(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a prostate cancer poster session. Dr. Andrew Hahn presented the results of a real-world analysis evaluating the prevalence of major adverse cardiac events in men with prostate cancer receiving ADT.
Androgen deprivation therapy (ADT) remains the backbone of treatment for advanced prostate cancer;1,2 however, prior studies have reported an increased risk of major adverse cardiac events (MACE) associated with ADT, particularly among patients with pre-existing cardiovascular disease (CVD) or cardiovascular risk factors. Oral GnRH antagonists, including relugolix, have demonstrated lower rates of MACE compared with GnRH agonists in randomized clinical trials, most notably in the HERO study,3 which demonstrated a 54% lower risk of MACE in men treated with relugolix versus leuprolide (2.9% versus 6.2%; HR: 0.46, 95% CI: 0.24-0.88).4 Despite these findings, contemporary real-world data evaluating cardiovascular outcomes following ADT initiation, particularly across different ADT classes and patient risk profiles, remain limited and poorly characterized.
The objective of this study was to evaluate the prevalence of MACE among men receiving ADT for prostate cancer in real-world clinical practice in the United States and to assess differences in cardiovascular outcomes by ADT class, including GnRH agonists, GnRH antagonists, and relugolix.
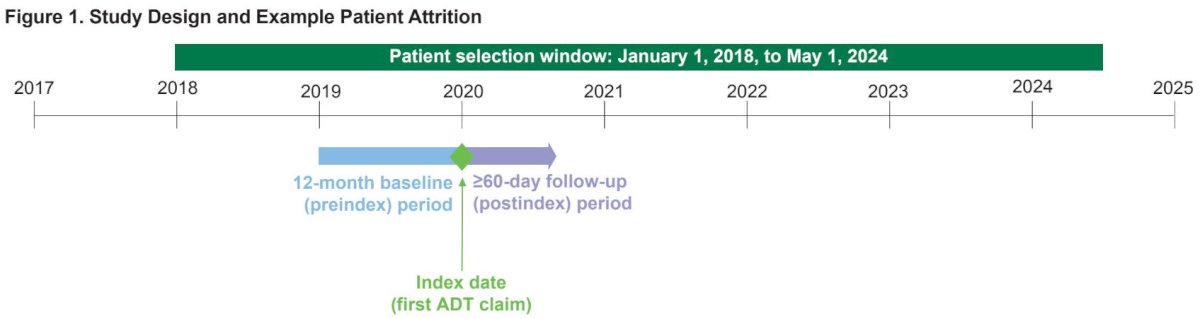
This retrospective observational study utilized data from the Merative MarketScan Commercial and Medicare databases. Men aged ≥40 years with prostate cancer who newly initiated ADT between January 1, 2018, and May 1, 2024, were identified. Eligibility required at least 12 months of continuous enrollment prior to ADT initiation, defined as the pre-index period. Patients were followed for a variable post-index period of ≥60 days, defined by duration of ADT and pharmacy benefits.
ADT exposure was categorized as GnRH agonists, GnRH antagonists, and relugolix. Patients initiating degarelix who switched to a GnRH agonist within 60 days were classified as agonist users, while men remaining on degarelix for ≥60 days were classified as antagonist users. Baseline cardiovascular disease was defined by documented diagnoses of myocardial infarction, cerebrovascular accident/stroke, arterial thromboembolism, unstable angina, or revascularization procedures during the pre-index period.
Outcomes included 2-point MACE (nonfatal myocardial infarction or stroke) and 3-point MACE (nonfatal MI, stroke, or all-cause death), reported per 100 person-years. Statistical analyses were descriptive, with categorical variables summarized as counts and percentages and continuous variables summarized using means and medians.
