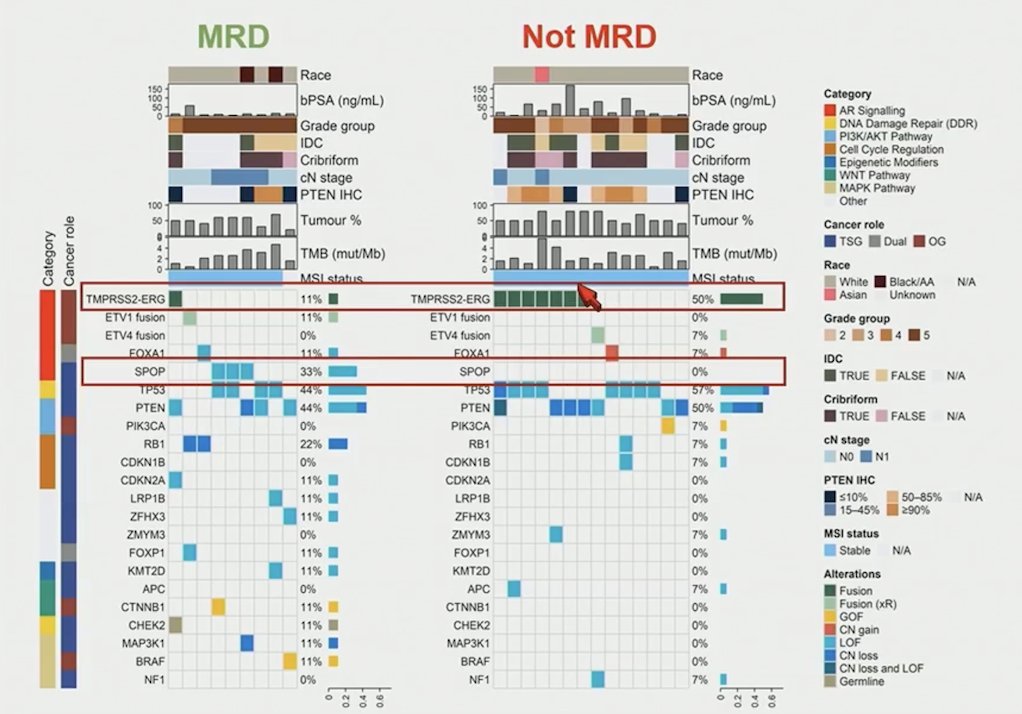
Dr. Gleave concluded his presentation discussing genomic alterations and pathologic responses to neoadjuvant androgen receptor pathway inhibitor doublets versus docetaxel triplets in GUNS with the following take-home points:
- Minimal residual disease rate was significantly higher in TP53, PTEN, RB1, and AKT altered cancers using an androgen receptor pathway inhibitor-docetaxel triplet (39%) versus a doublet (0%) (p = 0.016)
- Sub protocol 2b is expanding to the second stage, with a target enrollment of 45 participants
- ETS fusions were associated with unfavorable pathology and non-minimal residual disease response to androgen receptor pathway inhibitor-docetaxel triplets in TP53-mutated or PTEN-deficient cancers
- These findings, with planned pre- versus post-treatment genomic analyses, will improve our understanding of treatment sensitivity and resistance in prostate cancer genomic subtypes and guide the evolution of biomarker-targeted androgen receptor pathway inhibitor combination strategies
Presented by: Martin Gleave, MD, FRCSC, FACS, Vancouver Prostate Center, University of British Columbia, Vancouver, Canada