(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a prostate cancer poster session. Dr. Rana McKay presented a study of US cancer practices evaluating gaps in BRCA mutation testing among metastatic castration-resistant prostate cancer (mCRPC) patients between 2018 and 2024.
Treatment of mCRPC has advanced with the approval of poly (ADP-ribose) polymerase inhibitor (PARPi) for patients with specific homologous recombination repair gene mutations, including BRCAm. Biomarker-targeted therapy requires timely BRCAm testing, recommended by most clinical guidelines.1-4
Contemporary real-world evidence describing BRCAm testing patterns in mCRPC remains limited. The study investigators evaluated BRCA1/2 testing patterns by mCRPC diagnosis year and factors associated with receipt of testing.
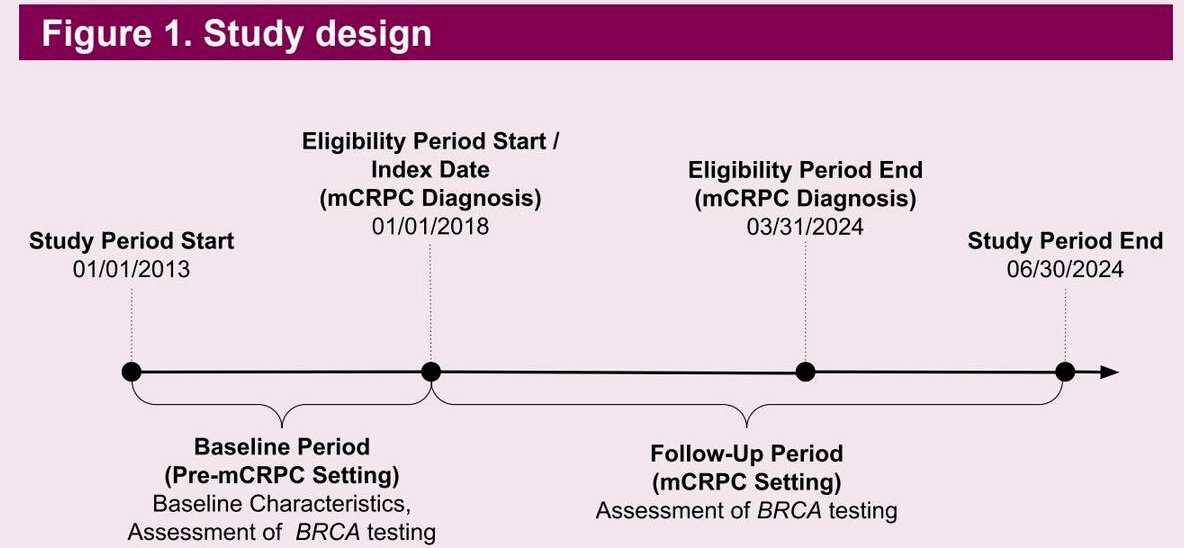
This retrospective cohort study used the Flatiron Health electronic health record–derived database.5 Patients diagnosed with mCRPC between January 1, 2018, and March 31, 2024, were included, while clinical trial participants were excluded. BRCA testing was defined as documentation of somatic or germline BRCA1/2 testing after initial prostate cancer diagnosis. Descriptive statistics characterized testing prevalence by year of mCRPC diagnosis, and multivariable logistic regression evaluated factors associated with receipt of testing based on prespecified clinical and demographic variables.
