(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the session Treatment Selection, Response Assessment, and Monitoring Across the Spectrum of Advanced Prostate Cancer. Dr. Christopher Sweeney delved into Making Sense of Many Options for Metastatic Hormone Sensitive Prostate Cancer Treatment Selection.
Dr. Sweeney framed his discussion around a central premise: we can make sense of the expanding treatment landscape in mHSPC by thoughtfully harnessing the vast body of data generated through decades of rigorous industry- and investigator-sponsored trials. He emphasized that the field has largely pursued a strategy of delivering maximal doses for the longest possible duration in the broadest eligible populations. While this approach has produced meaningful survival gains, a substantial proportion of patients still derive limited or no benefit. As he noted, “the Wright brothers did not get it right the first time,” underscoring that progress requires iteration and refinement.
He acknowledged that drug development with targeted therapies and companion diagnostics is challenging; however, exposing patients to futile and potentially toxic therapy is an even greater challenge. Dr. Sweeney argued that the field now has a responsibility to translate emerging biologic insights into near-term clinical benefit by advancing biomarker-directed, precision-based treatment selection strategies for patients with mHSPC.
Dr. Sweeney openly acknowledged a personal bias, emphasizing his focus on investigator-initiated studies. He argued that these trials often serve as exemplars within the broader mHSPC landscape, complementing industry-sponsored efforts while offering unique advantages. They typically enroll broader patient populations, including both high- and low-volume disease as well as synchronous and metachronous presentations, and frequently provide extended follow-up of eight years or more. In addition, they are often less constrained by regulatory requirements. As an example, he cited ENZAMET, which permitted concurrent docetaxel as standard of care and used a nonsteroidal antiandrogen such as bicalutamide as the control arm, reflecting real-world practice patterns.1,2
He further highlighted the value of these trials in generating high-impact, reusable datasets. Their relative accessibility enables secondary analyses, hypothesis generation, and the creation of synthetic control cohorts. Importantly, many include rich translational resources, such as archived H&E slides for AI-based pathology, radiographic imaging for radiomics, and banked blood and tumor specimens suitable for germline and tumor whole-exome sequencing, gene expression profiling, SNP arrays, and circulating protein analyses. Together, these resources provide the foundation for biomarker discovery and the development of companion diagnostics, advancing the goal of more precise, personalized treatment selection in mHSPC.
Dr. Sweeney contrasted the simplicity of mHSPC management in 2004, when treatment largely centered on ADT, with the far more complex landscape in 2026. Today, clinicians must navigate multiple intensification strategies, including ARPIs, docetaxel, PARP inhibitors, radioligand therapy, and other targeted agents across different disease states. While this reflects major therapeutic progress, it also underscores the urgent need for biomarker-driven treatment selection to rationally guide care.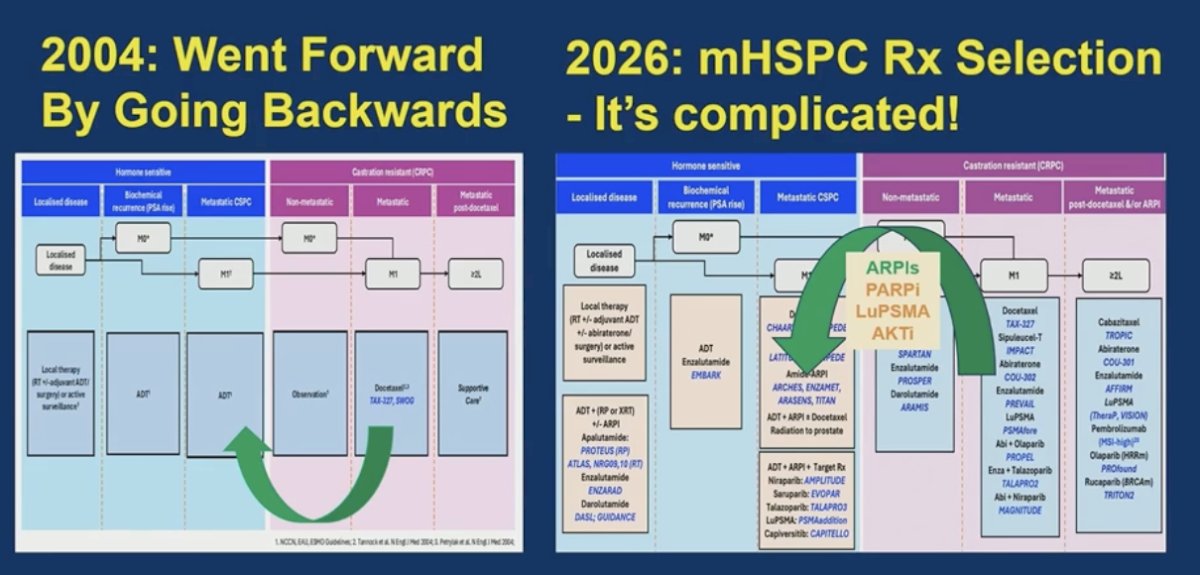
