(UroToday.com) At the 2026 ASCO Genitourinary Cancers Symposium, Dr. Neal Shore presented results from the first safety-focused matching-adjusted indirect comparison (MAIC) evaluating darolutamide plus androgen deprivation therapy (DAR+ADT) versus other androgen receptor pathway inhibitor (ARPI)–based regimens in metastatic castration-sensitive prostate cancer (mCSPC).
This analysis represents the first safety-specific indirect comparison of individual adverse events across DAR+ADT, enzalutamide + ADT (ENZ+ADT), apalutamide + ADT (APA+ADT), and abiraterone + ADT (ABI+ADT) in mCSPC.
In the past decade, treatment of mCSPC has evolved rapidly with the introduction of docetaxel and ARPIs.1 Network meta-analysis (NMA) is the gold-standard method for comparing multiple treatments when direct head-to-head data are unavailable, as endorsed by Cochrane,2 NICE,3 ISPOR,4,5, and EU HTA.6 Previous NMAs in mCSPC have predominantly focused on efficacy endpoints, with limited evaluation of individual adverse events.7,8
Although multilevel network meta-regression (ML-NMR) is often recommended for indirect comparisons, MAIC allows adjustment using individual patient data (IPD) to align baseline characteristics and effect modifiers across trials.9 This approach avoids outcome-specific weighting and separate regressions for each endpoint.
This analysis, therefore, used an anchored MAIC framework to compare the safety profile of DAR+ADT with ENZ+ADT, APA+ADT, and ABI+ADT.
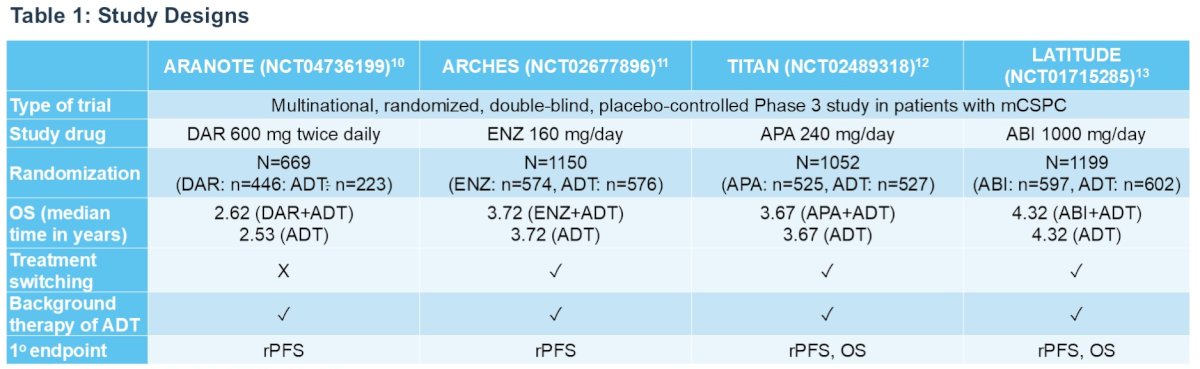
An anchored MAIC was conducted using individual patient data (IPD) from ARANOTE10 (DAR+ADT vs ADT) and published aggregate data from:
- ARCHES (ENZ+ADT)11
- TITAN (APA+ADT)12
- LATITUDE (ABI+ADT)13
ARANOTE IPD were reweighted to match baseline characteristics and treatment effect modifiers reported in comparator trials.
Propensity-score-based weighting adjusted for key effect modifiers used in reweighting included:
- Age
- ECOG performance status (0 vs ≥1)
- Gleason score (<8 vs ≥8)
- Disease volume (high vs low)
- Metastatic presentation (de novo vs recurrent)
- Presence of visceral metastases (yes vs no)
The matching quality was assessed using the effective sample size (ESS). Weighted generalized linear models with binomial likelihood and complementary log-log link were used to estimate annualized adverse event rate ratios.
Eight adverse events of special interest were evaluated:
- Fatigue
- Fractures
- Falls
- Hypertension
- Rash
- Mental impairment
- Dizziness
- Seizures
Safety analyses focused on all-grade adverse events.
