(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a prostate cancer poster session. Dr. Mehmet Asim Bilen presented the results of a real-world comparison of PSA response in metastatic castration-sensitive prostate cancer (mCSPC) patients treated with apalutamide versus darolutamide, without prior or concurrent docetaxel.
Apalutamide and darolutamide are two androgen receptor pathway inhibitors (ARPIs) approved for the treatment of metastatic castration-sensitive prostate cancer (mCSPC) in combination with androgen deprivation therapy (ADT), with darolutamide also approved in combination with ADT and docetaxel.1-3 Post-hoc analyses of phase 3 trials, including TITAN and ARANOTE,4,5 have shown that early and sustained prostate-specific antigen (PSA) reductions ≥90% (PSA90) following treatment initiation have been associated with improved progression-free survival and overall survival in mCSPC.
Recently, real-world studies of patients with mCSPC have demonstrated that apalutamide is associated with a significantly higher likelihood of achieving PSA responses and improved overall survival relative to enzalutamide, abiraterone acetate, and darolutamide without docetaxel.6-11 Given the prognostic significance of achieving PSA90, there is a need to evaluate the comparative effectiveness of apalutamide versus darolutamide in real-world clinical practice in the United States.
The study objective was to compare PSA90 response by 6 months after treatment initiation for patients with mCSPC newly initiated on apalutamide without docetaxel versus darolutamide without docetaxel.
Clinical data were derived from Precision Point Specialty (PPS) Analytics from approximately 90 private community-based urology practices as part of routine clinical care in the United States, linked with administrative claims data from the Komodo Research Database. Data were de-identified and Health Insurance Portability and Accountability Act compliant.
This was a retrospective, longitudinal study of ARPI-naïve patients with mCSPC conducted in routine clinical practice. Patients were selected into mutually exclusive treatment cohorts based on the first dispensed ARPI therapy after first apalutamide or darolutamide initiation after FDA approval dates. Baseline characteristics were evaluated during the 12 months prior to the index date.