Dr. Sweeney highlighted how far the field has progressed since the 1990s, when 8-year overall survival in mHSPC was approximately 25% with ADT-based approaches. With treatment intensification strategies such as docetaxel and AR pathway inhibitors, 8-year overall survival now exceeds 50% in contemporary trials.1-4 As patients live substantially longer, the long-term consequences of therapy, including cumulative toxicities, have become increasingly important considerations in treatment selection and survivorship planning. A summary slide is shown below.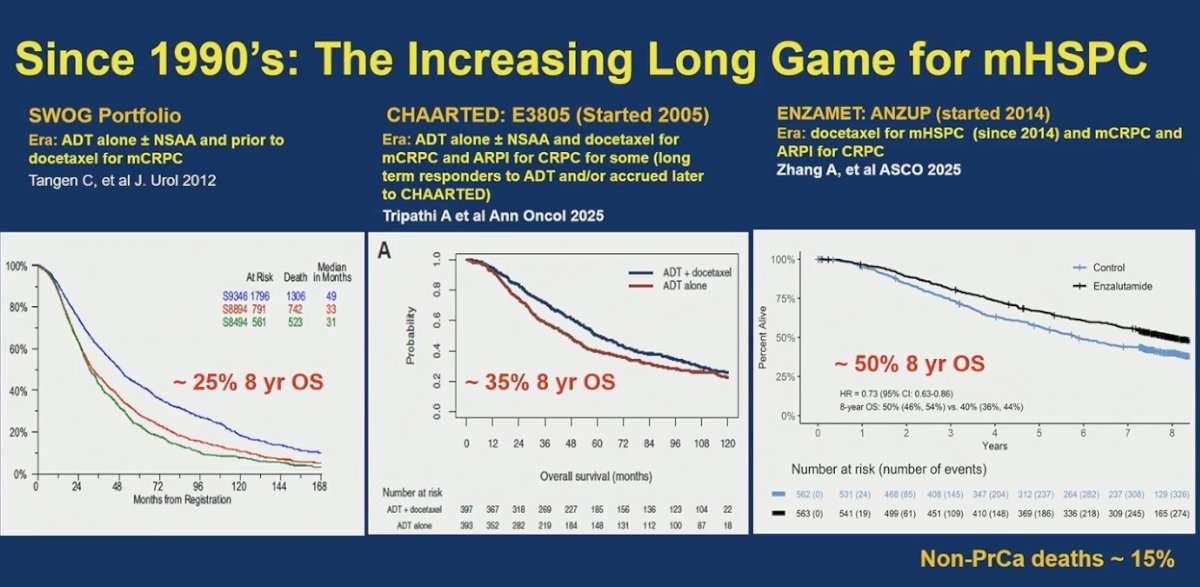
Moreover, Dr. Sweeney emphasized that achieving a PSA <0.2 ng/mL at 6–7 months is a powerful prognostic marker, consistently associated with approximately 50% overall survival at 8 years across modern mHSPC trials. Contemporary studies show higher proportions of patients reaching this deep PSA response, reflecting the impact of upfront treatment intensification. The key question, he noted, is how to further increase the number of patients who achieve early, profound PSA suppression through optimized upfront combination strategies and, ultimately, biomarker-directed patient selection.4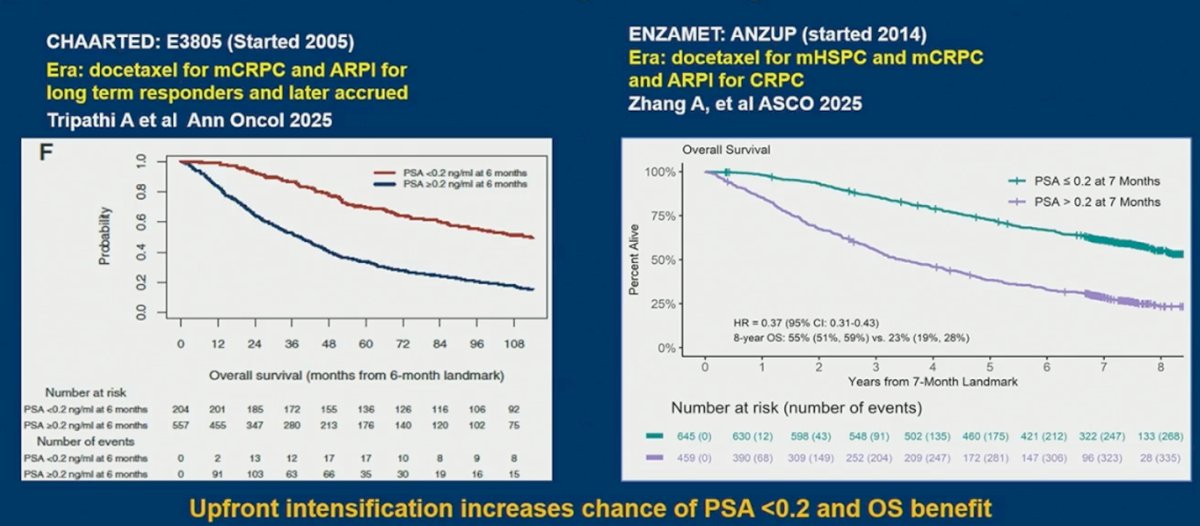
Dr. Sweeney summarized the current state of mHSPC management (Table below) as one in which nearly all patients should receive ADT plus an AR pathway inhibitor, reserving ADT alone only for those with very limited life expectancy. He highlighted APCCC voting patterns that strongly support treatment intensification: 91% favored ADT + ARPI in metachronous low-volume disease (with 68% also supporting SBRT), 84% favored adding docetaxel in metachronous high-volume disease if patients are fit for chemotherapy, 82% supported adding prostate radiation (and SBRT) in synchronous low-volume disease, and 94% favored docetaxel in synchronous high-volume disease. Together, these votes reflect a broad expert consensus around upfront intensification, tailored by disease volume and presentation.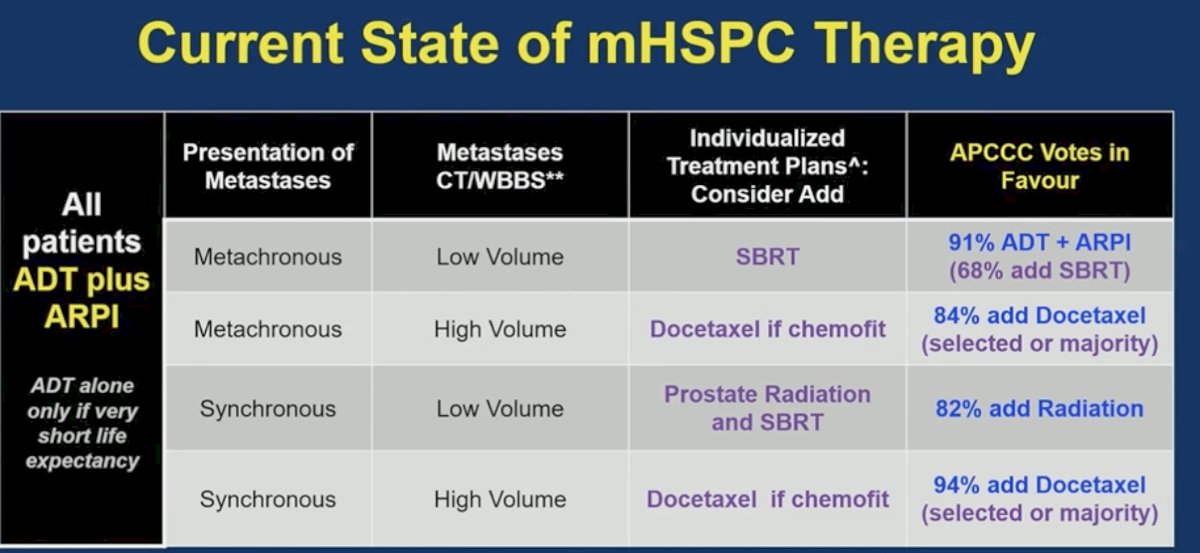
Dr. Sweeney highlighted data from the STOPCAP meta-analysis demonstrating an age-dependent effect with abiraterone in mHSPC. While abiraterone improved overall survival in patients younger than 75 years, the benefit was attenuated in those ≥75 years (HR 1.01, 95% CI 0.82–1.26), with a significant interaction by age (interaction HR 1.56, p=0.001). In contrast, the “amide” ARPIs maintained consistent survival benefit across age groups, including patients ≥75 years, without a significant interaction effect. These data suggest that abiraterone may not be the preferred ARPI in older patients, particularly those over 75.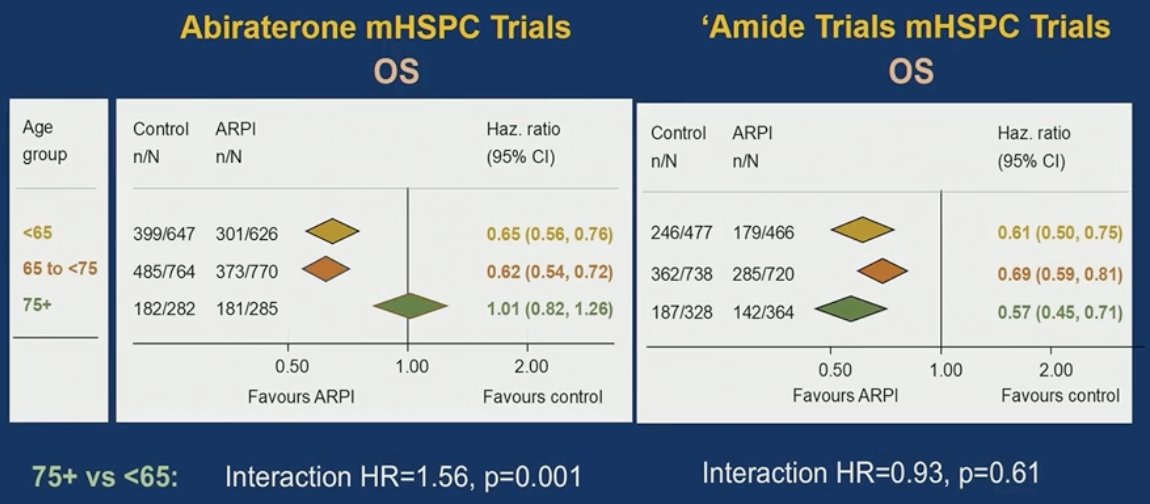
Dr. Sweeney posed the question of where we go next in mHSPC. With ADT plus ARPI now the backbone, the focus shifts to treatment optimization, leveraging biomarkers, including early deep PSA responses, to guide intensification, selection of additional agents such as docetaxel or targeted therapies, and potentially treatment breaks. The challenge is moving beyond a one-size-fits-all approach toward biomarker-directed strategies that identify who needs more therapy, who may benefit from novel combinations such as PARP inhibitors, LuPSMA, or AKT inhibitors, and who may safely de-escalate.