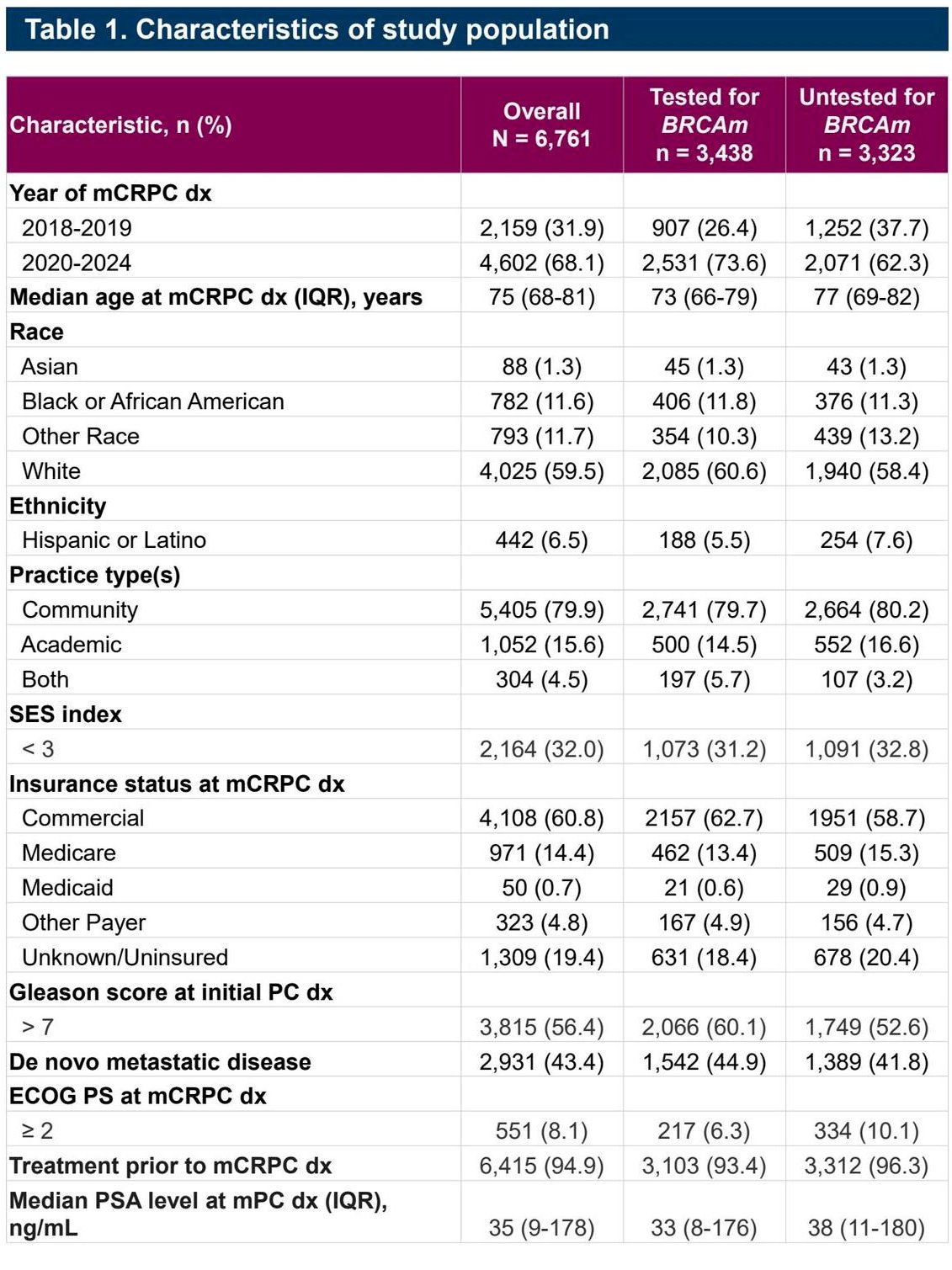
A total of 6,761 patients with mCRPC were included. The cohort was predominantly White (~75–76%), with approximately 80% treated in community oncology practices, reflecting real-world care delivery patterns. The median age at mCRPC diagnosis was approximately 75 years. Roughly half of patients had received prior systemic therapy before mCRPC progression, consistent with contemporary treatment sequencing patterns.