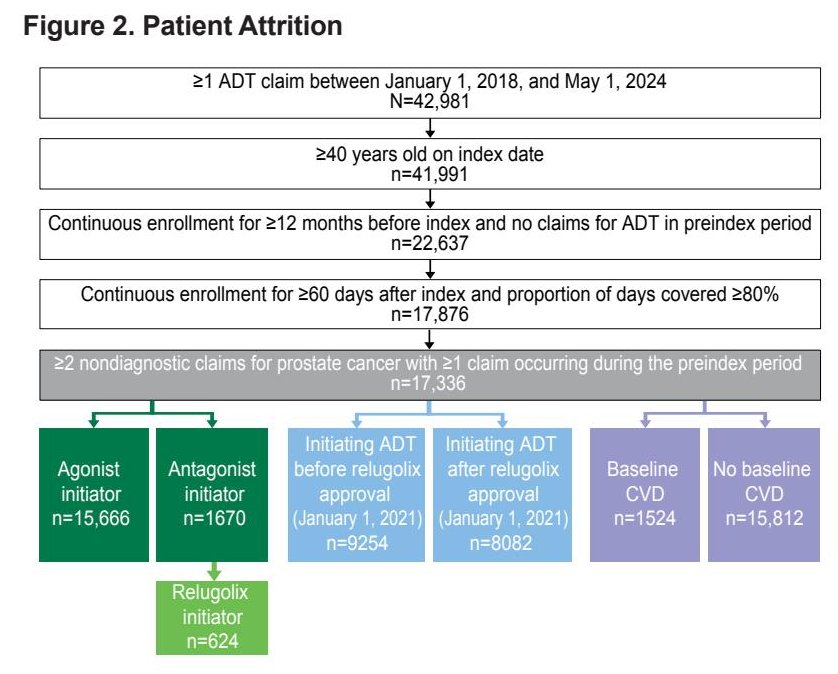
As shown in Figure 2, among 21,681 men initiating ADT during the study period, 17,336 met eligibility criteria for inclusion in the final analysis. Of these, 90.4% initiated a GnRH agonist and 9.6% initiated a GnRH antagonist, including 624 patients who received relugolix. Continuous enrollment criteria and minimum exposure thresholds were applied to define the evaluable population.
The baseline characteristics are summarized in Table 1. Overall, the median age was 69 years. Patients initiating GnRH agonists had a median age of 69 years, while those initiating GnRH antagonists were younger, with a median age of 65.5 years; relugolix initiators were the youngest subgroup (median age 63 years).
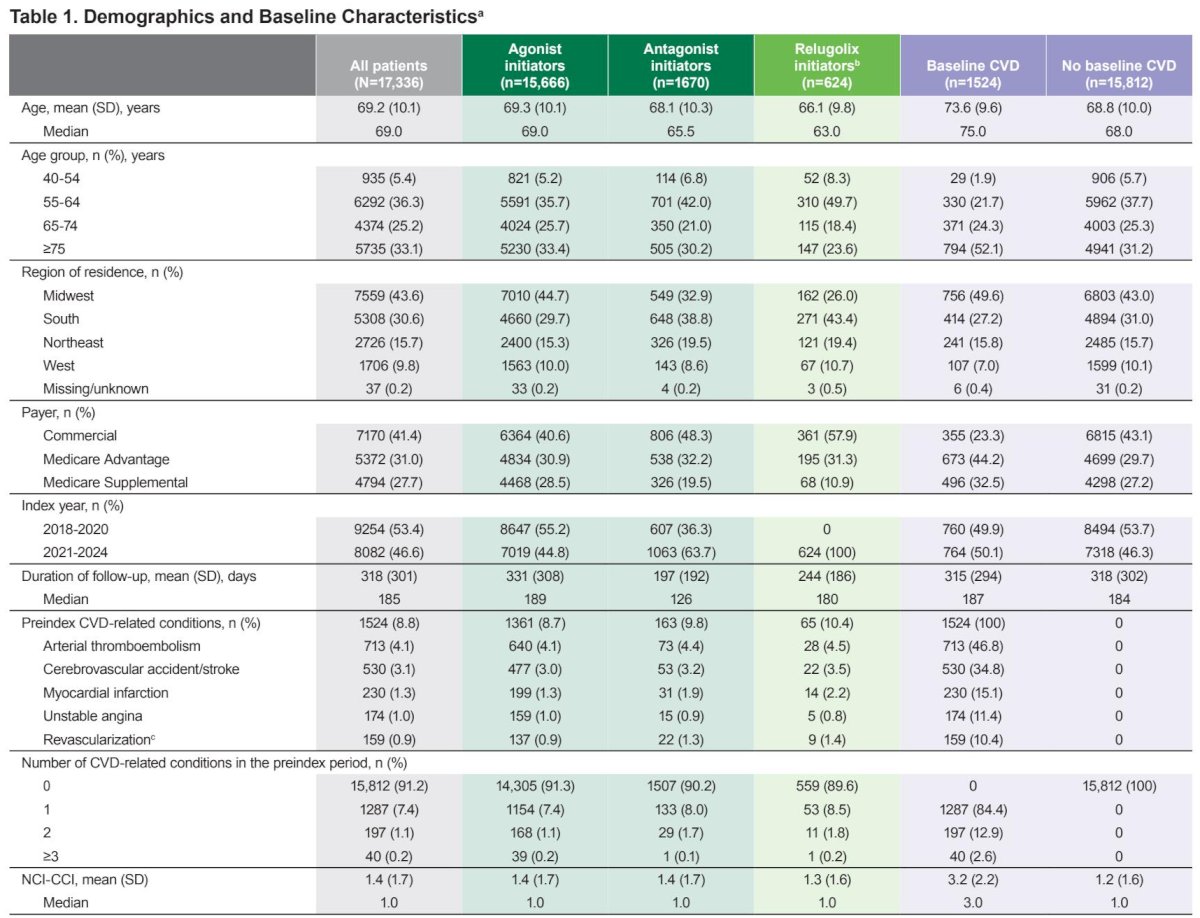
Approximately 69% of patients had baseline cardiovascular disease, with a higher prevalence observed among GnRH agonist users compared with antagonist users. Relugolix initiators were more frequently commercially insured and had shorter median follow-up durations. Geographic distribution, insurance type, and comorbidity burden varied across ADT classes, reflecting real-world treatment selection patterns.
