(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Daniel George discussing treatment utilization among patients with mHSPC in real-world US settings. The incidence of mHSPC is increasing in the US, partly due to screening practices. In recent years, the treatment options for mHSPC have expanded significantly, focusing on early treatment intensification through combination therapies such as ADT + androgen receptor pathway inhibitor, ADT + docetaxel doublet therapies, and ADT + androgen receptor pathway inhibitor + docetaxel triplet therapy, which can improve survival compared with monotherapy.
Although the number of life-prolonging treatment options for patients with mHSPC has increased, initial real-world evidence has demonstrated slow uptake. This study utilized a large, contemporary, real-world dataset to evaluate the characteristics and treatment utilization among US patients with mHSPC in recent years.
This retrospective, observational study used data from PRECISION, a harmonized dataset on patients with advanced prostate cancer. Adult men who were diagnosed with mHSPC during January 1, 2020 – December 22, 2025 (index date) and who initiated ≥1 therapy were included:
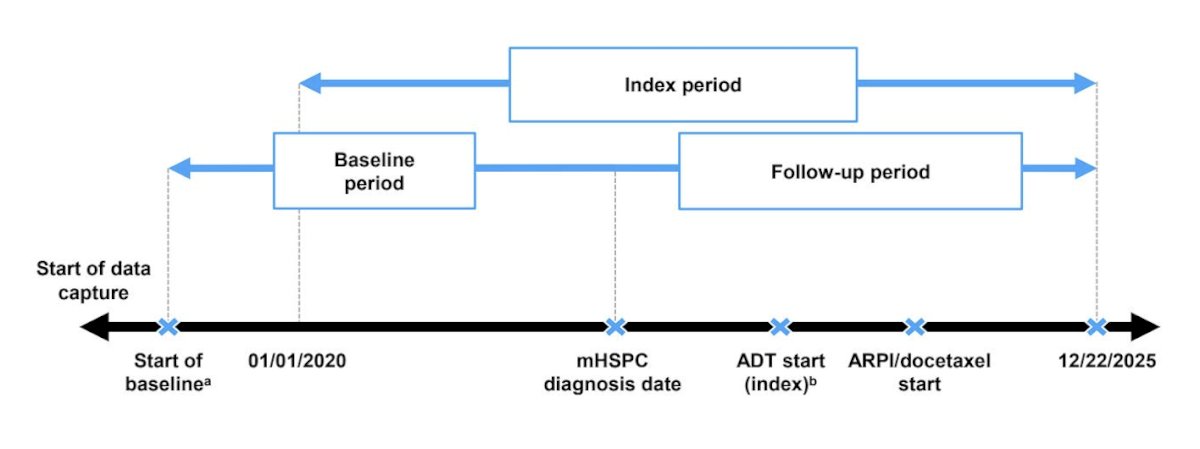
Patient characteristics were described at index, and treatment utilization was evaluated from index until progression to metastatic castration-resistant prostate cancer (mCRPC), death, or last follow-up. If an androgen receptor pathway inhibitor, docetaxel, or radiotherapy was started within 4 months of index/ADT start, it was considered a first-line combination. If it was started after >4 months, it was considered treatment intensification.
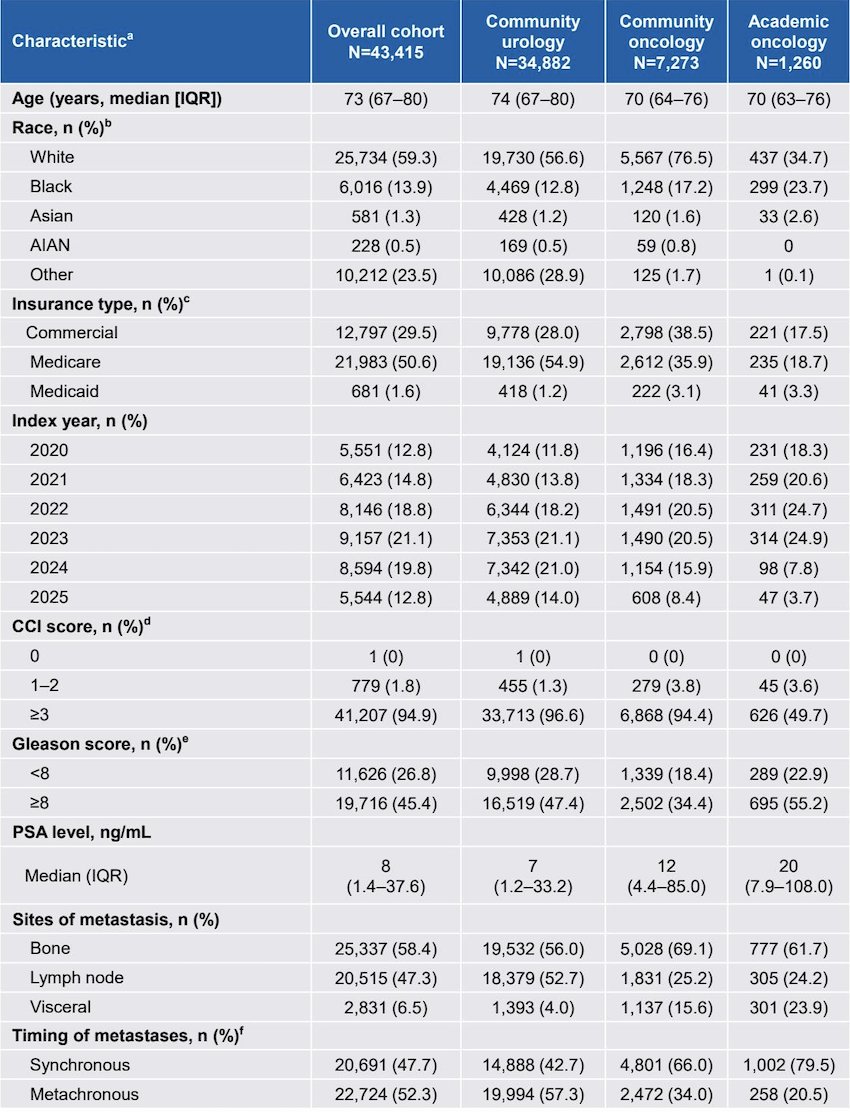
Among the 43,415 patients who met the inclusion criteria in PRECISION, 80.3%, 16.8%, and 2.9% were treated in community urology, community oncology, and academic oncology centers at index, respectively. The median age was 73 years (IQR 67-80), 59.3% were White, 47.7% had synchronous, and 52.3% had metachronous metastases. The median PSA level was 8 ng/mL (IQR 1.4-37.6):