Eligible patients had mCSPC with a diagnosis code or clinical indicator for bone, nodal, or visceral metastases in the absence of castration resistance at or prior to the index date. Castration resistance was assessed based on a previously published algorithm incorporating ADT exposure, PSA levels, and clinical notes abstracted from electronic medical records and claims data. Patients were excluded if they received docetaxel within 90 days prior to or 30 days after ARPI initiation.
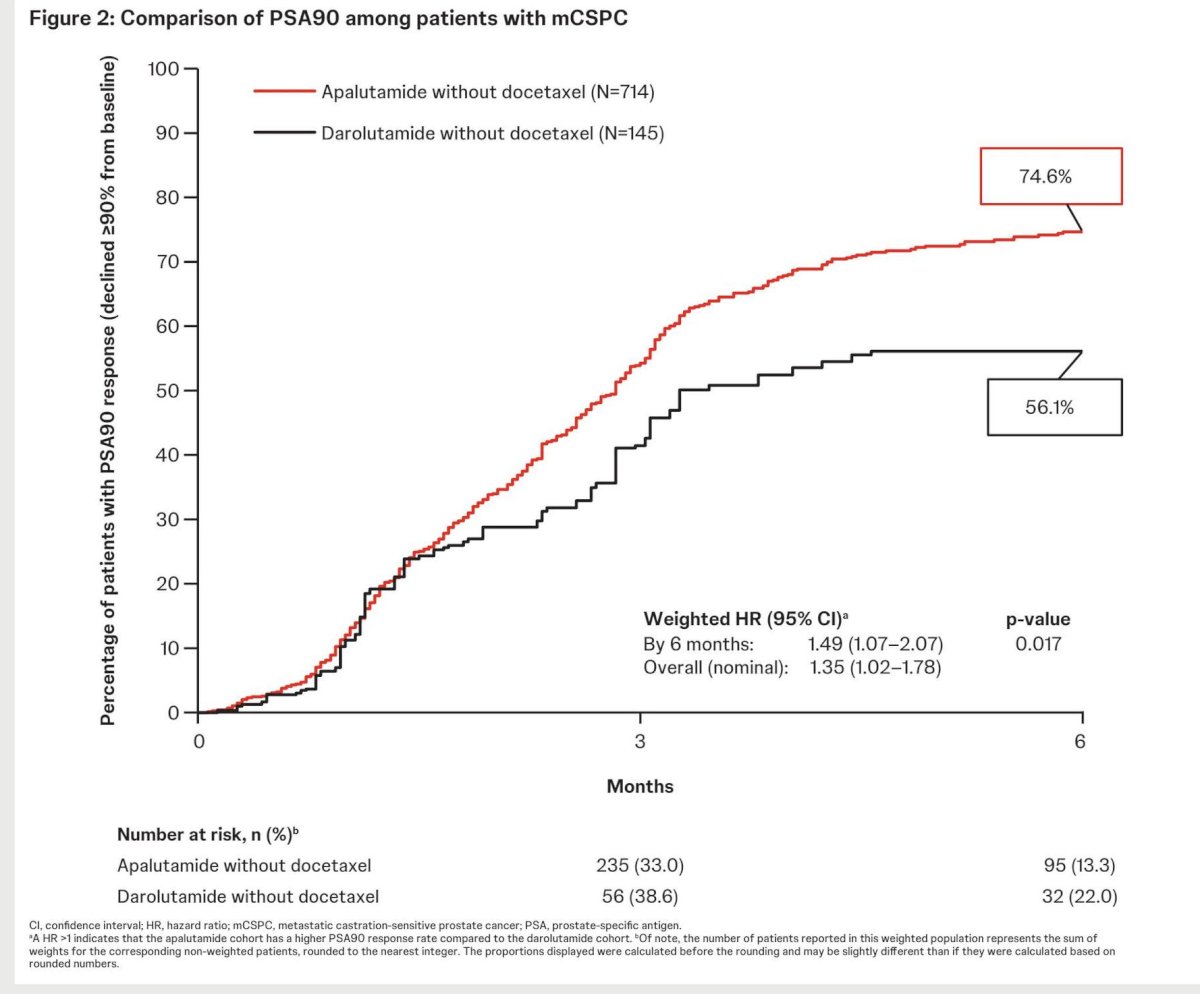
The primary outcome was the proportion of patients achieving a PSA90 response by 6 months after initiation of apalutamide without docetaxel or darolutamide without docetaxel.
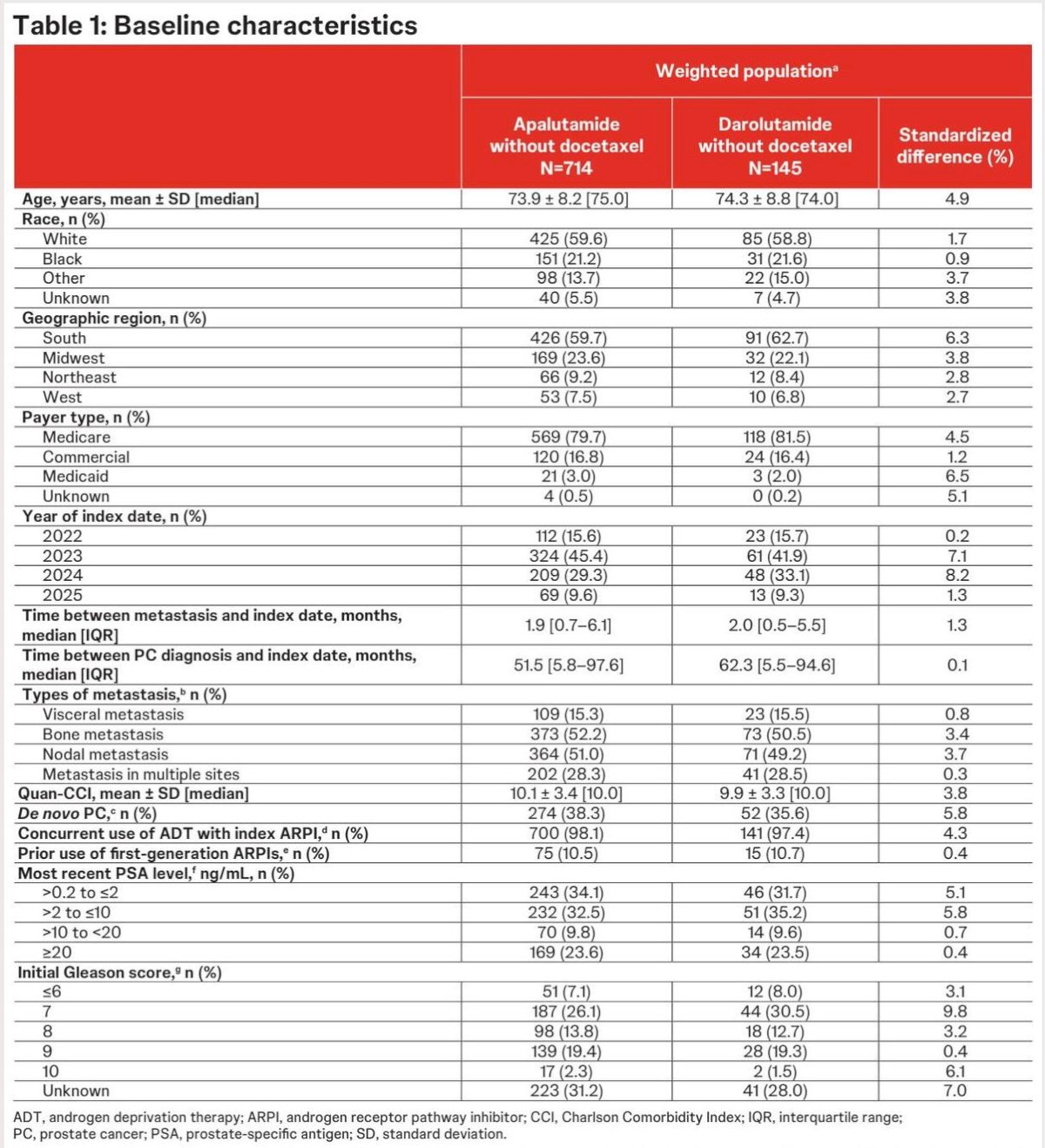
Inverse probability of treatment weighting, based on the propensity scores (PS), was used to account for differences in baseline characteristics between the apalutamide and darolutamide cohorts. Baseline characteristics between treatment cohorts were considered well-balanced after weighting, as indicated by standardized differences of <10%. A weighted Kaplan-Meier analysis was conducted to assess the proportion of patients who achieved PSA90. Weighted Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (Cls) for PSA90 response between apalutamide and darolutamide cohorts.