Dr. Sweeney highlighted a model for consensus building grounded in global data sharing and meta-analyses. By integrating results from CHAARTED and subsequent STOPCAP individual patient data meta-analyses, the field was able to identify which patients truly benefit from adding docetaxel to ADT, primarily those with high-volume disease, while demonstrating limited benefit in low-volume populations.1 This collaborative, data-driven approach informed practice, refined patient selection, and allowed the field to move beyond a “docetaxel for everyone” strategy toward more tailored intensification.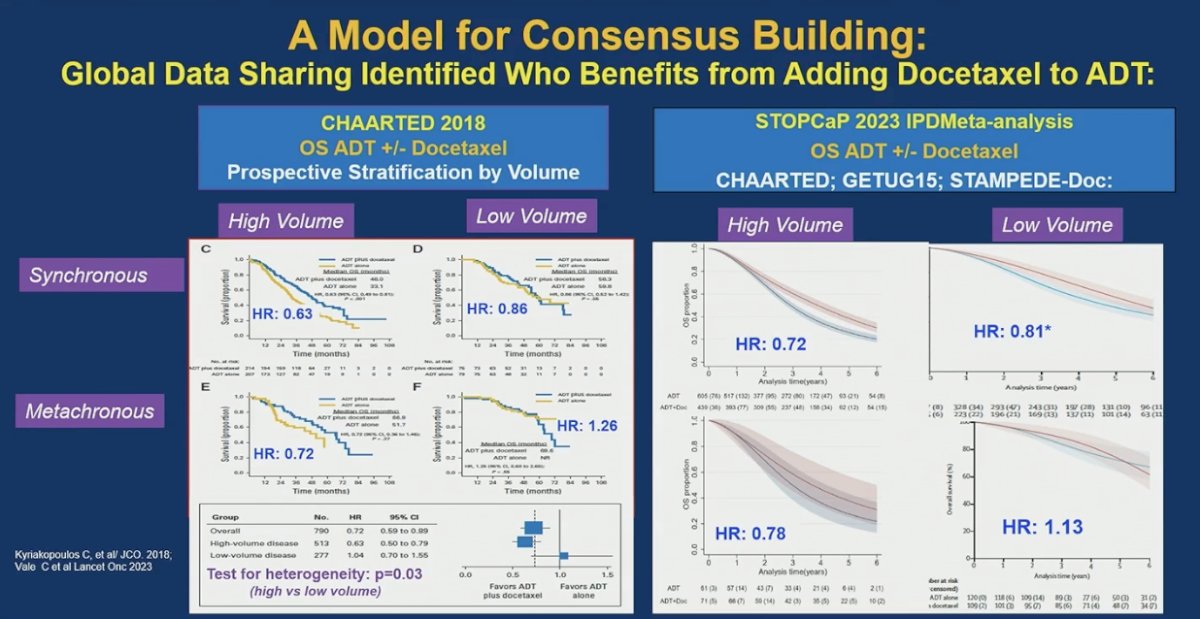
Dr. Sweeney noted that the same global, collaborative model used to define the role of docetaxel in CHAARTED is now being applied to biomarker development. He highlighted Decipher, a 22-gene RNA classifier originally developed in localized prostate cancer and trained on CHAARTED, as a potential tool to refine docetaxel selection. Using samples from STAMPEDE, Decipher appeared predictive for docetaxel benefit, identifying patients more likely to benefit, while not being predictive for abiraterone. This approach represents a step toward biomarker-directed intensification, moving beyond clinical volume alone to molecularly informed treatment decisions.1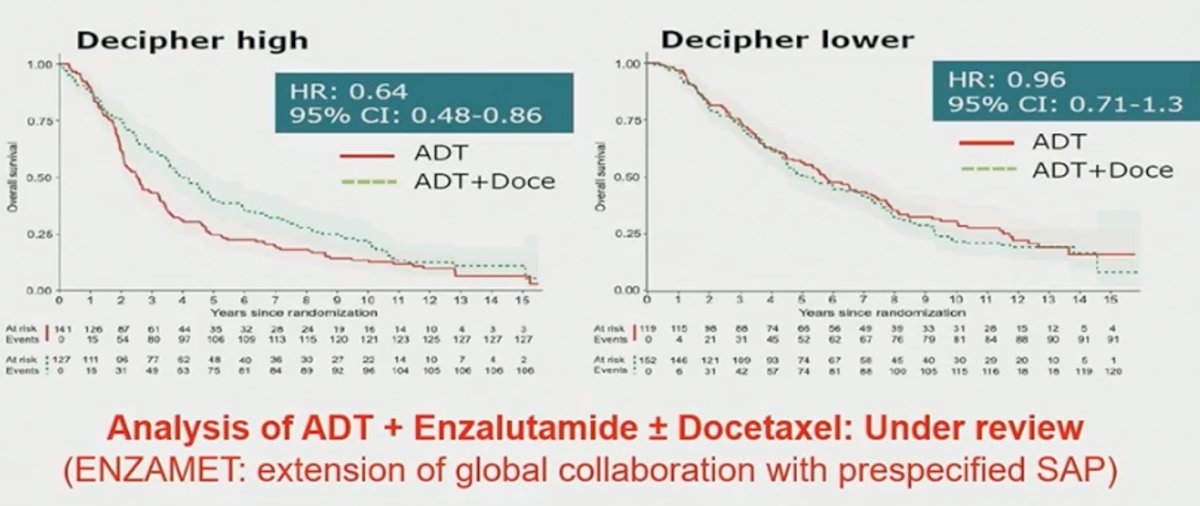
He briefly highlighted several ongoing trials evaluating treatment de-escalation and structured treatment breaks in mHSPC. Studies such as EORTC de-escalation strategies, the phase II Libertas trial, and A-DREAM are exploring whether patients who achieve deep PSA responses (e.g., PSA <0.2 ng/mL) on ADT plus ARPI can safely discontinue or intermittently hold therapy without compromising long-term outcomes. These efforts aim to reduce cumulative toxicity and improve quality of life while preserving disease control in carefully selected patients.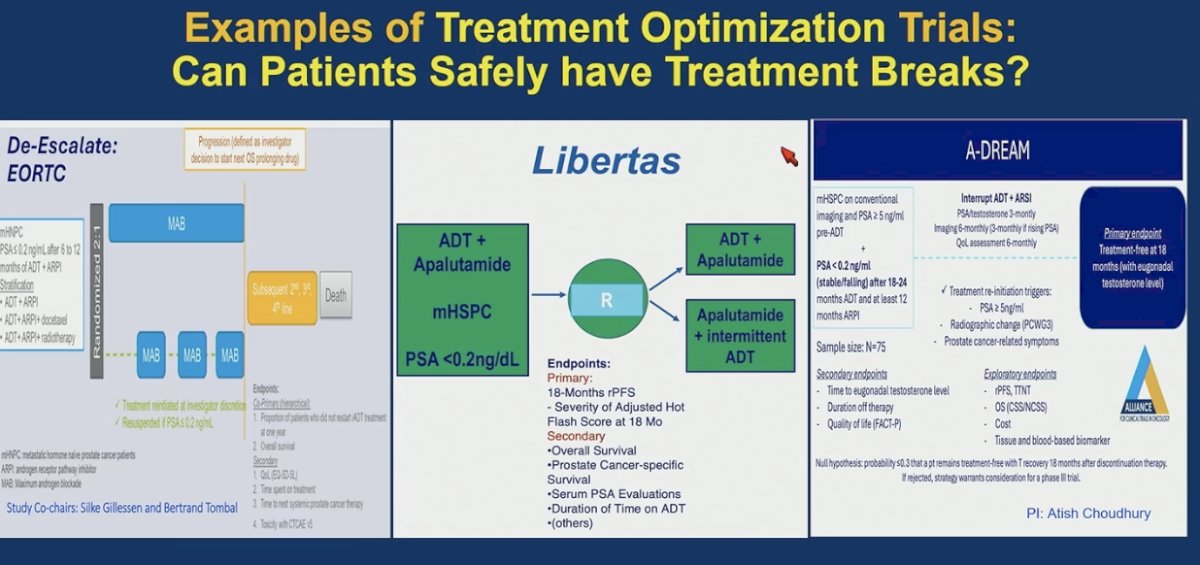