When considering the entire mHSPC disease state, 39.2% received ADT monotherapy, 57.1% received doublet therapy (ADT + androgen receptor pathway inhibitor, 55.5%; ADT + docetaxel, 1.5%), and 3.8% received triplet therapy (ADT + androgen receptor pathway inhibitor + docetaxel). Among patients receiving doublet therapy, the median time from index to androgen receptor pathway inhibitor or docetaxel start was 0.7 (IQR 0–2.3) months. Among patients receiving triplet therapy, the median time from index to first agent (androgen receptor pathway inhibitor or docetaxel) was 0.4 (IQR 0–1.2) months, and from index to second agent was 2.0 (0.9–5.5) months. Overall, 0.8% and 14.0% had concomitant radiotherapy of the prostate and other sites, respectively.
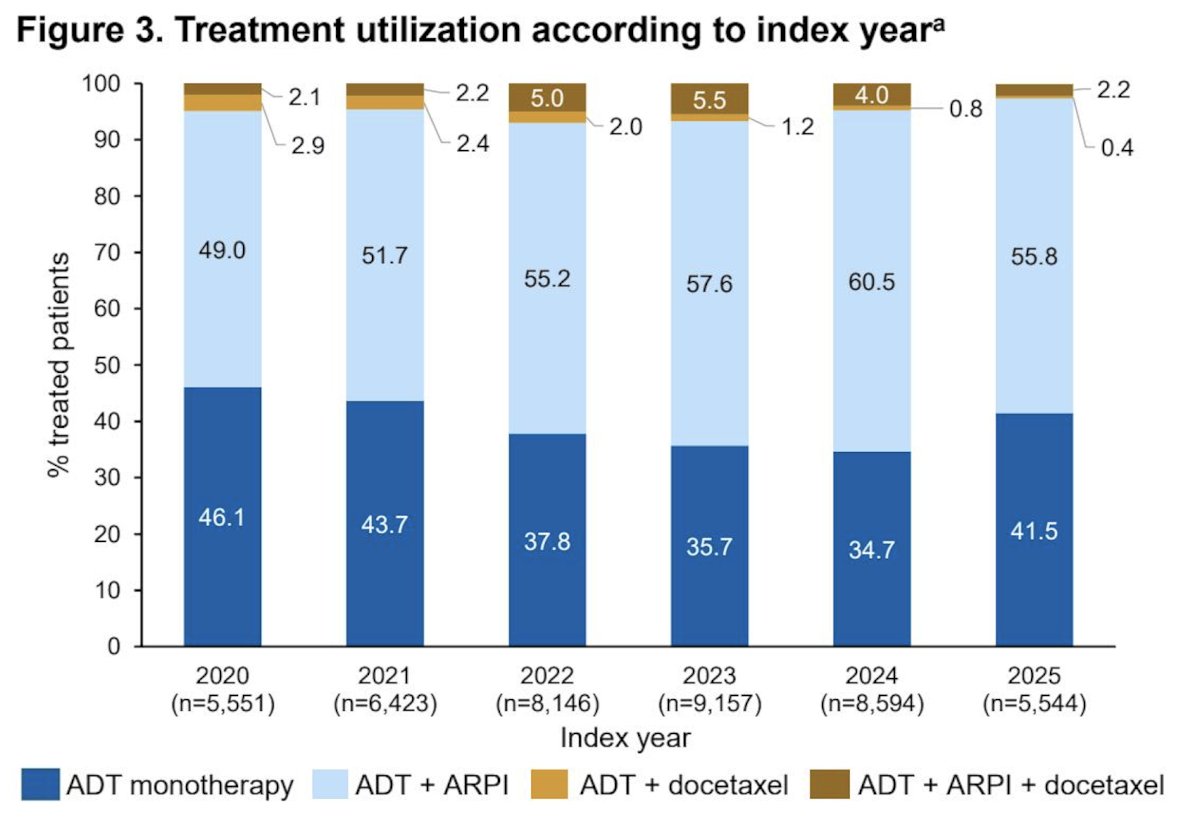
When analyzed by treatment setting, ADT monotherapy was more common in community urology centers (40.1%) versus community (35.8%) and academic (31.8%) oncology centers, while triplet therapy was more common in academic (12.9%) and community (8.7%) oncology centers compared with community urology centers (2.4%). When analyzed by index year, the rates of ADT monotherapy and ADT + docetaxel doublet therapy decreased, while ADT + androgen receptor pathway inhibitor doublet therapy increased. Triplet therapy use increased modestly over time:
When considering the first 4 months post-index, 49.2% of patients received ADT monotherapy, 48.3% received doublet therapy (ADT + androgen receptor pathway inhibitor, 46.6%; ADT + docetaxel, 1.7%), and 2.5% received triplet therapy. Among those receiving doublet therapy during this period, the median time from index to androgen receptor pathway inhibitor or docetaxel start was 0.4 (IQR 0–1.3) months. Among those receiving triplet therapy during this period, the median time from index to first agent (androgen receptor pathway inhibitor or docetaxel) was 0.1 (IQR 0–0.8) months, and from index to second agent was 1.3 (IQR 0.5–2.1) months.
After the first 4 months, there was evidence of treatment intensification in 20.4% of the patients initially on ADT monotherapy (addition of androgen receptor pathway inhibitor [19.4%], docetaxel [0.6%], or both [0.4%]) and 2.1% of those on doublet therapy (addition of androgen receptor pathway inhibitor in patients on ADT + docetaxel initially [0.9%] or addition of docetaxel in patients on ADT + androgen receptor pathway inhibitor initially [1.2%]). Treatment utilization rates overall and by timing of initiation are shown in the following figure:![After the first 4 months, there was evidence of