Trial CharacteristicsTable 1 summarizes the design differences across trials:
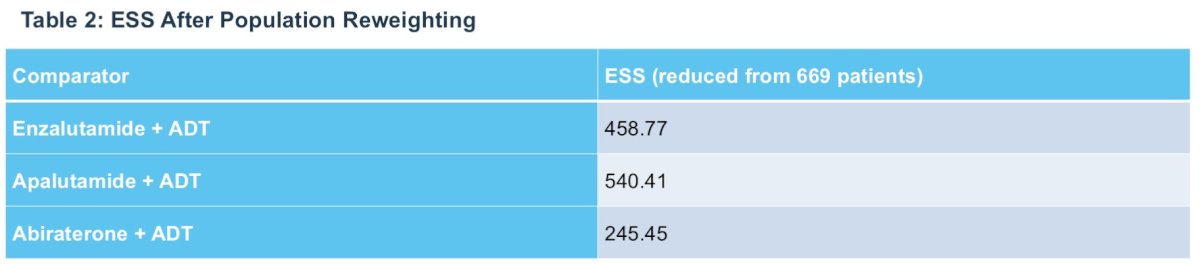
After population reweighting:
- ENZ+ADT comparison ESS: 458.77
- APA+ADT comparison ESS: 540.41
- ABI+ADT comparison ESS: 245.45
These ESS values indicate adequately preserved sample sizes after adjustment, supporting stability of the indirect comparisons.
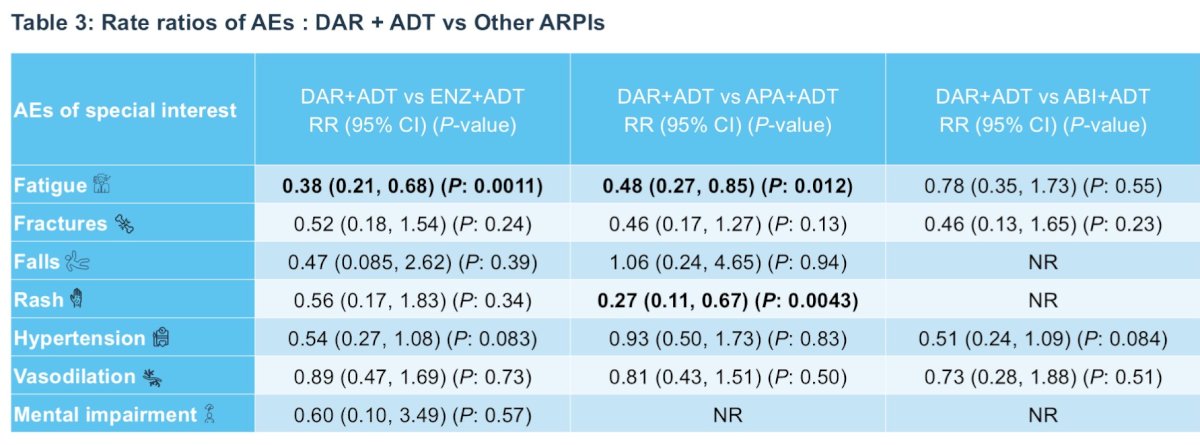
No seizure events were observed in the MAIC because no seizures occurred in ARANOTE.
With regards to fatigue, DAR+ADT demonstrated significantly lower rates of fatigue compared to:
- ENZ+ADT: RR 0.38 (95% CI 0.21–0.68), p=0.001 → 62% relative reduction
- APA+ADT: RR 0.48 (95% CI 0.27–0.85), p=0.012 → 52% relative reduction
Rash rates were significantly lower with darolutamide + ADT compared with apalutamide + ADT (RR 0.27; 95% CI 0.11–0.67; p=0.004), representing a 73% relative reduction.
Numerical trends favored darolutamide + ADT for fractures (vs all comparators) and hypertension (vs enzalutamide + ADT: RR 0.54; vs abiraterone + ADT: RR 0.51), although these differences did not reach statistical significance.