Furthermore, he highlighted ongoing phase III efforts aimed at refining docetaxel selection in mHSPC. Trials such as ASPiRE are evaluating the addition of docetaxel to ADT plus apalutamide in genomically defined or high-risk populations, while CCTG-PR26 (TRIPLE-SWITCH) is incorporating ctDNA-guided strategies to optimize treatment sequencing and better identify patients most likely to benefit from chemotherapy. Together, these studies reflect a shift away from a one-size-fits-all intensification approach toward biomarker-informed personalization of docetaxel use.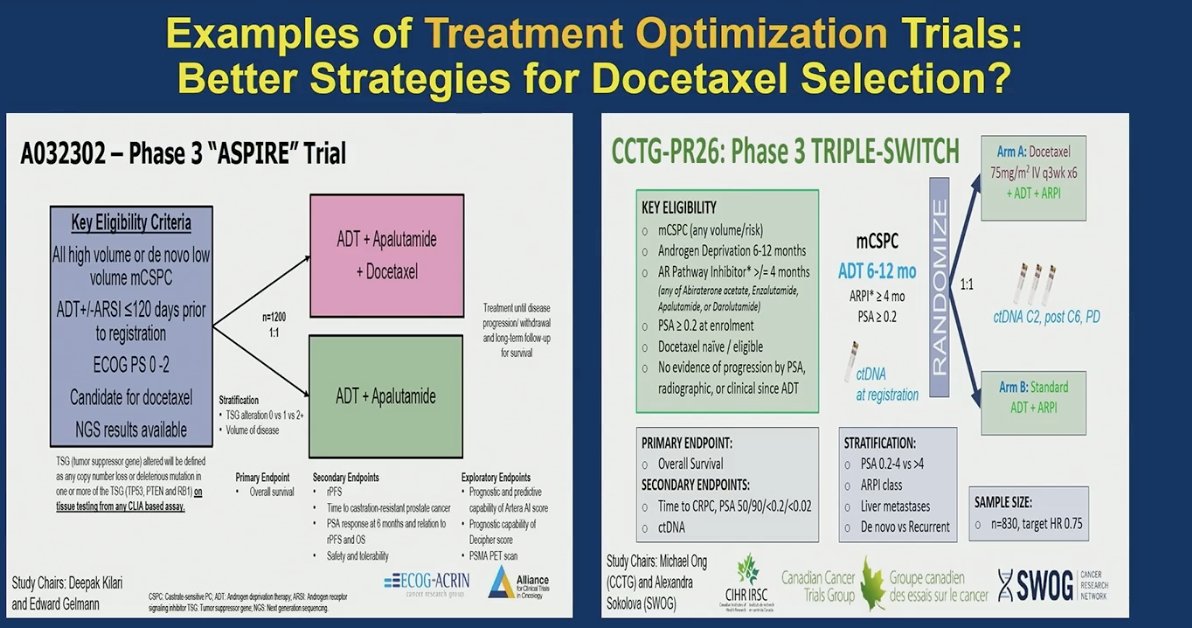
He also reviewed PARP inhibitor data in mHSPC, highlighting results from AMPLITUDE, which evaluated niraparib plus abiraterone and prednisone in patients with HRR alterations. In the BRCA-mutated subgroup, there was a clear rPFS benefit (HR 0.52, p<0.0001), with median rPFS not reached in the niraparib arm versus 26 months with placebo plus AAP. An early OS signal was also observed in BRCA-mutant patients, though not yet statistically significant. Importantly, the benefit outside of BRCA alterations remains uncertain, underscoring the need for biomarker-driven patient selection.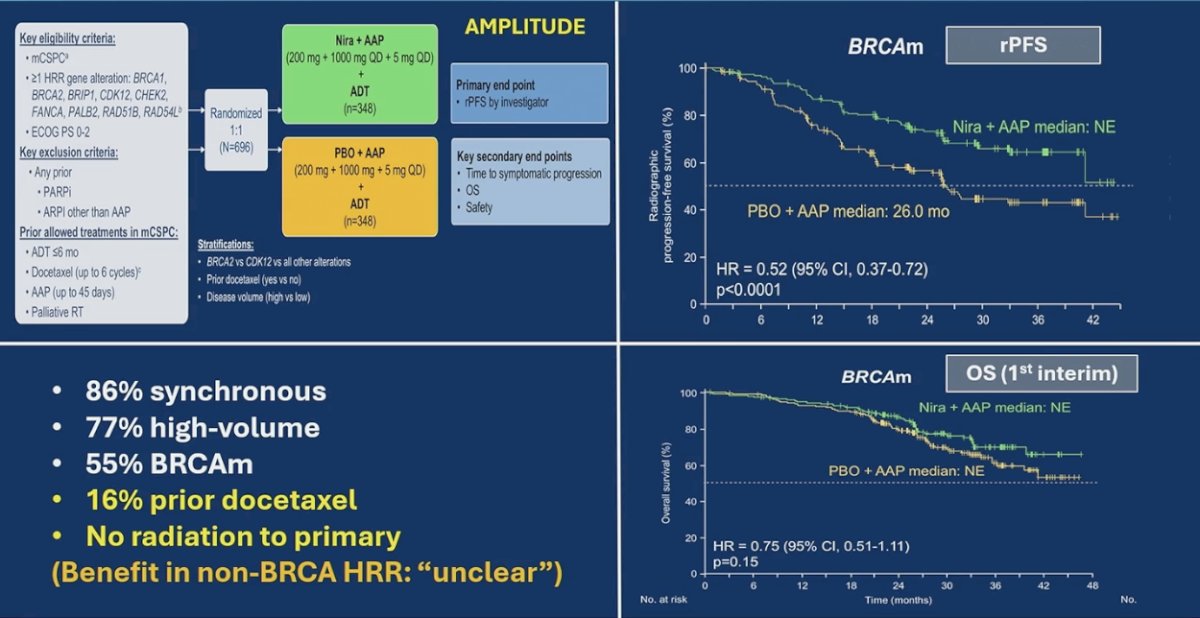
He also discussed PSMAaddition, a phase III trial evaluating the addition of 177Lu-PSMA-617 to ADT plus ARPI in mHSPC. The study demonstrated a significant improvement in rPFS (HR 0.72; 95% CI 0.58–0.90), while the interim OS analysis showed a favorable but not yet statistically significant