Overall, 51% of patients had documented BRCA testing, meaning nearly half of patients with mCRPC lacked evidence of biomarker assessment during the study period. Temporal analyses showed steady increases in testing uptake:
- 2018: ~37% tested
- 2019: ~46% tested
- 2020: ~53% tested
- 2021: ~54% tested
- 2022: ~56% tested
- 2023: ~57% tested
- 2024: ~56% tested
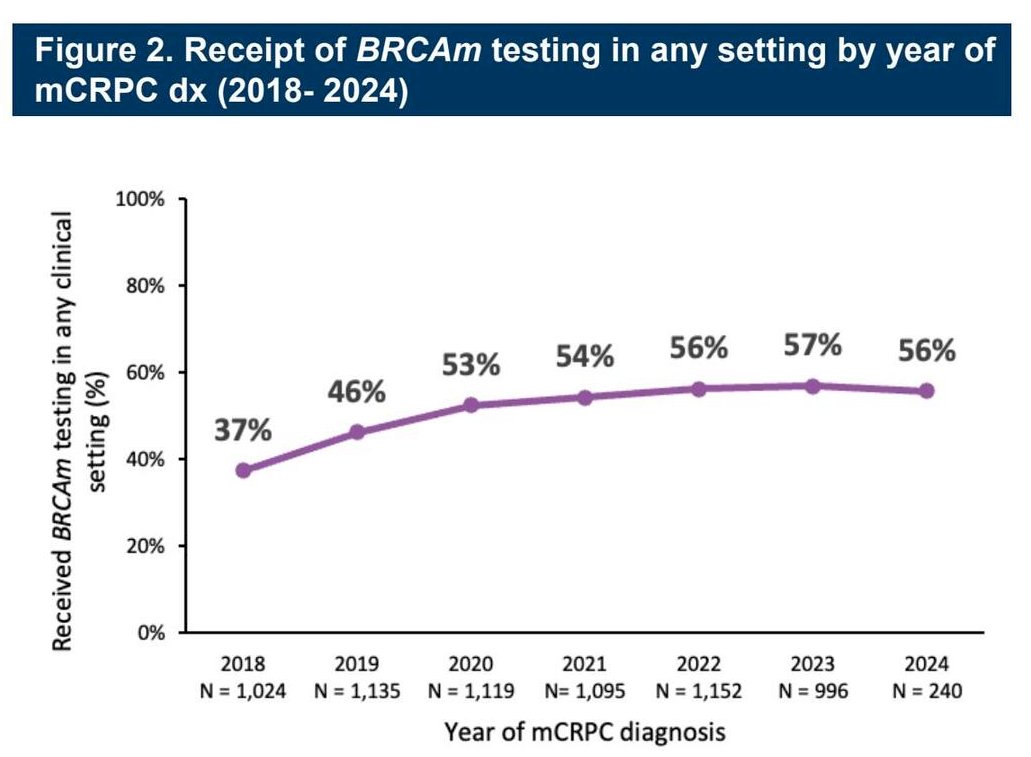
These data demonstrate early adoption followed by a plateau beginning around 2020–2021, with persistent under-testing thereafter.
Among tested patients, testing modality varied:
- 40% somatic-only testing
- 23% germline-only testing
- 36% both germline and somatic testing
- ~0.3% unknown testing type
This variability suggests ongoing inconsistency in implementation of comprehensive genomic testing strategies.
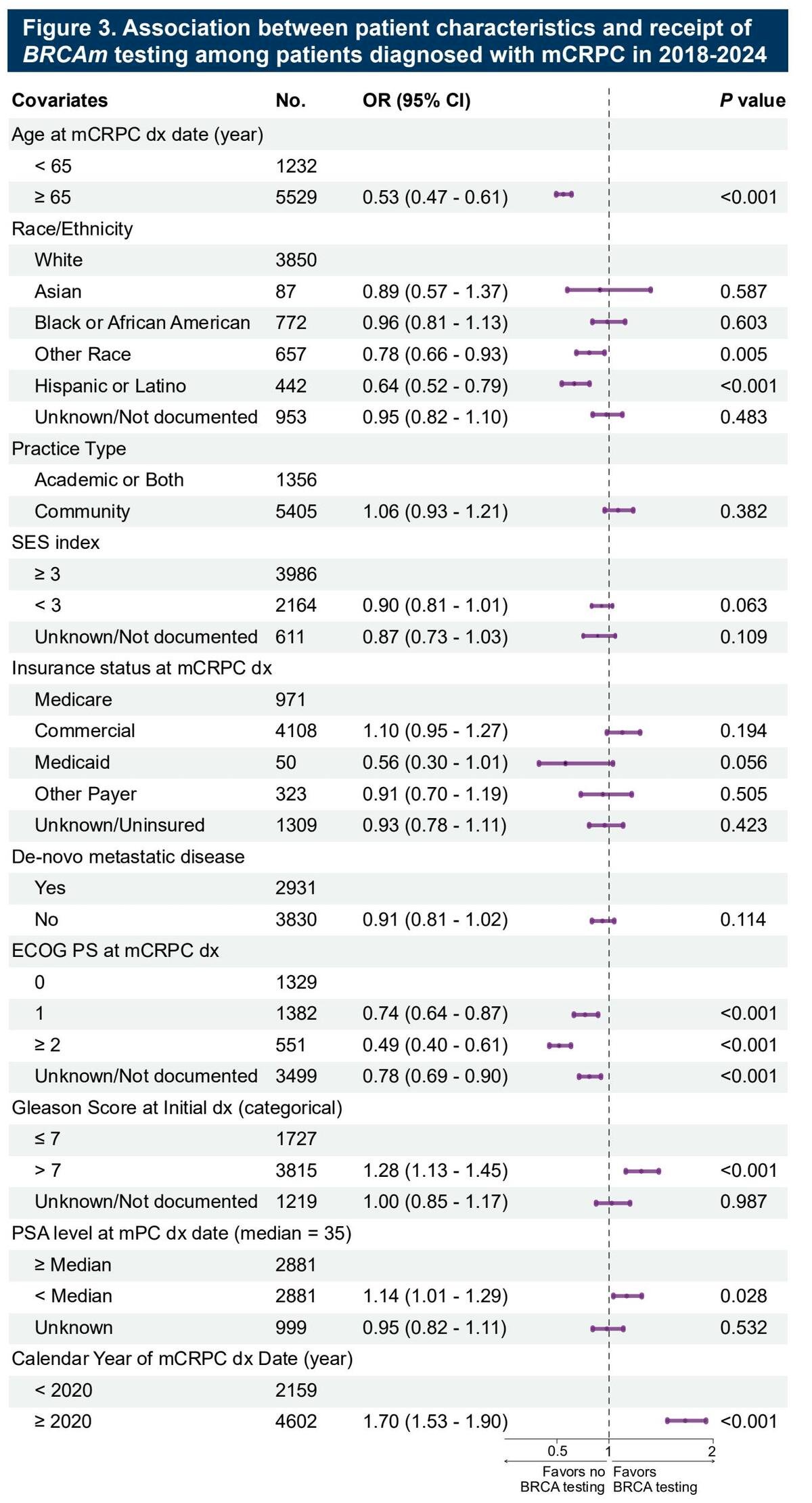
Multivariable analyses identified several predictors of testing. Patients diagnosed in more recent calendar years had significantly higher odds of testing compared with those diagnosed before 2020. Higher Gleason score (≥7), de novo metastatic presentation, and worse ECOG performance status were also associated with increased likelihood of testing. Conversely, some demographic and practice-setting differences persisted, although adjusted analyses showed no statistically significant difference in testing likelihood between White and Black/African American patients.
Importantly, most patients were managed in community oncology settings, highlighting that persistent testing gaps likely reflect system-level barriers rather than isolated institutional practice patterns. Potential contributors include access to testing infrastructure, clinician awareness, reimbursement challenges, and logistical hurdles in coordinating germline versus somatic assays.