Overall rates of cardiovascular events are shown in Figure 3. Across the entire cohort, the prevalence of 2-point and 3-point MACE during the post-index period was 3.5 and 4.0 per 100 person-years, respectively.
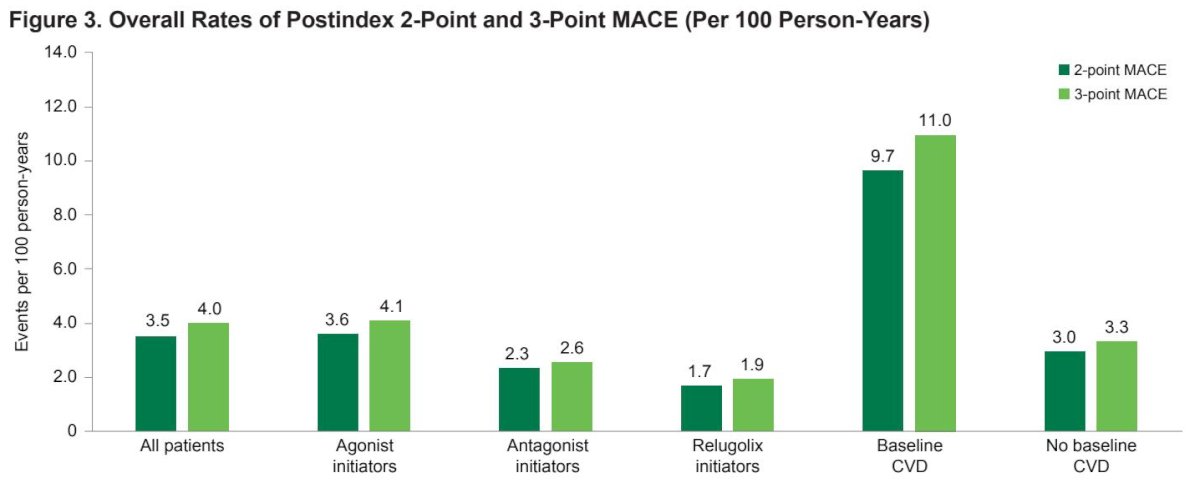
Patients with baseline cardiovascular disease had substantially higher event rates compared with those without baseline CVD. In this subgroup, 2-point MACE occurred at a rate of 9.7 per 100 person-years and 3-point MACE at 11.0 per 100 person-years, highlighting the strong influence of baseline cardiovascular risk on subsequent outcomes.
ADT class–specific analyses demonstrated higher MACE rates among GnRH agonist initiators compared with antagonist initiators. GnRH agonist users experienced 2-point MACE at a rate of 3.6 per 100 person-years and 3-point MACE at 4.1 per 100 person-years, compared with 2.3 and 2.6 per 100 person-years, respectively, among antagonist users.
Relugolix initiators consistently demonstrated the lowest cardiovascular event rates, with 2-point MACE occurring at 1.7 per 100 person-years and 3-point MACE at 1.9 per 100 person-years.