trend (HR 0.84; 95% CI 0.63–1.13). Notably, patients had no prior docetaxel or radiation to the primary, and a substantial proportion had high-volume and synchronous disease. These data suggest that radioligand therapy may further intensify upfront treatment, although longer follow-up is needed to clarify the overall survival impact.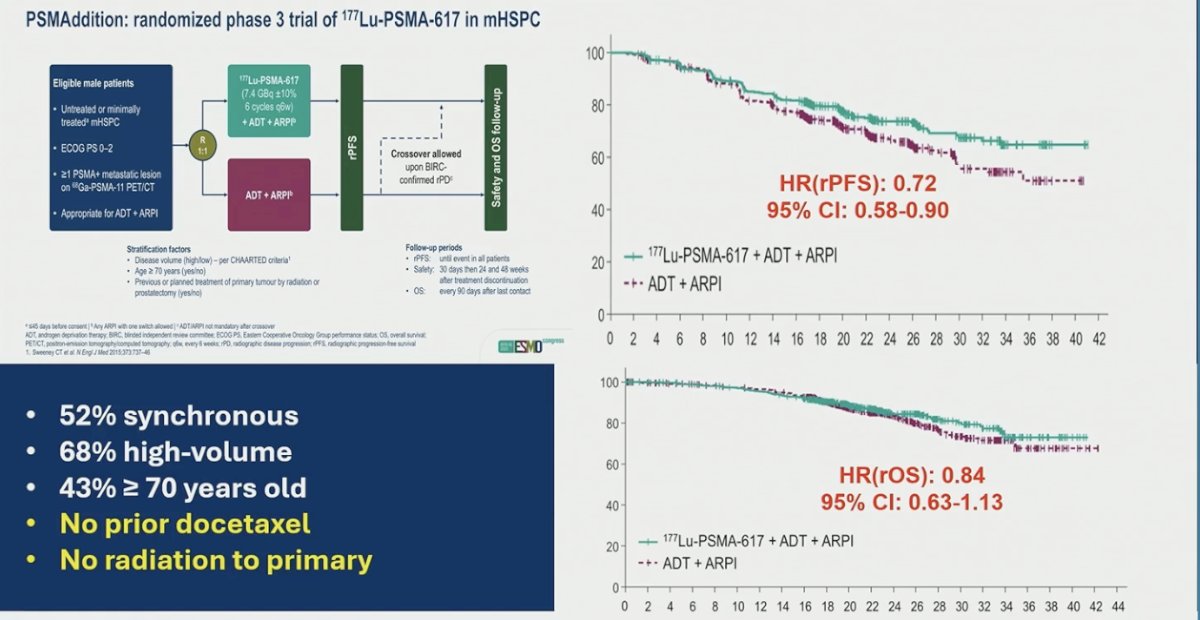
He emphasized the need for better biomarkers to guide LuPSMA use in mCRPC. Data from TheraP and VISION suggest that higher PSMA PET uptake (e.g., SUVmean >10) is associated with longer overall survival compared to lower uptake, indicating that PSMA avidity may help identify patients most likely to benefit, as shown in VISION and TheraP. However, optimal thresholds and clinical integration remain undefined, underscoring the need for prospective validation and biomarker-driven patient selection.5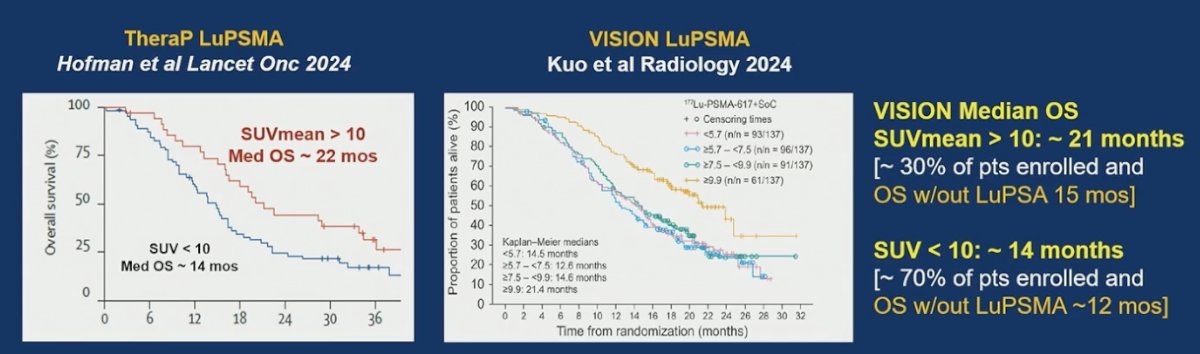
In CAPItello, a large screening effort (n=6566) identified PTEN loss by IHC in a sizable subset, with 1012 patients meeting ≥90% PTEN loss (about 25% of those screened); this was a high-risk population (75% high-volume, 100% synchronous), with no prior prostate radiation or docetaxel. In the most PTEN-deficient group (100% loss; n=303, 4.6% of all screened), the OS signal with AKT inhibition was directionally favorable but not definitive (HR 0.77, 95% CI 0.51–1.14). A logical next step is whether genomic selection could enrich further, such as using NGS to capture PTEN alterations (and potentially pathway co-alterations) that may better identify tumors truly driven by PI3K–AKT signaling and, in turn, increase the proportion of patients with meaningful benefit compared with IHC loss alone.6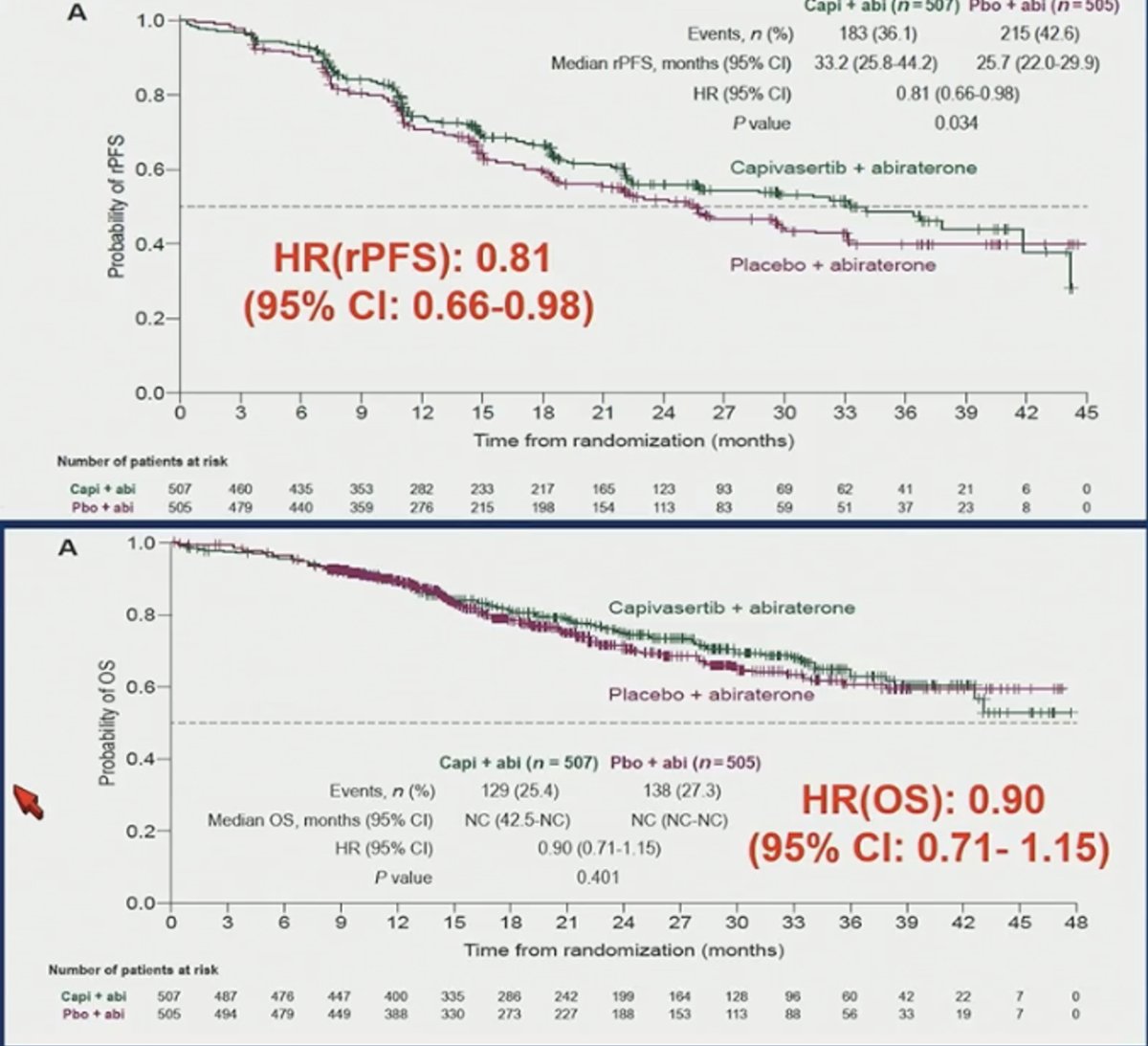