treatment intensification in 20.4% of the patients initially on ADT monotherapy (addition of androgen receptor pathway inhibitor [19.4%], docetaxel [0.6%], or both [0.4%]) and 2.1% of those on doublet therapy (addition of androgen receptor pathway inhibitor in patients on ADT + docetaxel initially [0.9%] or addition of docetaxel in patients on ADT + androgen receptor pathway inhibitor initially [1.2%]). Treatment utilization rates overall and by timing of initiation are shown in the following figure:](/images/com-doc-importer/247-asco-gu-2026/asco-gu-2026-treatment-utilization-among-patients-with-mhspc-in-real-world-us-settings-a-prostate-cancer-disease-observation-precision-data-platform-analysis/image-3.jpg)
Among patients who initiated an androgen receptor pathway inhibitor as part of doublet or triplet therapy in the first 4 months post-index, 13.6% and 11.6%, respectively, subsequently switched to a different androgen receptor pathway inhibitor.
Dr. George concluded his presentation discussing treatment utilization among patients with mHSPC in real-world US settings with the following take-home points:
- ADT monotherapy utilization for mHSPC modestly declined between 2020 and 2025
- However, contrary to guidelines, overall, almost 40% of patients received only ADT monotherapy before the development of mCRPC, the last follow-up, or death
- Among patients who received ADT monotherapy within the first 4 months, 20.4% received subsequent treatment intensification
- Rates of ADT + androgen receptor pathway inhibitor doublet therapy increased over time. Triplet therapy utilization also increased, but only modestly
- Given that 80% of patients were treated in community urology centers at index, these trends largely represent the urology population
- Patients treated in oncology settings, particularly academic oncology, were less likely to receive ADT monotherapy and substantially more likely to receive triplet regimens than patients treated in urology settings
- Overall, these data suggest that, although the use of guideline-recommended regimens for mHSPC is increasing, there remains room for improvement
Presented by: Daniel George, MD, Medical Oncologist, Professor, Departments of Medicine and Surgery, Duke Cancer Institute, Duke University, Durham, NC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.