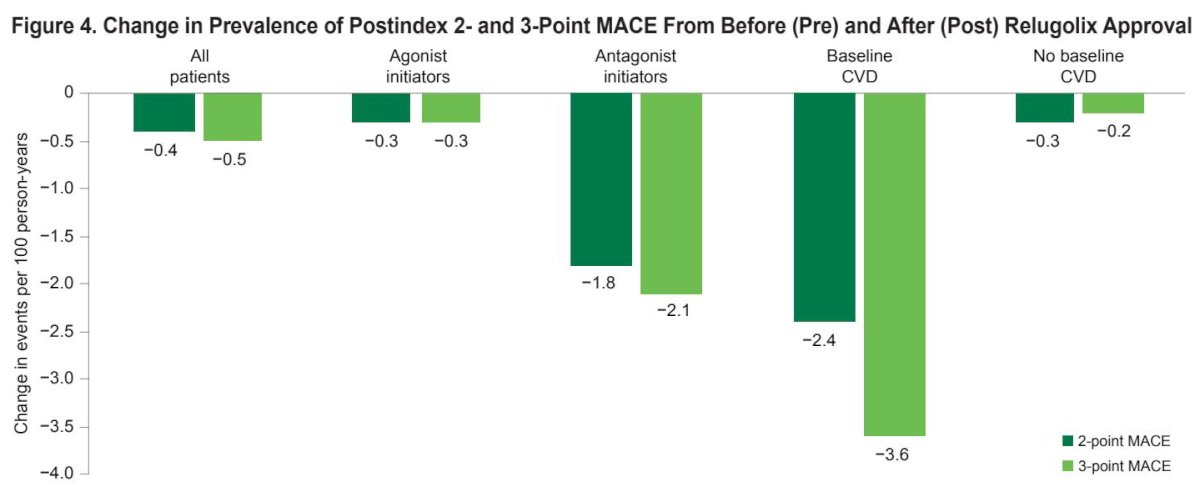
As illustrated in Figure 4, following relugolix approval, reductions in MACE prevalence were observed across ADT classes, particularly among patients with baseline cardiovascular disease. Among patients initiating an antagonist after relugolix approval, 58.7% received relugolix. In men with baseline CVD initiating ADT during this period, relugolix users experienced markedly lower MACE rates compared with GnRH agonist users (3.1 vs 8.8 per 100 person-years).
These findings suggest a shift in ADT selection toward GnRH antagonists, particularly relugolix, among patients at higher cardiovascular risk, which may be contributing to declining MACE rates over time in real-world practice.
These data reinforce the importance of cardiovascular risk assessment prior to ADT initiation and support careful selection of ADT modality, particularly among men with baseline cardiovascular disease. Incorporating cardiovascular risk stratification into prostate cancer treatment planning may help mitigate treatment-related morbidity while maintaining oncologic efficacy.
Dr. Hahn concluded as follows:
- In real-world clinical practice, the prevalence of MACE is low after initiation of ADT
- Although differences in baseline characteristics remain, MACE rates were numerically lower in men receiving GnRH antagonists compared with those receiving GnRH agonists
- Relugolix users were generally younger and had lower rates of MACE
- Use of GnRH antagonists increased following relugolix approval, and with that, awareness and management of pre-existing CVD risk, potentially leading to a decline in MACE rates
- Evaluation for pre-existing CVD or high CVD risk is an important part of prostate cancer management
- Careful choice in therapy, as well as management of underlying CVD, may allow patients and providers to decrease the risk of MACE
Presented by: Andrew Hahn, MD, Assistant Professor, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: ADT Class and Cardiovascular Risk: A Large Retrospective Analysis in Prostate Cancer - Andrew Hahn
References:
- Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005;294(2):238-244.
- Hu JR, Duncan MS, Morgans AK. Cardiovascular effects of androgen deprivation therapy in prostate cancer. Arterioscler Thromb Vasc Biol. 2020;40(3):e55-e64.
- Sumitomo Pharma America Inc. Orgovyx (relugolix) prescribing information. Marlborough (MA): Sumitomo Pharma America Inc; 2025.
- Shore ND, Saad F, Cookson MS. Oral relugolix for androgen-deprivation therapy in advanced prostate cancer. N Engl J Med. 2020;382(23):2187-2196.