Moreover, he highlighted data from IPATential150 suggesting that PTEN loss by IHC may not be the optimal biomarker for patient selection. While the combination of abiraterone plus ipatasertib improved rPFS in PTEN-deficient tumors defined by IHC (HR 0.77, p=0.034), the overall survival benefit was not clearly demonstrated (HR 0.94), raising concerns about the robustness of IHC-based selection. Dr. Sweeney emphasized that, despite the mixed results, he believes there is a signal in IPATential150 that warrants continued investigation, particularly in better-defined molecular subsets. He noted that AKT inhibition has demonstrated clearer clinical benefit in ER-positive breast cancer, where biomarker-driven selection has been more refined, suggesting that similar optimization of patient selection in prostate cancer may be required to fully realize the potential of this strategy.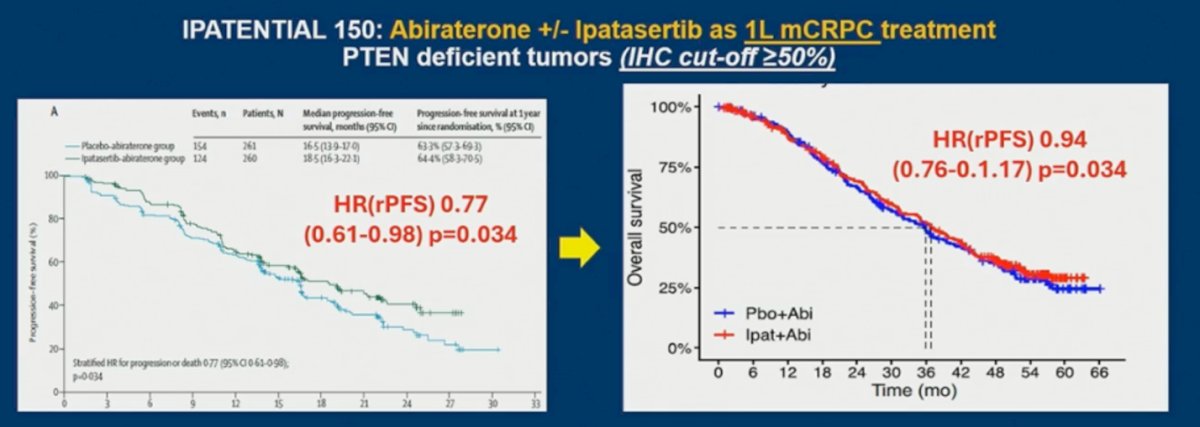
Moreover, he highlighted emerging data suggesting that NGS-defined AKT pathway alterations may be both prognostic and predictive. In IPATential150, patients selected by genomic alterations in AKT, PIK3CA, or PTEN appeared to derive greater OS benefit compared to selection by PTEN IHC alone. He contrasted this with ER-positive breast cancer, where capivasertib plus fulvestrant demonstrated benefit in genomically defined AKT pathway–altered tumors, reinforcing the concept that more precise molecular selection, rather than IHC alone, may better capture patients most likely to benefit from AKT inhibition in prostate cancer.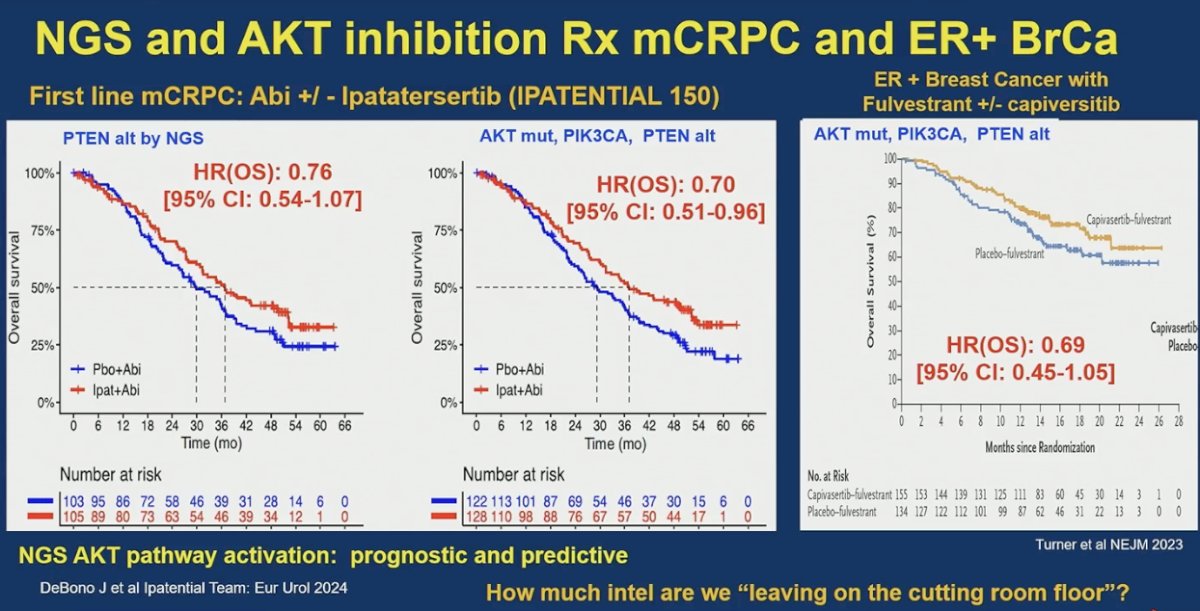