Vasodilation risks were comparable across all ARPI doublets.
Overall, DAR+ADT was associated with a more favorable safety profile compared with other ARPI+ADT combinations. The key statistically significant advantages included:
- Lower fatigue vs ENZ+ADT and APA+ADT
- Lower rash vs APA+ADT
Numerical trends favored DAR+ADT for:
- Fractures
- Falls
- Hypertension
- Vasodilation
These findings support the tolerability profile of darolutamide in mCSPC.
Dr. Shore noted the following strengths and limitations of the study:
- Differences in trial follow-up duration were addressed through exposure-time adjustment, supporting fair comparison of adverse event rates.
- There was good overlap between trial populations, as reflected by robust effective sample sizes (ESS) after reweighting, which supports the feasibility and stability of the adjusted comparisons.
- Although MAIC adjusts for observed treatment effect modifiers, residual confounding from unmeasured variables cannot be excluded.
Dr. Shore concluded as follows:
- This analysis represents the first safety-focused indirect comparison of individual adverse events evaluating darolutamide + ADT versus other ARP| + ADT regimens in men with mCSPC.
- Overall, darolutamide + ADT was associated with a more favorable safety profile compared with other ARPI + ADT combinations.
- Patients treated with darolutamide + ADT experienced significantly lower rates of fatigue compared with enzalutamide + ADT and apalutamide + ADT, and lower rates of rash compared with apalutamide + ADT.
- Numerical trends across other adverse events generally favored darolutamide + ADT, supporting its overall tolerability relative to other ARPI-based regimens.
- Collectively, these results suggest that darolutamide + ADT may offer safety advantages for patients with mCSPC and provide clinicians and payers with evidence to inform treatment selection across diverse patient populations.
Presented by: Neal D. Shore, MD, FACS, Director, START Carolinas/Carolina Urologic Research Center, Head of GU Oncology and Radiopharm START Research, AUC Urology Specialists, Myrtle Beach, SC
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th–28th, 2026
References:- Shore N, Elhage A, Gallagher P, et al. Safety profile of darolutamide plus androgen deprivation therapy compared with other androgen receptor pathway inhibitor combinations in metastatic castration-sensitive prostate cancer: a matching-adjusted indirect comparison. Prostate Cancer Prostatic Dis. 2025 Dec 9. doi:10.1038/s41391-025-01054-8. Online ahead of print.
- Chaimani A, Higgins JPT, Mavridis D, et al. Cochrane handbook for systematic reviews of interventions. Version 6.5 (updated February 2024). London: Cochrane; 2019–2024.
- National Institute for Health and Care Excellence (NICE). Guide to the methods of technology appraisal 2013. London: NICE; 2013. Available from: https://www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781. Accessed January 7, 2026.
- Hoaglin DC, Hawkins N, Jansen JP, et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 2. Value Health. 2011;14(4):429-437.
- Jansen JP, Fleurence R, Devine B, et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 1. Value Health. 2011;14(4):417-428.
- van Beekhuizen HJ, et al. Comparative safety and tolerability of androgen receptor pathway inhibitors in metastatic castration-sensitive prostate cancer: a real-world analysis. Pharmacoecon Open. 2025;9(4):597-609.
- Hoeh B, et al. Comparative adverse event profiles of androgen receptor pathway inhibitors in metastatic castration-sensitive prostate cancer. Eur Urol Focus. 2025;11(2):386-390.
- Flauto F, et al. Real-world safety of androgen receptor pathway inhibitors in metastatic castration-sensitive prostate cancer. Eur Urol Oncol. 2025 Jul 10:S2588-9311(25)00188-9.
- Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness research using matching-adjusted indirect comparisons. Value Health. 2012;15(6):940-947.
- Saad F, Armstrong AJ, Shore ND, et al. Abiraterone acetate plus prednisone in metastatic, castration-sensitive prostate cancer. J Clin Oncol. 2024;42(36):4271-4281.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase III study of enzalutamide plus androgen deprivation therapy in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974-2986.
- Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381(1):13-24.
- Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352-360.