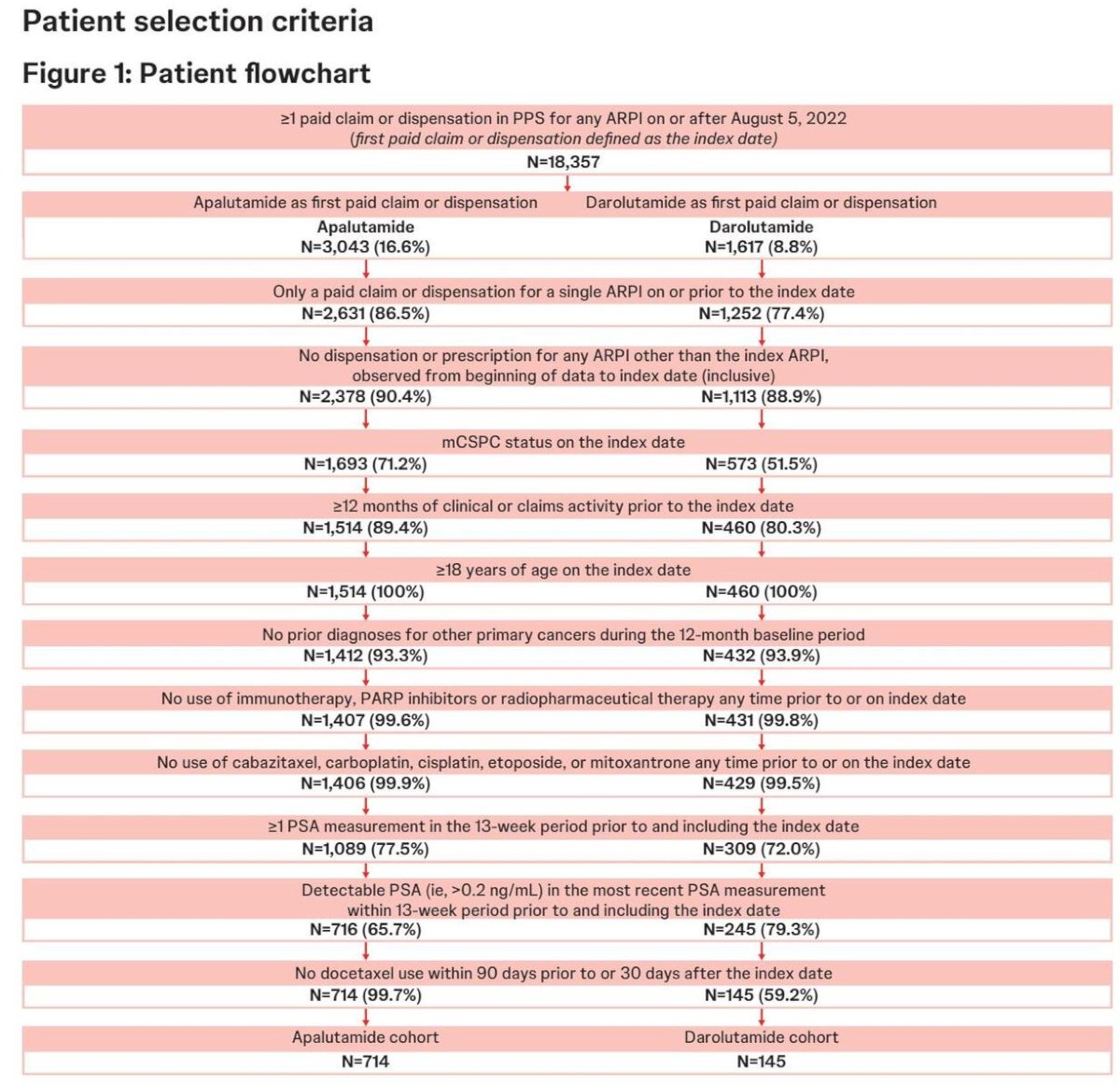
Overall, 714 patients initiating apalutamide without docetaxel and 145 initiating darolutamide without docetaxel were identified. Baseline patient characteristics were generally well balanced between weighted cohorts.
By 6 months, apalutamide patients had a 49% higher rate of PSA90 response compared to darolutamide patients (74.6% versus 56.1%; HR: 1.49, 95% CI: 1.07–1.27; p=0.017). The median time-to-PSA90 response was 2.8 months for apalutamide patients and 3.3 months for darolutamide patients.