He emphasized that as we intensify therapy with PARP inhibitors, AKT inhibitors, and LuPSMA, understanding quality-of-life impact and potential life-threatening toxicities becomes critical. PARP inhibitors are associated with anemia, fatigue, transfusion burden, and risk of infections and cardiac compromise; AKT inhibitors add diarrhea, rash, and hyperglycemic complications; and LuPSMA commonly causes gastrointestinal distress from dry mouth to intestinal symptoms, often reducing the enjoyment of food. Longer-term risks, including bone marrow and renal effects with radioligand therapy, remain to be fully defined. As survival improves, balancing efficacy with toxicity, functional impact, and patient-reported outcomes is increasingly central to treatment selection. A summary of the AE profile is shown below.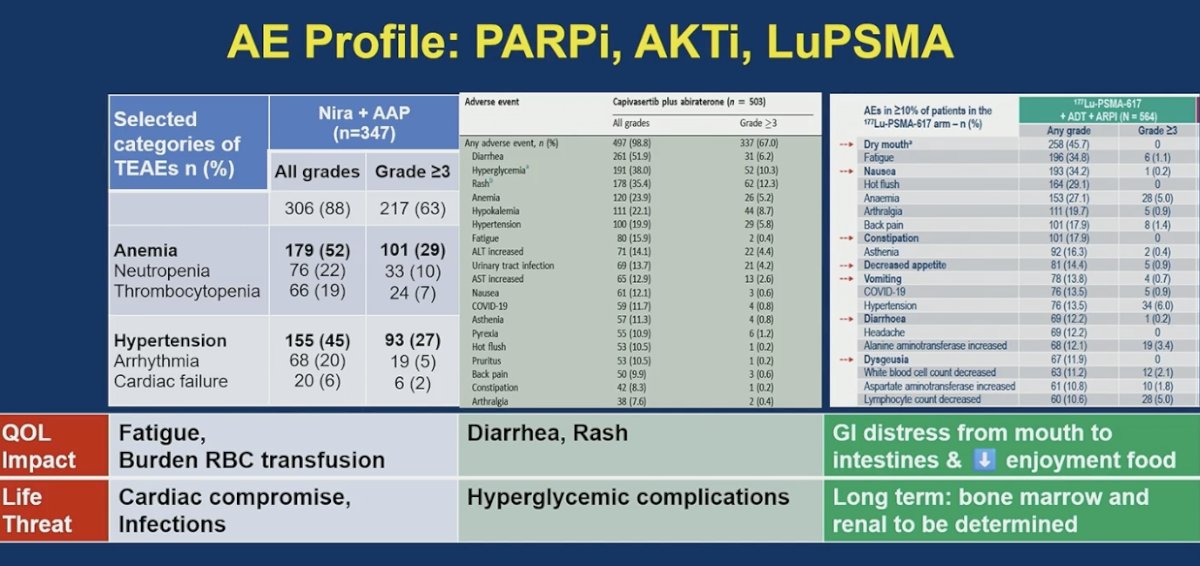
Dr. Sweeney concluded with a high-level perspective on AKT inhibitors, PARP inhibitors, and LuPSMA in mHSPC, noting that it is encouraging to see new data and acknowledging the contributions of both academic and industry investigators. All three strategies demonstrate activity, with modest rPFS improvements and OS hazard ratios below 1.0. However, each approach carries a clinically meaningful adverse event profile and treatment burden. In his view, the magnitude of benefit is not yet sufficient to support routine use in unselected patients, particularly given the likelihood of increased toxicity and attenuated efficacy in real-world settings outside the controlled environment of clinical trials. He emphasized that the path forward lies in optimizing dosing and refining biomarker selection through cooperative group–led studies, guided by the principle of delivering the right drug to the right patient at the right time, for the right duration and dose.