From a clinical perspective, these findings are particularly relevant given expanding indications for PARP inhibitors and combination strategies in advanced prostate cancer. Suboptimal testing rates may limit access to effective targeted therapies and clinical trials.
In summary, this large real-world analysis demonstrates that although BRCA testing rates in mCRPC have improved since 2018, uptake plateaued at approximately 55–57% in recent years, leaving nearly half of eligible patients without documented testing. Testing approaches remain heterogeneous, and community practice settings account for the majority of care delivery. These data highlight an ongoing unmet need to optimize biomarker testing implementation to ensure equitable access to precision therapies for patients with advanced prostate cancer.
Presented by: Rana R. McKay, MD, Associate Professor of Medicine, Department of Medicine, University of California San Diego Moores Cancer Center, La Jolla, CA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Barata PC, Sartor O, Garcia JA, et al. Real-world biomarker testing patterns and treatment implications in advanced prostate cancer. JAMA Oncol. 2024;10(7):975-977.
- Clarke NW, Armstrong AJ, Thiery-Vuillemin A, et al. Abiraterone acetate plus prednisone with or without olaparib for metastatic castration-resistant prostate cancer (PROpel): a randomized controlled trial. N Engl J Med Evid. 2022;1(9).
- Chi KN, Agarwal N, Bjartell A, et al. Niraparib plus abiraterone acetate for metastatic castration-resistant prostate cancer (MAGNITUDE): randomized, double-blind phase 3 trial results. Ann Oncol. 2023;34(9):772-782.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer (TALAPRO-2): a randomized phase 3 trial. Lancet. 2023;402(10398):291-303.
- Flatiron Health. Flatiron database characterization: real-world oncology data resource description. Available at: https://flatiron.com/database-characterization