Potential limitations were as follows:
- Miscoding or misclassification in the clinical record or through the administrative claims can lead to selection and information biases despite efforts to balance the study populations
- PSA testing conducted outside of the PPS network was not captured, which may have led to an underestimation of PSA90 response rates
- Given the use of open-source data, combination treatment with docetaxel may not be completely captured if administered outside of PPS network or hospitals that do not provide data to KRD+
- Darolutamide was used off-label prior to FDA approval for mCSPC without docetaxel on June 3, 2025; prior studies have demonstrated frequent off-label use without docetaxel during this time period'
- Regression analyses could only adjust for measured covariates, and residual confounding may be present
Dr. Asim Bilen concluded as follows:
- Earlier deep PSA response was observed in a significantly higher proportion of ARPI-naïve patients initiating apalutamide without docetaxel relative to those initiating darolutamide without docetaxel, suggesting larger therapeutic benefit for apalutamide among patients with mCSPC, even without treatment intensification
- Treatment efficacy in routine clinical practice may be influenced by molecular and treatment administration factors, including dosing frequency and food requirements, which can affect adherence and systemic exposure
- These findings combined with the demonstrated significant overall survival benefit for apalutamide vs darolutamide without docetaxel may hold substantial long-term clinical significance and could contribute to informing treatment strategies for patients with mCSPC
Presented by: Mehmet Asim Bilen, MD, Associate Professor, Department of Hematology and Medical Oncology, Emory University School of Medicine, Director, Genitourinary Medical Oncology Program, Winship Cancer Institute of Emory University, Atlanta, GA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- U.S. Food and Drug Administration. FDA approves apalutamide for metastatic castration-sensitive prostate cancer. 2019. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-apalutamide-metastatic-castration-sensitive-prostate-cancer. Accessed February 26, 2026.
- U.S. Food and Drug Administration. FDA approves darolutamide tablets for metastatic hormone-sensitive prostate cancer. 2022. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-darolutamide-tablets-metastatic-hormone-sensitive-prostate-cancer. Accessed February 26, 2026.
- U.S. Food and Drug Administration. FDA approves darolutamide for metastatic castration-sensitive prostate cancer. 2025. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-darolutamide-metastatic-castration-sensitive-prostate-cancer. Accessed February 26, 2026.
- Chowdhury S, Armstrong AJ, Tombal B, et al. Darolutamide plus androgen-deprivation therapy in metastatic hormone-sensitive prostate cancer (ARANOTE). Ann Oncol. 2023;34(5):477-485.
- Saad F, Fizazi K, Jinga V, et al. Darolutamide plus androgen-deprivation therapy in metastatic hormone-sensitive prostate cancer: extended follow-up analysis. Eur Urol Oncol. 2025;8(5):1321-1332.
- Lowentritt B, Brown G, Singh M, et al. Real-world outcomes in metastatic castration-sensitive prostate cancer treated with androgen receptor pathway inhibitors. Rev Urol. 2024;23(2):29-40.
- Brown G, Lowentritt B, Singh M, et al. Comparative effectiveness of androgen receptor pathway inhibitors in metastatic castration-sensitive prostate cancer. Rev Urol. 2024;23(2):15-27.
- Bilen MA, Brown G, Lowentritt B, et al. Real-world comparison of apalutamide versus darolutamide without docetaxel in metastatic castration-sensitive prostate cancer. Adv Ther. 2025;42(7):3437-3454.
- Lowentritt B, Brown G, Singh M, et al. Real-world comparison of overall survival in patients with metastatic castration-sensitive prostate cancer initiating apalutamide without docetaxel versus darolutamide without docetaxel. J Comp Eff Res. 2025;14(7):e250023.
- Lowentritt B, Brown G, Singh M, et al. Real-world comparison of achieving undetectable prostate-specific antigen response in patients with metastatic castration-sensitive prostate cancer treated with apalutamide without docetaxel versus darolutamide without docetaxel. Presented at: International Prostate Cancer Update (IPCU); 2026; Vail, CO.
- Lowentritt B, Brown G, Singh M, et al. Real-world comparison of PSA response in patients with metastatic castration-sensitive prostate cancer treated with apalutamide without docetaxel versus darolutamide without docetaxel. Presented at: Genitourinary Cancers Symposium (GPCC); 2026; Park City, UT.