As an example of a forward-looking cooperative group effort, he outlined a proposed phase IV platform strategy. The first step would involve universal upfront ADT plus ARPI for conventional-scan mHSPC, with docetaxel added based on emerging biomarkers and selective use of SBRT and prostate radiation for limited metastatic burden. Following induction, tumors and PSMA PET imaging would guide biology-driven intensification: PARP inhibitors for BRCA-mutated disease, AKT inhibitors for PIK3CA/AKT/PTEN alterations, PD-1 inhibitors for MSI-high tumors, and LuPSMA radioligand therapy for persistent PSMA-avid disease, with alternative strategies for PSMA-negative or genomically high-risk tumors. In the second phase, patients achieving deep responses (PSA <0.1 and PSMA PET–negative at 2 years) could hold therapy with structured monitoring, restarting upon PSA rise, and outcomes compared with biomarker-matched synthetic controls. This framework reflects a shift toward adaptive, biomarker-integrated care across the disease continuum.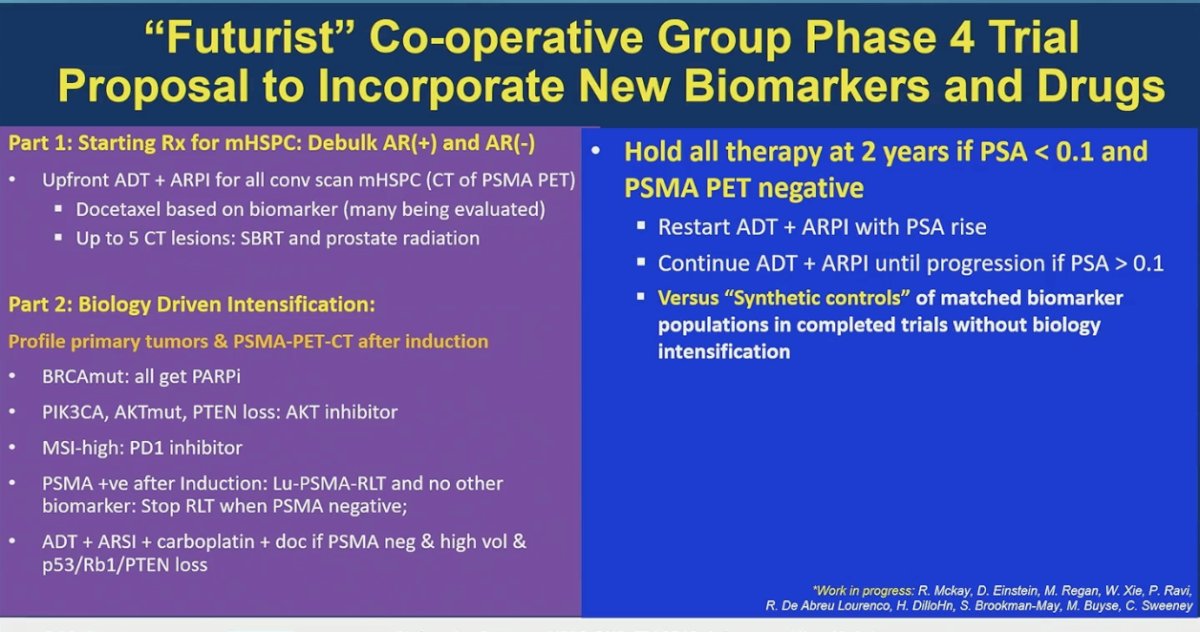
Presented by: Christopher Sweeney, MBBS, South Australian Immunogenomics Cancer Institute, University of Adelaide, Adelaide, Australia
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: Navigating mHSPC Treatment Selection: ADT-ARPI Backbone, Biomarker-Driven Optimization, and the Role of Docetaxel and Targeted Therapies - Christopher Sweeney
- Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, Wong YN, Hahn N, Kohli M, Cooney MM, Dreicer R, Vogelzang NJ, Picus J, Shevrin D, Hussain M, Garcia JA, DiPaola RS. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015 Aug 20;373(8):737-46. doi: 10.1056/NEJMoa1503747. Epub 2015 Aug 5. PMID: 26244877; PMCID: PMC4562797.
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Cheung L, Chi KN, Chowdhury S, Frydenberg M, Horvath LG, Joshua AM, Lawrence NJ, Marx G, McCaffrey J, McDermott R, McJannett M, North SA, Parnis F, Parulekar W, Pook DW, Reaume MN, Sandhu SK, Tan A, Tan TH, Thomson A, Vera-Badillo F, Williams SG, Winter D, Yip S, Zhang AY, Zielinski RR, Davis ID; ENZAMET trial investigators and Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334. doi: 10.1016/S1470-2045(23)00063-3. PMID: 36990608.
- Bossi A, Foulon S, Maldonado X, Sargos P, MacDermott R, Kelly P, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Salem N, Calabro F, Berdah JF, Hasbini A, Silva M, Boustani J, Ribault H, Fizazi K; PEACE-1 investigators. Efficacy and safety of prostate radiotherapy in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2024 Nov 23;404(10467):2065-2076. doi: 10.1016/S0140-6736(24)01865-8. Erratum in: Lancet. 2025 May 10;405(10490):1665. doi: 10.1016/S0140-6736(25)00903-1. PMID: 39580202.
- Mucci LA, Vinson J, Gold T, Gerke T, Filipenko J, Green RM, Anderson SG, Badal S, Bjartell A, Chi KN, Davis ID, Enting D, Fay AP, Lazarus J, Mateo J, McDermott R, Odedina FT, Olmos D, Omlin A, Popoola AA, Ragin C, Roberts R, Russnes KM, Waihenya C, Stopsack KH, Hyslop T, Villanti P, Kantoff PW, George DJ; IRONMAN Global Team. IRONMAN: A Novel International Registry of Men With Advanced Prostate Cancer. JCO Glob Oncol. 2022 Nov;8:e2200154. doi: 10.1200/GO.22.00154. PMID: 36332173; PMCID: PMC9668562.
- Chi KN, Armstrong AJ, Krause BJ, Herrmann K, Rahbar K, de Bono JS, Adra N, Garje R, Michalski JM, Kempel MM, Fizazi K, Morris MJ, Sartor O, Brackman M, DeSilvio M, Wilke C, Holder G, Tagawa ST. Safety Analyses of the Phase 3 VISION Trial of [177Lu]Lu-PSMA-617 in Patients with Metastatic Castration-resistant Prostate Cancer. Eur Urol. 2024 Apr;85(4):382-391. doi: 10.1016/j.eururo.2023.12.004. Epub 2024 Jan 6. PMID: 38185538; PMCID: PMC11859717.
- Fizazi K, Clarke NW, De Santis M, Uemura H, Fay AP, Karadurmus N, Kwiatkowski M, Alvarez-Fernandez C, Jiang S, Sotelo M, Parslow D, Oliveira N, Kwon TG, Ye D, Boudewijns S, Danchaivijitr P, Rooney C, Gresty C, Yeste-Velasco M, Logan J, George DJ; CAPItello-281 Study Group. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study. Ann Oncol. 2026 Jan;37(1):53-68. doi: 10.1016/j.annonc.2025.10.004. Epub 2025 Oct 19. PMID: 41120017.